

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Papillary tumor of the bile ducts is a distinctive pathologic entity characterized by the presence of intraluminal papillary tumors of the intra- and/or extrahepatic bile ducts, and is associated with bile duct obstruction and dilatation (1-4). The latter may be lobar, segmental, generalized, or cystic in appearance depending upon the location of a tumor (Fig. 1). Intraductal papillary tumor of the bile ducts is rare, but probably because of recent developments in diagnostic technology, clinicians and radiologists have encountered increasing number of cases (1). Since it is often misdiagnosed as stones, or remains unrecognized for long periods, the true incidence of the condition is perhaps underestimated (1). In this essay, we describe the radiological manifestations of this disease based on the pathologic findings.
CLINICAL MANIFESTATION
The clinical symptoms and signs of intraductal papillary tumor of the bile ducts are caused by partial or complete biliary obstruction either by a tumor per se, by sloughed tumor debris, or by a copious amount of mucus (1, 5). Diagnosis is usually based on the findings of imaging studies demonstrating bile duct dilatation and intraductal tumors. Because papillomatous tumors are low-grade malignancies, are usually limited to the mucosa, and can invade the ductal wall at a late stage, early diagnosis is important. After surgical resection, a benign course and long survival can be expected (1, 3, 5).
PATHOLOGY
An intraductal papillary tumor is nodular or flat and is characterized by the presence of innumerable, papillary, frondlike infoldings consisting of proliferation of the columnar epithelial cells surrounding the slender fibrovascular stalks supported by connective tissue from the lamina propria (Fig. 2). The tumor often spreads along the mucosal surface but may invade the ductal wall, including its outer surface (1, 3-5). Along the bile ducts, tumors are usually multiple (papillomatosis), involving a fairly wide area of both the intra- and extrahepatic bile ducts (1, 2, 5-7). Histologically, the lesion may be an intraductal papillary adenocarcinoma, adenoma or dysplasia, and various histologic patterns frequently coexist (2, 5). The tumor is friable and sloughs easily, and sometimes produces a profuse amount of mucus, resulting in partial biliary obstruction (5-7).
RADIOLOGICAL FINDINGS
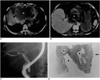
At sonography, CT or MR cholangiography, the bile ducts of the involved hepatic segment, hepatic lobe or entire biliary tree are seen to be dilated. When the tumor involves a segment or one hepatic lobe, the degree of bile duct dilatation is thus particularly severe, and the dilated bile duct appears crowded (Fig. 3). At ultrasonography, an introductal mass is usually echogenic (Figs. 3-5). As it is confined within the bile ducts, the echogenic walls remain intact (2). At CT, an intraductal papillary tumor can appear as a hypo- or isoattenuating soft tissue mass within the dilated duct relative to the hepatic parenchyma, or as segmental thickening of the wall of the bile ducts (3, 4) (Figs. 3 and 4). At contrast enhanced CT, attenuation may be increased, and the outer margin of the thickened bile duct wall is smooth and clear. When it is small and isoattenuating to adjacent hepatic parenchyma, or when complex orientation of the dilated bile ducts obscures the presence of a mass, a tumor is not always depicted (3, 4). At endoscopic retrograde cholangiopancreatography or percutaneous transhepatic cholangiography, the biliary tree is diffusely dilated, and biliary obstruction is usually partial. A tumor may be small and flat, and the ductal wall is sometimes irregular (2-4). A mass reveals fine surface irregularities, either in the form of a velvety or serrated contour, representing the tumor's papillary surface (Figs. 4 and 5). The gallbladder and cystic duct may also be involved (Fig. 5). It is impossible to differentiate benign from malignant papillary tumors solely on the basis of the radiological findings.
VARIANTS
Intraductal Papillary Mucinous Tumors of the Bile Ducts
Some papillary tumors of the bile ducts produce a large amount of mucin (5-7) and may occasionally impede the flow of bile juice, leading to obstructive jaundice. Endoscopy may demonstrate a mucin plug protruding from the patulous orifice of the duodenal papilla (5). In terms of its histopathology and pathophysiology, and the production of excess mucin, this tumor has a striking similarity to intraductal papillary tumor of the pancreas.
Sonography, CT, and MR cholangiopancreatography demonstrate severe dilatation of the intra- and extrahepatic ducts (Fig. 6); both proximal and distal to a tumor are dilated because mucin may obstruct the papilla of Vater. At CT, a tumor may appear as a small, flat mass, isoattenuating to adjacent liver tissue, while mucus is not visible. At sonography, a mucus plug usually echofree but may appear as a masslike, echogenic focus. It is difficult but not impossible to differentiate between a papillary tumor and mucus plugs or stones. Endoscopic retrograde cholangiopancreatography or percutaneous transhepatic cholangiography may demonstrate that the dilated bile ducts contain large or small, multiple, amorphous filling defects caused by mucus plugs (3, 5). The tumor may or may not be visible.
Laputa1 (Floating) Tumors
Intraductal papillary tumors are very friable and slough spontaneously (1). When a tumor grows to a certain size, it sloughs and floats in the bile duct or implants at other sites (papillomatosis) (Fig. 7). The floating tumor may then reside within the bile ducts, imbibing nutrients from bile juice and growing substantially. These sizable, floating tumors may occlude the papillary orifice or escape from the bile duct through the duodenal papillary orifice and then disappear radiologically and clinically. The term, 'Laputa tumor' has thus been coined.
DIFFERENTIAL DIAGNOSIS
Because both diseases caused bile duct dilatation and intraluminal masses or filling defects, intraductal papillary tumors of the bile ducts may be misdiagnosed as recurrent pyogenic cholangitis with bile duct stones. At sonography and cholangiography, mucus plugs or a sloughed (Laputa) tumor may be confused with stones (Fig. 7). Where recurrent pyogenic cholangitis involves focal bile duct stricture, the condition may be misdiagnosed as papillary tumor of the bile duct: both diseases may involve segmental or lobar bile duct dilatation in the absence of an identifiable mass or stone (Fig. 8). Mucinous cystadenoma and cystadenocarcinoma may be mucin hypersecreting and may communicate with the bile duct and may thus be difficult to differentiate from a papillary tumor, especially one that is cystic (7).







 XML Download
XML Download