

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Idiopathic synovial osteochondromatosis is an uncommon benign monoarticular disorder of unknown cause characterized by proliferation and metaplastic transformation of the synovium, where there is cartilage formation (1-3). The knee is the most commonly affected joint, followed by the elbow, hip, and shoulder, although any other joint may be involved (3-15). Patients usually present with pain, swelling, and restricted movement, symptoms which often progress slowly for several years (3). The age range of affected patients is wide, but most present in the fourth or fifth decade of life; men are affected two to four more times frequently than women (3, 11). The condition is usually progressive and leads to early osteoarthritis. Currently accepted surgical treatment involves the removal of any free intra-articular bodies and complete resection of the involved synovium, although local recurrence is not uncommon (1-5, 13, 15).
The radiologic appearance of idiopathic synovial osteochondromatosis depends on the stage of the disease and the extent of calcification or ossification of the cartilaginous nodule (3, 5, 11). Synovial osteochondromatosis that develops within a bursa overlying an osteochondroma may simulate malignant transformation of the osteochondroma (12).
There are scattered reports of idiopathic synovial osteochondromatosis of the hip (13-16), but to more fully characterize the radiologic findings of this condition, with emphasis on the appearance at MRI, the MRI findings of 15 patients were retrospectively analysed.
MATERIALS AND METHODS
Fifteen patients with histopathologically proven synovial osteochondromatosis of the hip were involved in this study. Previously described criteria (2, 3, 5, 17), including the greater number and uniformity in size of intra-articular bodies, and the absence of significant arthritic change, were used to differentiate between idiopathic and secondary synovial osteochondromatosis. The clinical symptoms were hip pain in 14 patients and a painful inguinal mass in one; the duration of these ranged from 6 months to 8 (mean, 3.9) years. Clinical records, pathologic results, and the radiologic findings were reviewed.
The patients [11 men and 4 women aged 20-59 (mean 37) years] underwent hip radiography and MR imaging. For the latter, a 1.5-T (Signa; General Electric Medical Systems, Milwaukee, Wis., U.S.A.) or a 1.0-T imager (Magnetom Impact; Siemens, Erlangen, Germany) was used. Spin-echo T1-weighted (400-700/10-40 [TR/TE]) and fast spin-echo T2-weighted (1500-5000/70-112 [TR/TE]) or turbo spin-echo T2-weighted MR images (3500-4500/80-95 [TR/TE]) were obtained in the axial, coronal, and sagittal planes. Using a field of view of 18-38 cm, two signals were acquired. Section thickness was 5-6 mm and section gap, 1-2 mm.
Hip radiographs and MR images were evaluated by two experienced musculoskeletal radiologists, who reached a consensus. Radiographs were analysed in terms of the presence of 1) juxta-articular calcified and/ or ossified bodies, 2) osteophytes, 3) bone erosion, 4) juxta-articular osteopenia, and 5) joint space narrowing.
For MR images, attention was focused on 1) the configuration of intra-articular bodies, 2) bone erosion, 3) synovial thickening, 4) conglomeration of the intra-articular bodies, and 5) extra-articular extension.
RESULTS
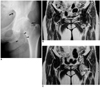
Idiopathic synovial osteochondromatosis was present in the right hip in eight patients, and in the left, in seven. At hip radiography, juxta-articular calcified and/ or ossified bodies were seen in 12 patients (80%) (Figs. 1A, 2A), bone erosion in eight (53%) (Fig. 3A), osteophytes in seven (47%) (Figs. 1A, 2A), juxta-articular osteopenia in five (33%) (Fig. 4A), and joint space narrowing in five (33%) (Fig. 4A). In one patient with bone erosion, this was extensive and circumferential, with scalloping of the femoral neck (Fig. 3).
In our series, no radiographic findings were normal. In the three patients with no juxta-articular calcified and/ or ossified body, other findings such as bone erosion, juxta-articular osteopenia or joint space narrowing were observed, a fact which may be related to the long duration of the disease (mean, 3.9 years).
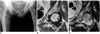
In eight patients (53%), MR imaging depicted intra-articular bodies of focal low signal intensity at all pulse sequences, with areas of iso-intensity at T1WI and hyperintensity at T2WI. In three (20%), intra-articular bodies of focal low signal intensity and areas of hyperintensity at all pulse sequences were observed, with areas of iso-intensity at T1WI and hyperintensity at T2WI. In four (27%), intra-articular bodies of only focal low signal intensity at all pulse sequences were demonstrated. MR imaging revealed synovial thickening in 13 patients (87%) (Figs. 3, 4), bone erosion in 11 (73%) (Fig. 3), conglomeration of the intra-articular lesion in 11 (73%) (Fig. 1), and an extra-articular herniation sac in six (40%) (Figs. 1, 3).
DISCUSSION
Synovial osteochondromatosis is the term used to describe the conversion of synovial connective tissue to cartilage (1, 3, 16). The term idiopathic synovial osteochondromatosis has been used to describe a specific pathological process presenting in otherwise normal joints (3, 16, 20).
The radiographic features of idiopathic synovial osteochondromatosis include calcified and/ or ossified bodies in a joint free of arthritis. If the cartilaginous bodies are neither calcified nor ossified, radiographs may fail to suggest the presence of abnormality, creating a problem in the diagnosis of this condition (4). Associated radiographic features are bone erosion (4), occasional osteoarthritis (4, 16), and regional osteoporosis (4).
In the present study, juxta-articular calcified and/ or ossified bodies, bone erosion, osteophytes, juxta-articular osteopenia, and joint space narrowing were found to be present. In patients with idiopathic synovial osteochondromatosis of the hip, no radiographic findings were normal, though juxta-articular calcified and/ or ossified bodies were absent in three cases, a fact which may be related to the long duration of the disease (mean, 3.9 years). The presence of osteophytes, juxta-articular osteopenia, and joint space narrowing in our series reflects the early osteoarthritic changes occurring in this disorder. In one patient with bone erosion, extensive circumferential erosion with scalloping was found; this aggressive radiographic appearance was related to the presence of a large cartilaginous lesion (Fig. 3).
Our results showed that MR imaging is useful in the diagnosis of synovial osteochondromatosis of the hip, especially in cases in which juxta-articular calcified and/ or ossified bodies are not present.
As expected, the MR characteristics of synovial osteochondromatosis depend on the pulse sequence used and the presence and extent of calcification and/ or ossification (2). Reports have described the MR imaging appearance of hyaline cartilage-containing lesions as distinct, stating that a lobulated lesion of low-to-intermediate signal intensity at T1WI and high signal intensity at T2WI is present (2, 21).
In our study, MR imaging was more sensitive than radiography in the detection of both bone erosion and juxta-articular bodies. The high frequency of synovial thickening at MR imaging, caused by proliferative change in synovial membrane in idiopathic synovial osteochondromatosis (1), was pronounced.
Strikingly, MR imaging depicted conglomeration of the intra-articular lesion in 73% of patients, and the presence of herniation sacs in 40%, findings which were confirmed at surgery. These results are related, we believe, to the fact that the hip joint has a tighter capsule than other joints in the extremity, leading to marked compression of the intra-articular body and increased intra-articular pressure in affected hip joints. Appropriate surgical planning depends on an awareness of this MRI finding.
The present study has several potential limitations. First, radiographic and MR images were interpreted by two observers, via consensus; thus interobserver variability could not be determined. Second, although the methods used by earlier investigators were modified for our study, our analysis of synovial thickening did not involve measurement of the synovium (18, 19). Finally, due to the retrospective nature of the present study, detailed histologic reports that would have allowed better radiographic-pathologic correlation were not available.
In summary, our most common radiographic finding of idiopathic synovial osteochondromatosis of the hip was the presence of juxta-articular calcified and/ or ossified bodies. The MR imaging finding which suggested this diagnosis was the presence of intra-articular bodies of focal low signal intensity at all pulse sequences, with areas of iso-intensity at T1WI and hyperintensity at T2WI. In addition, the presence of an extra-articular herniation sac was not uncommon. These appearances should permit differentiation between idiopathic synovial osteochondromatosis and other causes of intra-articular pathology of the hip joints.


 XML Download
XML Download