

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Pericallosal lipomas are congenital brain tumors occurring in the fetus. Though now more common than before, articles describing their presence have been few, and the tumors are rare (1-4). At obstetric ultrasound these lesions usually present as solid, well-marginated, hyperechoic masses within the interhemispheric fissure along the corpus callosum. A recent report by Ickowitz et al. (2) described their experience with fetal MR imaging of a pericallosal lipoma. We present a case of prenatally diagnosed pericallosal lipoma located at the anterior interhemispheric fissure and associated with agenesis of the corpus callosum.
CASE REPORT
A 3.5-kg female neonate with a gestational age of 39 weeks was born by normal delivery to a 34-year-old woman whose pregnancy had been unremarkable until the 20th week. Ultrasonography at 20 weeks' gestation revealed mild dilatation of the occipital horns of the lateral ventricles. No other fetal abnormalities were noted. Follow-up ultrasound at 26 weeks' gestation depicted a well-circumscribed echogenic mass measuring about 13 mm within the anterior portion of the interhemispheric fissure (Fig. 1A). The posterior horns of the lateral ventricles were mildly dilated to 11 mm, but the frontal horns were not dilated and were more laterally positioned. The cavum septi pellucidi was not visualized. Ultrasound examinations repeated at 30 and 35 weeks' gestation showed that the lateral ventricles measured 16 mm and 20 mm, respectively: at the most recent examination, the mass had increased in size to 16×28 mm. Fetal growth was normal.
Fetal MR imaging, also performed at 35 weeks' gestation, showed that the mass was 28 mm in size; high signal intensity and the lesion's resemblance to maternal subcutaneous fat was revealed by T1-weighted imaging (Fig. 1B), while T2-weighted imaging demonstrated intermediate intensity (Fig. 1C). A fat-suppressed T1-weighted MR image (Fig. 1D) showed complete cancellation of the signal intensity of the mass, a finding consistent with fatty mass. MR images also revealed agenesis of the corpus callosum and colpocephaly; the occipital, but not the frontal, horns of the lateral ventricles were dilated.
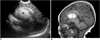
The findings of a post-delivery neonatal neurological examination were normal, but sagittal neurosonography revealed the presence of a midline echogenic mass with scattered echogenic spots in the cingulate sulcus (Fig. 2A). A sagittal T1-weighted MR image depicted a high-signal-intensity bulky mass in the midline of the anterior pericallosal area (Fig. 2B). Fat globules were scattered along the cingulate sulcus, and agenesis of the corpus callosum was also noted. The cerebral gyri extended in a radial pattern from the lateral ventricles without the normal curve of the cingulate gyrus. The neonate was discharged at 4 days of age.
DISCUSSION
Intracranial lipoma is a rare congenital malformation with a prevalence at autopsy of 1:1700 (5). With the increasing use of obstetric sonography, the frequency with which this lesion is discovered in the fetus is growing. Pericallosal lipoma is usually located within the interhemispheric fissure along the corpus callosum (6), and on the basis of MR imaging findings in adults and children, these lesions are classified as one of two types (2, 3, 6). The tubulonodular form is round, more than 2 cm in size, and is usually located at the genu area of the corpus callosum. The second form, on the other hand, is curvilinear; thin and elongated, it is less than 1 cm in diameter and is usually found more posterior to the corpus callosum. The former has been more often associated with congenital anomalies than has the latter. In our case, the lesion was located along the genu area of the corpus callosum, which was not defined. However, because of the lipoma, direct sonographic visualization of the callosal anomaly in utero may be difficult. Indirect signs such as colpocephaly and the absence of the cavum septi pellucidi suggest possible callosal dysgenesis. In our case, the occipital horns of the lateral ventricles were enlarged and the cavum septi pellucidi was not visualized.
The pathogenesis of a pericallosal lipoma is believed to be the result of abnormal resorption of the primitive meninx, a phenomenon which usually occurs between the eighth and the tenth week of development (2). When the primitive meninx is not resorbed, it differentiates into lipomatous tissue. Lipomas of this kind may develop in all the cerebral cisternae, but are much more frequent in the area of the corpus callosum, where they interfere with its normal growth. For this reason, developmental anomalies of the corpus callosum almost always coexist; the degree of anomaly appears to correspond to the size and location of the lipoma (2, 6).
Pericallosal fetal lipoma is usually reported during the third trimester, but has become increasingly common during the second (1, 2). Obstetric sonography reveals the characteristic features of a lipoma: a nodular or curvilinear echogenic mass within the interhemispheric fissure. Color Doppler US may demonstrate the presence within the mass of anterior cerebral arterial branches (4). The differential diagnosis of a lipoma includes intrauterine intracranial hemorrhage, teratoma, and other intracranial tumors such as fat-containing dermoid and epidermoid cysts (1, 2, 7). Hemorrhage is usually found within the hemispheres or germinal matrix, and at follow-up ultrasonography rapid changes in the lesion's size and morphology are observed. Teratomas are usually complex echogenic masses which at ultrasonography are seen to have solid, cystic components. Fat-containing dermoid and epidermoid cysts are found near the midline and usually occur in adults.
Ickowitz et al. (2) recently described their MR imaging findings of intracranial fetal lipoma, reporting high signal intensity at T1-weighted MR imaging and intermediate signal intensity at T2-weighted. For characterization of the tissue content of a lipoma, fat-suppressed T1-weighted MR imaging is very useful.
The prognosis for a fetus with a prenatally diagnosed intracranial lipoma depends more on the associated anomalies than on the callosal agenesis itself. Other defects described in association with pericallosal lipomas include midline defects (cleft lip or palate, median cleft nose, hypertelorism, cerebellar vermis defects, frontal lipomas) and dysraphism (myelomeningocele, encephalocele, anomalies of the cervical spine, cranium bifidium, or other calvarial defects) (1). A few articles have described the occurrence of lipomas of the corpus callosum in association with Goldenhar syndrome (oculoauriculovertebral syndrome) (8, 9), and associated cardiac defects and trisomy 21 have also been reported (10). In addition to the structural abnormalities previously noted, children may manifest seizure activity, mental retardation, headaches, behavioral changes, or vertigo (1, 2), though our patient had only agenesis of the corpus callosum, with normal findings at neonatal neurological examination. Due to late-developing neurological symptoms, however, careful follow-up evaluation may be needed.
In summary, an echogenic mass within the interhemispheric fissure of a fetal cerebrum could be a pericallosal lipoma, and fetal MR imaging may help diagnose and characterize the tumor and its associated anomalies.

 XML Download
XML Download