

 PDF
PDF ePub
ePub Citation
Citation Print
Print


MR spectroscopy (MRS) has been used in the diagnosis and characterization of many disease processes, including breast diseases, as a noninvasive method which can provide in-vivo data on human biochemistry and pathophysiology. 1H, 13C, 14N, 19F, 23Na and 31P have been used in MRS (1, 2), 1H and 31P being used most widely. 31P MRS is especially suitable for breast studies, more so than 1H because water suppression is not essential and there is a relative lack of phosphorus metabolites in normal breast tissue (3). The use of 31P MRS for brain, heart, muscle and liver studies (1, 4-5), as well as for diagnosing breast diseases (3, 6-25), has already been reported in the literature. However, the results have varied because of differences in the design, materials, and methods of the various studies.
Our study was undertaken to assess the potential clinical utility of in-vivo 31P MRS in the diagnosis of various untreated primary malignant and benign human breast lesions compared to normal tissue. For all lesions, study conditions were the same, including the use of a large volume of solid tissue in order to avoid contamination from adjacent tissue.
MATERIALS AND METHODS
Patient selection
Seventeen patients with malignant lesions [Group I; mean age of patients, 41.1 (range, 24-62) years], eight with benign lesions [Group II; mean age, 32.1 (range, 19-44) years] and, as controls, seven normal breasts [Group III; mean age, 43.7 (range, 40-47) years] were included. Patients with a palpable mass who had not previously undergone treatment or surgery were selected, and 18, fine needle aspiration biopsy (FNAB) was followed by 31P MRS between one day and eight months later. All malignant lesions were primary breast malignancies and in 12 patients (66.7%), the results of FNAB and surgical histology were consistent. Because of the characteristic of the coil, the volume of the tumor had to exceed 12 cc (3×2×2 cm), with a superoinferior diameter at least 3 cm, and either for this reason or because of the long interval between FNAB and 31P MRS, the effect of FNAB on 31P MRS was neglected.
Malignant tumors in which possible internal hemorrhage or necrosis had been revealed by previous clinical or radiological examination were excluded. Modified radical mastectomy was performed in 14 patients, one underwent lumpectomy, and because of metastasis, two were treated with chemotherapy only. Final pathologic diagnoses were invasive ductal carcinoma (n=14), medullary carcinoma (n=1), mucinous carcinoma (n=1), and metaplastic carcinoma, matrix-producing type (n=1).
Seven patients with benign lesions underwent excisional biopsy, and because a huge benign phyllodes tumor was present, the other underwent modified radical mastectomy. Final pathologic diagnoses were fibroadenoma (n=4), benign phyllodes tumor (n=2), lactating adenoma (n=1), and fibrocystic change (n=1). Five healthy women without any history of previous breast disease were selected as controls and the contralateral normal breasts of two patients with invasive ductal carcinoma were also included in this group. To confirm the normalcy of the breast as well as the appropriateness of the amount of breast tissue, mammography was performed prior to MRS. The menstrual cycle was in the luteal phase in two patients and in the menstrual phase in one; three had ceased to menstruate because of previous hysterectomy, chemotherapy or recent hormone replacement therapy, and one did not recall the date of her last menstruation. Verbal consent was obtained from all patients prior to examination.
One patient underwent 31P MRS prior to chemotherapy and three more times during chemotherapy.
All studies were performed consecutively between January 1999 and March 2000, and the project was approved by our institutional review board.
Methods
MRS was performed not more than a week prior to surgery, chemotherapy or any other treatment. For all examinations, a 1.5T whole-body MRI/MRS system (1.5 T Magnetom Vision ; Siemens, Erlangen, Germany) with a 1H-31P dual surface coil (27 cm-14 cm loops with 1H excitation and signal detection and 31P signal detection with a 31P preamplifier) was used. Patients were positioned either supine or prone on the table, with the 1H-31P dual surface coil covering the area of the tumor. The findings of previous mammographic and/or ultrasonographic studies were reviewed prior to and while MRS was being performed, and T1-weighted localizer MR images were obtained (TR 300 ms, TE 12 ms, 5 mm slice thickness, 420 mm field of view, 154×256 acquisition matrix, 2 NEX of acquisition). Localization was readjusted several times until the center of the coil correlated well with the center of the tumor. In each case approximately 15 minutes were needed to obtain the 31P MR spectrum, and spectral parameters were as follows : TR 330 ms, TE 3 ms, flip angle 90°, slab thickness 50 mm, FOV 420 mm, 16×1024 acquisition matrix, 11 NEX of acquisition.
Raw data (the integral of each metabolite) were obtained after the completion of scan averages for each examination and transferred to an installed program (Numaris spectroscopy analysis package VB33A). Apodization, zero- and first-order phase corrections were performed and all 31P MR spectra were plotted and analyzed in the absorption mode and then fitted to Lorentzian lineshapes. 31P MR resonances in the spectra were assigned on the basis of prior assignments such as phosphocreatine (PCr), inorganic phosphate (Pi), phosphomonoester (PME), phosphodiester (PDE), and α-, β- and γ-phosphorus adenosine triphosphate (ATP). Chemical shifts in 31P MR spectra were referenced to the position of PCr (δ=0.0 ppm) (PME, 7.1 ppm ; Pi, 5.3 ppm ; PDE, 3.6 ppm, γ-phosphorus of ATP, -2.4 ppm ; α-phosphorus of ATP, -7.7 ppm ; and β-phosphorus of ATP, -16.1 ppm) (13).
For normal controls, the coil was located in the area of the largest amount of normal tissue, which was most often 2 cm above and away from the nipple. The right breast was preferred because of the artifact from the heartbeat which occurs with the left breast.
Analysis of raw data
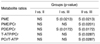
Mean and standard deviations of the integral of each metabolite were measured (Table 1). Various metabolite ratios were obtained, namely PME/PCr, Pi/PCr, PDE/PCr, γ-ATP/PCr, α-ATP/PCr, β-ATP/PCr, T-ATP/PCr, PME/β-ATP, Pi/β-ATP, PDE/β-ATP, PCr/β-ATP, γ-ATP/β-ATP, α-ATP/β-ATP, T-ATP/β-ATP, PME/T-ATP, Pi/T-ATP, PDE/T-ATP, PCr/T-ATP, γ-ATP/T-ATP, α-ATP/T-ATP, β-ATP/T-ATP, and PDE/PME. Data for the three groups were analyzed and compared using the Kruskal-Wallis test with Dunn's method; a p level of less than 0.05 was considered significant.
RESULTS
Seven parameters were statistically significant (Table 2). PME was significantly higher in both malignant and benign lesions than in normal tissue. PDE/PCr was also significantly different in both malignant and benign lesions compared to normal tissue, a finding which resulted from the relatively high PDE and low PCr in malignant and benign lesions and the relatively high PCr and low PDE in normal tissue. PME/PCr, T-ATP/PCr and PCr/T-ATP showed significant differences between benign lesions and normal tissue because of relatively high PME and T-ATP and low PCr in benign lesions and relatively low PME and T-ATP and high PCr in normal tissue. Differences between malignant lesions and normal tissue were borderline, and those between malignant and benign lesions were not significant. One patient who underwent four consecutive 31P MRS scans before and after chemotherapy showed elevated PCr and decreased PDE and PME when her clinical response to this therapy was good, and elevated PDE and decreased PCr when her response was poor (Table 3). This patient had lung metastasis, and clinical response was assessed according to her general condition, as indicated by blood markers and laboratory tests, and by the softness of the tumor on palpation. Magnetic resonance imaging (MRI) during chemotherapy revealed little apparent change in the size of her tumor or the extent of intratumoral microcalification (Fig. 1, 2, 3, 4).
DISCUSSION
Phosphorus metabolites play an important role in the human body as high energy metabolites. Phosphorus is fundamental for obtaining information about cell energy metabolism, the state of tissue oxygenation, pH, and membrane turnover (1). Phosphorus metabolites are abundant in viable tissue, and their clear, wide chemical shift spectrum observed in MRS; recommends them for use in medicine. The concentration of phosphorus metabolites is only one-tenth that of proton, however, and their signal is 100,000 times weaker than that of hydrogen (1, 3), and thus the clinical usefulness of 31P MRS is limited. It is, nonetheless, more suitable than other alternatives in settings involving the breast: this is a superficial organ, water suppression is not essential, and there is a greater lack of phosphorus metabolites in normal breast tissue than in other normal tissue (3, 5).
Among the seven peaks of phosphorus metabolites in 31P MRS, a high energy phosphate such as PCr or ATP provides energy for cytologic metabolites, and Pi represents the lowest energy state which increases in concentration as tissue becomes ischemic (1). PME indicates the presence of precursors of cytoplasmic membrane biosynthesis, such as phosphoethanolamine (PE) and phosphocholine (PC). PDE indicates the presence of breakdown products of membrane metabolism, such as glycerophosphoethanolamine and glycerophosphocholine (GPC).
Most tumors in organs such as the liver, brain and muscle show decreased PCr and increased PME and PDE, with greater change in PME (2). An elevated PME level reflects the higher membrane phospholipid metabolism associated with higher tumor cell reproduction and growth rates (2), though its level does not actually appear to correlate with the degree of malignancy. A good treatment response is indicated by decreased PME and PDE levels and increased PCr (15-17), while a poor response results in increased PME (17). These changes do not correlate with volume change, i.e. they are changes detectable by MRS before any detectable change in tumor volume. In our study, a patient who underwent four consecutive 31P MRS scans before and after chemotherapy showed elevated PCr and decreased PDE and PME at the time her clinical response was good. Because the MRI findings showed little changeduring the same period, these findings were important.
The current literature regarding 31P MRS of the breast describes variations in normal breast tissue according to the menstrual cycle, lactation, and the presence of various carcinomas, as determined by in-vivo, ex-vivo and in-vitro methods. Merchant et al. (13) reported that PME+Pi were lower and PDE+phosphorylated glycan (PG) were higher in breast cancers than in normal tissue and that PCr was high in benign disease, and Merchant (3) noted similar findings, namely that PME and Pi were lower and PDE and phosphorylated glycan were higher in breast cancers than in normal tissue. Redmond et al. (18) reported that α-ATP and γ-ATP were high and PCr was low in carcinomatous tissue, but that PCr was high in normal tissue. PDE/PCr was high in carcinomatous tissue, but this was without statistical significance.
Smith et al. (19) demonstrated low glycerophosphorylethanolamine levels, and low NTP and high Pi, in 46 human breast ductal carcinoma extracts. Degani et al. (20) documented the presence of increased NTP/Pi after tamoxifen treatment, as revealed by 31P MRS scanning of breast cancer tissue using the human MCF7 breast cancer cell line in athymic mice. This increase was explained as resulting from the rapid growth of fibrous reparative tissue following rapid necrosis. Singer et al. (21) obtained 31P MRS scans of breast cancer cell lines such as primary breast carcinoma (21PT, 21NT), metastatic breast carcinoma (21MT-2), and normal epithelium of the breast (76N); their results showed a 16-27-fold increase in phosphocholine (PC) in primary and metastatic carcinomas and decreased ATP and PCr, suggesting that the mechanism involved in the marked increase in PC was actually increased PC synthesis, or its decreased use in carcinomatous tissue. Using tissue extracts, Merchant et al. (22) showed that 31P MRS could differentiate benign from malignant lesions on the basis of elevated PME, and by the use of biopsy samples, Degani et al. (24) demonstrated that carcinomas contain three times more ATP and PME than benign breast lesions. Sijen et al. (15) performed in-vivo 31P MRS scanning in five human breast carcinoma patients and four normal volunteers, finding that in carcinomatous tissue there was high PME, Pi and PDE, but little PCr. PME decreased and PCr increased following radiotherapy, while in normal volunteers, PCr was high and all other phosphate metabolites were low. Kalra et al. (14) performed in-vivo 31P MRS scanning in 31 cases of human breast carcinoma, finding that PME and PDE were high but that PCr was not detected. In 14 normal volunteers, all phosphate metabolite levels were very low, and in three elderly patients undergoing tamoxifen therapy, PME/γ-ATP decreased with clinical improvement and increased when there was no improvement. Twelves et al. (16) performed in-vivo 31P MRS in 23 human breast carcinomas, finding high levels of PME, PDE and PCr, and low ATP. The results also revealed increased PCr and decreased PME levels after chemotherapy. Merchant et al. (25) demonstrated significant differences in PCr/Pi levels in both malignant and benign lesions, explaining that if parallel to ATP/Pi, this difference indicated necrosis of tumor tissue before volume changes occurred. Our study included only solid lesions without necrosis and no parameters were able to significantly differentiate malignant from benign lesions.
Among 46 normal volunteers, Redmond et al. (18) found higher PME and ATP levels and lower PCr in premenopausal than in postmenopausal women, while in their five normal volunteers, Sijen et al. (15) found elevated PCr and low levels of all phosphate metabolites (PME, Pi, PDE, and ATP). Twelves et al. (23) reported the results of in-vivo 31P MRS studies in eight lactating women and 14 non-lactating premenopausal women. The high levels of PME found among the former probably reflected the higher proportion of epithelial tissue present during lactation. PCr was low in these same women, and lowest during the follicular phase in normal premenopausal women.
The use of many metabolite ratios was inevitable because the quantitation of 31P suffers limitations arising from many factors. These include the difficulty of appropriate calibration, the sensitivity of surface coils, and technical variations in the geometry of many of the localization techniques and the minimization of noise differences (1, 18). Also, because the intensity of PME and PDE is low, analysis of their levels is difficult (2). Sijens et al. (15) used the PCr/ATP ratio, but other researchers used different ratios such as PM/ATP (2), PME/γ-ATP and PDE/γ-ATP (14), PME+Pi and PDE+PG (17), PDE/PCr, ATP/PCr and Pi/PDE (18), the percentage of the total 31P peak area of the spectrum, PDE/PME and PCr/Pi (16, 23), and PME/Pi, ATP/Pi, PCr/Pi, PME/ATP, PCr/ATP, PCr+Pi/ATP, glycerol phosphodiesters(GPD)/ATP and PDE/ATP (24). No concensus as to the most useful of these has emerged.
The diversity of the results reported in the literature seems to have numerous causes. Tumors before and after treatment, for example, and those with a large amount of necrosis were included in the same group, yet comparisons with benign lesions or normal volunteers were not made (5, 15, 19). In other cases, normal parenchymal tissue or pectoralis muscle was included in the area of examination (13-16, 18), or the diverse spectrum of benign diseases from cyst to fibroadenoma was included in the same group (24). In our study, in order to avoid contamination and include tumor tissue only, at least 12 cc of solid tumor without necrosis or hemorrhage was selected. As well as normal thissue, malignant and malign lesions were also included.
According to the literature, metabolite ratios for benign lesions differ from those for malignant tissue and are not distinguishable from those for normal breast tissue (1, 3, 15, 18, 22, 24, 25). In our study, PME, PDE and PCr levels in cancers and normal tissue were similar to those previously reported. Although the menstrual phases of normal control subjects varied, the patterns were all similar; among phosphorus metabolites, PCr showed the highest levels, and PME and PDE the lowest. In this study, however, benign and malignant lesions could not be differentiated. Because we included only large lesions, those with a volume of at least 12 cc, an explanation for this result could be that for large lesions, whether pathologically benign or malignant, tumor metabolism is similar. The literature explains that lactating breasts show a similar spectral pattern to that of malignant lesions (16, 23), the suggested mechanisms for this being either that 1) PME simply reflects the increased proportion of epithelial tissue, whether normal or malignant, or 2) that elevated PME may be due to increased membrane synthesis in hyperplastic or proliferating breast tissue (16). That all patients involved in this study were relatively young is probably related to the fact that among Korean women, the age at which breast cancer is most prevalent is about ten years less than among western women. The reason for this is not clear.
In conclusion, localized in-vivo 31P MRS in the present study showed that using current techniques, a broad clinical spectrum can be demonstrated. In addition, and contrary to the conclusions reached by earlier reports, 31P MRS does not in fact differentiate malignant from benign breast lesions, at least where the volume of a lesion is relatively large. Although not statistically proven in this study, the primary role of 31P MRS in breast disease may, therefore, be to monitor the response of sizable tumors during therapeutic trials rather than the differential diagnosis of benign from malignant lesions or the initial diagnosis of small, early breast cancer.






 XML Download
XML Download