

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Barium contrast studies and endoscopy are useful for the evaluation of mucosal surface lesions of the esophagus but provide little information about the extramucosal extent of disease. Computed tomography (CT) and magnetic resonance imaging (MRI), on the other hand, permit the evaluation of wall thickness, mediastinal involvement, adjacent lymphadenopathy, and distant spread. With the advent of the helical technique, CT allows the rapid acquisition of both multiplanar and transaxial images, while MRI permits multiplanar imaging with high contrast resolution. In this article, the authors describe the wide range of imaging and pathologic findings of various benign esophageal lesions.
The Anatomy and Imaging Findings of the Normal Esophagus
The esophagus is a muscular tube, 20 to 24 cm in length, that connects the pharynx to the stomach. It is composed of five layers: two muscle layers (outer longitudinal and inner circular), submucosa, muscularis mucosae, and stratified squamous epithelium which changes abruptly at the cardia of the stomach into simple columnar epithelium. There is no serosal layer. The esophagus has three segments: cervical, thoracic, and abdominal, the first of which lies anterior to the vertebrae and posterior to the trachea. Throughout its course in the posterior mediastinum, the thoracic esophagus is situated adjacent to vital structures including the trachea, vertebrae, lungs, heart, blood vessels, and lymphatics. Its upper third has an intimate relationship with the trachea, while its lower third lies close to the aorta. The abdominal esophagus is usually 3 cm or less in length and connects with the gastroesophageal junction.
In CT imaging of the esophagus, approximately 100-120 mL (30 gm) of intravenous contrast material is usually injected at a rate of 2-3 mL/sec prior to scanning, and for opacification of the esophageal lumen, an esophageal paste (Esopho-CAT; E-Z-Em, Westburg, NT, U.S.A.) may also be ingested. The apparent thickness of the esophageal wall at CT varies according to the degree of distention, and a thickness of 3 mm or more has been considered abnormal (1). According to one study (2), however, in only 4% of normal subjects is the esophageal wall more than 5 mm thick, whereas in 42% its thickness is more than 3 mm prior to dilatation of the esophageal lumen by an effervescent agent. It seems, therefore, that 5 mm, rather than 3 mm, is an appropriate maximum normal value for esophageal wall thickness. At T1-weighted imaging, the esophagus appears as a structure of low signal intensity, contrasted by fat of high signal intensity, while T2-weighted imaging indicates that its muscular wall, which shows moderate enhancement after the injection of intravenous Gd-DTPA, is of low signal intensity.
Benign Esophageal Tumors
Leiomyoma
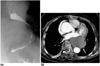
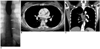
Esophageal leiomyoma is the most common benign esophageal tumor, accounting for more than 50% of all such tumors. Histopathologically, it consists of intersecting bands of muscle and fibrous tissue in a well-defined capsule. About 60% of these tumors are located in the distal third of the esophagus, 30% in the middle third, and 10% in the proximal third (3). Growing slowly, a tumor usually presents grossly as a discrete submucosal mass, ranging from 2 to 8 cm in diameter. Patients with these tumors are usually asymptomatic; even where a large mass significantly indents the lumen, this may be so. Where symptoms are apparent, the most common symptom of these is dysphagia. In contrast to gastric leiomyomas, esophageal leiomyomas rarely ulcerate, and hematemesis is thus extremely rare. Esophageal leiomyomatosis is sometimes associated with Alport syndrome (4).
At chest radiography, a leiomyoma may appear as a mediastinal mass (Fig. 1A), while the mass revealed by barium studies is usually discrete and submucosal. At CT, such tumors usually appear as homogeneous soft tissue lesions (5), though differentiation from other esophageal tumors (fibromas, neurofibromas, or hemangiomas) is difficult (Fig. 1B). MRI usually depicts a submucosal mass which at T2-weighted imaging is isotense to the esophageal wall (Fig. 1C). T2-weighted images of esophageal carcinomas, on the other hand, tend to show that their signal intensity is higher than that of normal esophageal wall (5).
Fibrovascular Polyp
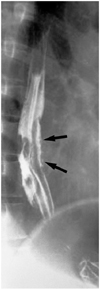
Fibrovascular polyps are rare benign intraluminal submucosal tumor-like lesions characterized by the development of pedunculated, intraluminal masses which in the esophagus can demonstrate enormous growth. Covered with normal mucosa and containing different amounts of fibrous, vascular, and adipose tissue (6) (Fig. 2), they almost always arise from the upper third of the esophagus, near to the cricopharyngeus. On the basis of their histologic composition, these lesions have been termed lipomas, fibromas, fibrolipomas, or fibroepithelial polyps. More recently, they have been classified as fibrovascular polyp, a term used by the World Heath Organization in their international histologic classification system. Dysphagia, vomiting, weight loss, and respiratory symptoms are the most frequent complaints of patients with fibrovascular polyps; these with long stalks, however, can regurgitate into the pharynx or mouth and cause death from asphyxiation if the larynx is occluded (7).
Fibrovascular polyps can sometimes be identified at chest radiography by the presence of a right-sided superior mediastinal mass, anterior tracheal bowing, or both (6). The lesions usually appear at esophagography as smooth, expansile, intraluminal masses that arise in the cervical esophagus and extend into the thoracic esophagus (Fig. 2A). Although most fibrovascular polyps have a site of attachment in the cervical esophagus, barium studies often fail to demonstrate a proximal pedicle. Fibrovascular polyps containing abundant adipose tissue may appear at CT as fat-attenuated lesions that expand the lumen of the esophagus (6) (Figs. 2B, C). Polyps containing equal amounts of adipose and fibrovascular tissue may appear as heterogeneous lesions, with focal areas of fat attenuation juxtaposed with areas of soft-tissue attenuation, and those containing abundant fibrovascular tissue may appear as soft-tissue-attenuated lesions with a paucity of fat. At T1-weighted MR imaging, fibrovascular polyps containing abundant adipose tissue are characterized by high signal intensity (8) (Fig. 2D).
Duplication Cyst
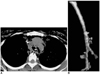
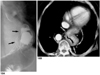
Esophageal duplication cysts account for 0.5-2.5% of all tumors or tumor-like lesions of the esophagus, and about 20% of all gastrointestinal tract duplications (9). They result from abnormal embryologic development in which nests of cells are sequestered from the primitive foregut, and may be classified as either cystic or, less commonly, tubular duplications. Although most duplication cysts are noncommunicating, tubular duplications may occasionally communicate directly with the esophageal lumen (10) (Fig. 3). Most adults with esophageal duplication cysts are asymptomatic, though symptoms caused by obstruction, bleeding, or an infected cyst may occasionally arise.
CT scans of cystic esophageal duplication depict a homogeneous mass with low attenuation and a smooth border (11) (Fig. 4). Kuhlman et al. (11) found that CT can provide information about the cystic nature, size and location of a lesion and allow the use of transesophageal needle aspiration rather than the traditional approach of surgical excision, for definitive diagnosis. CT scans of tubular duplication cysts may show two esophageal lumina, and in the esophageal wall, a thin enhancing rim, representing mucosal linings, may be apparent (10) (Fig. 3A). At T2-weighted MR imaging, duplication cysts may show bright signal intensity and a well-defined margin.
Schwannoma
Esophageal schwannoma is extremely rare; only 15 cases have been reported in the literature (12). A review of these previous reports indicates that benign schwannomas are usually located in the upper esophagus and occur more frequently in middle-aged women. A barium esophagogram reveals a large, smooth, polypoid-filled defect, and CT scans depict a mediastinal mass (Fig. 5). No distinctive characteristics differentiate these from other submucosal tumors, and at preoperative examination it is thus very difficult to distinguish between a schwannoma and other submucosal masses. Correct diagnosis requires histologic examination: positive immunohistochemical staining for S-100 protein and negative staining for smooth muscle markers such as actin and desmin confirm that the tumor originates from a nerve sheath (13).
Infectious and Inflammatory Diseases
Tuberculosis
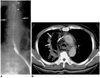
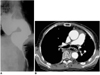
Tuberculosis involving the esophagus usually occurs in the late stages of the disease secondary to pulmonary, mediastinal, or disseminated diseases (14). It has been suggested that CT of the mediastinum provides the most complete depiction of the tuberculous mediastinal lymphadenopathy surrounding and displacing the esophagus and the fistulous tract extending from the esophagus into the nodal mass (Fig. 6). Amorphous gas collection at enlarged mediastinal lymph nodes in patients with tuberculous lymphadenitis suggests the presence of an esophagonodal fistula (14).
Candida Esophagitis
Candida esophagitis is the most common infection of the esophagus, usually occurring opportunistically in patients immunocompromised as a result of underlying malignancy; other debilitating illnesses; treatment with radiation, steroids, or cytotoxic agents; or, most recently, AIDS (15, 16). In the diagnosis of Candida esophagitis, double contrast esophagography shows a sensitivity of about 90% (15), demonstrating discrete plaque-like filling defects which have a finely nodular and granular, distinctive cobblestone or snakeskin-like appearance and correspond to the distinctive white plaques seen at endoscopy. These plaques consist of heaped-up areas of necrotic epithelial debris or actual colonies of C. albicans on the esophageal mucosa; the esophagus per se has an irregular or shaggy appearance (15, 16) (Fig. 7). The CT findings of Candida esophagitis, though nonspecific and commonly seen in various kinds of esophagitis, are circumferential esophageal wall thickening of more than 5 mm, with relatively long segmental involvement. Enhanced scans may also depict the target sign (circumferential wall thickening and enhancing internal mucosa) (2).
Reflux Esophagitis and Barrett's Esophagus
In the diagnosis of reflux esophagitis, the use of double-contrast esophagography has increased radiographic sensitivity to almost 90% (17). Double-contrast imaging reveals the finely nodular or granular appearance of the mucosa in the distal third or half of the thoracic esophagus, occurring due to the presence of mucosal edema and inflammation during the early stages of reflux esophagitis. As the disease progresses, double-contrast esophagography may demonstrate shallow ulcers and erosions, thickened longitudinal folds, inflammatory polyps, scarring, and strictures (18) (Fig. 8).
Barrett's esophagus involves the conversion of squamous epithelium in the distal esophagus into columnar epithelium. The most likely cause of the condition, which occurs in approximately 10% of patients with reflux disease and is premalignant with increased risk of adenocarcinoma (19), is chronic reflux esophagitis. In patients with long-segment Barrett's esophagus, the risk of developing adenocarcinoma is thought to be 30-40 times greater than among the general population (20). The characteristic radiologic feature of Barrett's esophagus is a midesophageal stricture or ulcer, often associated with a sliding hiatal hernia or gastroesophageal reflux (18, 19).
Scleroderma
Patients with scleroderma often develop diffuse interstitial lung disease as well as gastrointestinal symptoms such as dysphagia, regurgitation, and malabsorption. As well as revealing pulmonary parenchymal abnormalities, CT in such patients may demonstrate symptomatic esophageal dilatation and mediastinal lymph node enlargement (22) (Fig. 10).
Trauma and Caustic Esophagitis
Perforation
Perforation is the most serious and life-threatening event to affect the esophagus : in patients with untreated thoracic esophageal perforations, the fulminant mediastinitis which occurs leads to a mortality rate of almost 100%. Endoscopic procedures are responsible for up to 75% of all esophageal perforations (23), which may also be caused by foreign bodies or penetrating trauma. Most perforation involves the cervical esophagus ; spontaneous esophageal perforation (Boerhaave syndrome) due to a sudden, rapid increase in intraluminal esophageal pressure causes full thickness perforation of normal underlying esophageal tissue, and is frequently a result of violent retching or vomiting, usually after an alcoholic binge. Patients with negative esophagograms in whom esophageal perforation is still suspected on clinical grounds may undergo CT ; in such cases, findings of extraluminal gas in the mediastinum are highly suggestive of esophageal perforation (Fig. 11). Where this has occurred, CT is also useful for determining the extent of extraluminal gas and fluid in the mediastinum and for monitoring patients who are treated nonsurgically (24).
Fistulae
Esophageal-airway fistula
In adults, esophageal-airway fistulae are usually acquired lesions. They may occur as complications of tumors or infections and are also caused by trauma. It has been suggested that because it is noninvasive, CT should be the modality of choice for demonstrating their presence (25) (Fig. 12). Owing to the free ingress of air from the airway to the esophagus, the precise locations and size of the communication are outlined by air contrast.
Esophagopleural fistula
Esophagopleural fistulae are usually caused by previous surgery, infection, esophageal instrumentation, radiation, or direct invasion of the pleural space by advanced esophageal carcinoma. The CT findings of esophagopleural fistula include visualization of the fistulous tract, the presence of barium, air and fluid in the pleural space, and pneumonia (26) (Fig. 13).
Caustic Esophagitis
Long, ulcerated strictures may be observed in patients who have ingested lye or other caustic agents, and in severe cases, diffuse esophageal narrowing may reduce the thoracic esophagus to a thin, filiform stricture (27) (Fig. 14A). Cross-sectional images depict narrowing or obliteration of the esophageal lumen, and perifibrotic tissue may be observed (Fig. 14B). Reformatted CT images may be useful for demonstrating the surrounding fibrotic change which caustic esophagitis leads to (Fig. 14C).
Miscellaneous Diseases
Hiatal Hernia
Depending on the relationship between the cardia, the diaphragm, and the herniated portion of the stomach, hiatal hernias are classified as either sliding, accounting for about 99% of all that occur, or paraesophageal. The presence of the former is indicated if single-contrast barium studies performed with the patient in a prone position demonstrate the presence of a lower esophageal mucosal ring (web-like narrowing at the gastroesophageal junction's membranous ridge, covered superiorly by squamous epithelium and inferiorly by columnar epithelium forming the squamocolumnar junction) 2 cm or more above the diaphragmatic hiatus (Fig. 15A). Even in the absence of a definite mucosal ring, a hernia can often be recognized by the presence within it of gastric folds. In paraesophageal hernias, a portion of the stomach herniates through the esophageal hiatus into the chest alongside the distal esophagus, while the cardia retains its normal position below the diaphragm (Fig. 16). Rarely, all or most of the stomach herniates through the esophageal hiatus, producing a gastric volvulus.
Esophageal Diverticulum
Diverticula may be formed either by pulsion due to increased intraluminal esophageal pressure or by traction due to fibrosis in adjacent periesophageal tissue. Pulsion esophageal diverticula, which have a round contour and wide neck, consist only of mucosa, without a muscular layer. Traction diverticula, on the other hand, contain all layers of the esophageal wall, including muscle. Diverticula may be classified according to their location (29), the most common of which are the pharyngoesophageal junction (e.g. Zenker's diverticulum, pulsion type), the middle esophagus (mostly the traction type), and the distal esophagus just above the esophageal hiatus (e.g. epiphrenic diverticulum, pulsion type) (Fig. 17). Because their walls contain no muscle, pulsion diverticula tend to remain filled after the esophagus has emptied of barium. When the esophagus collapses, traction diverticula tend to empty.
Esophageal Achalasia
Achalasia (megaesophagus) arises, in part, because relaxation at the lower esophageal sphincter level has failed to occur, and is partly due to the failure of organized peristalsis. Among the various causes of dilatation of the esophagus, including achalasia, inflammatory stenosis, progressive systemic sclerosis (PSS) and carcinoma, achalasia causes the most severe generalized dilatation. Its symptoms include dysphasia, pain on swallowing, and chronic cough and recurrent pneumonia due to aspiration. Esophagography reveals, typically, that the lower end of the esophagus has a smooth, tapered, beak-like appearance at the level of the esophageal hiatus (Fig. 18A). According to Rabushka et al. (30), who retrospectively reviewed the CT scans of nine achalasia patients, CT demonstrated moderate to marked esophageal dilatation (mean diameter : 4.35 cm at the carinal level), but normal wall thickness (Fig. 18B). Complications in patients with proven achalasia included pulmonary aspiration (three), secondary carcinoma (one), and iatrogenic esophageal perforation (one). It has been reported that secondary esophageal cancer develops in 2-7% of patients with longstanding achalasia (31). Routine CT may not be indicated, but in complicated cases may be invaluable in confirming the diagnosis or in detecting atypical features that may indicate the presence of other diseases or superimposed benign or malignant processes.
Esophageal and Paraesophageal Varices
In patients with underlying hepatic disease, the most common cause of esophageal and paraesophageal varices is portal hypertension, which leads to hepatofugal venous flow within esophageal or paraesophageal collateral vessels. Downhill varices associated with superior vena caval obstruction have also been reported (32). CT is useful in demonstrating the presence and extent of varices (33, 34) (Fig. 19), the appearance of which varies according to the severity and extent of the disease. At unenhanced CT, thickening of the esophageal walls may be visible, which enhanced CT reveals enhancing structures within the esophageal wall or periesophageal region (33, 34).
CONCLUSION
The role of cross-sectional imaging in the evaluation of benign esophageal lesions continues to evolve. The advent of helical computed tomography and its volume data set facilitates the acquisition of multiplanar images; magnetic resonance imaging also helps acquire such images, as well as permitting tissue characterization. Through an awareness of the detailed morphology, location and extent of various benign esophageal lesions, as demonstrated by multiplanar cross-sectional imaging, the radiologist can play a more important role in the detection, diagnosis, and treatment of the diseases described in this paper.












 XML Download
XML Download