

 PDF
PDF ePub
ePub Citation
Citation Print
Print


In clinical practice, acute viral encephalitis is usually diagnosed on the basis of clinical features and laboratory examinations, especially CSF (cerebrospinal fluid) findings. A specific viral etiology can usually be confirmed by a combination of serologic tests of acute and convalescent phase sera and by the inoculation of blood or CSF into susceptible animals or tissue. In fatal cases, the virus can often be isolated from the brain by the inoculation of susceptible animal and tissue culture (1). Brain imaging studies may help the diagnosis of some cases of acute viral encephalitis; herpes simplex encephalitis (HSE), for example, characteristically involves the insula, temporal lobe and limbic system (2). Japanese encephalitis (JE), endemic in some regions of Asia, also characteristically involves, in most patients, a particular site, namely the thalamus (3-8). It is not uncommon, however, to encounter patients who present with clinical and CSF features consistent with acute viral encephalitis but neither specific serologic nor characteristic imaging findings suggestive of a specific viral etiology.
We recently encountered six cases of acute encephalitis of unknown etiology. The brain CT or MR imaging findings of these patients were similar, but serologic studies were negative for JE and/or HSE. To our knowledge, no study has described the imaging findings of this unusual type of acute encephalitis. In an attempt to make radiologists more aware of the diverse imaging findings of acute encephalitis, we present the brain CT and MR imaging findings of these six patients.
MATERIALS AND METHODS
Between 1997 and 1999, we retrospectively reviewed the medical records and CT and/or MR imaging findings of six patients [four men and two women aged 25 to 42 (mean, 37) years] with acute encephalitis involving the thalamus. The condition was diagnosed on the basis of clinical features and CSF examinations. The clinical features included fever, headache, disorientation, and confusion or mental alteration. In all patients, CSF examinations revealed lymphocyte-dominant pleocytosis in the range of 32 to 442 cells per microliter, elevated protein, and normal glucose. The clinical and laboratory findings are summarized in Table 1. No patient had been recently immunized or immunocompromised. In all patients, initial serologic tests for JE and HSE viruses were performed during the acute and convalescent stages (7-40 days after the onset of illness). In three, the serologic test for JE virus was performed twice, at an interval of 7 to 30 days, and in two, the serologic test for HSE virus was also performed twice, at an interval of 5 to 7 days. Serologic diagnosis of JE was based on the criteria developed by the research group for JE in Japan (i.e. a fourfold or greater rise in positive results in the haemagglutination inhibition test for the JE virus in paired sera) (9). For serological diagnosis of HSE, polymerase chain reaction (PCR) was used for the detection of herpes simplex virus DNA in CSF (10). In addition, serologic tests for a variety of pathogens were performed: cytomegalovirus in four patients, Epstein-Barr virus in four, mycoplasma in one, enterovirus in one, rubella in one, and human immunodeficiency virus in one. In all patients, serum and CSF were also examined for ordinary bacteria, fungus and acid-fast bacili (AFB) by direct staining and culture. All the serologic examinations mentioned above were negative in all patients. Despite the fact that all patients were treated with acyclovir, clinical outcomes were very poor: death (n=3) or a vegetative state (n=3).
Brain imaging studies were performed during the acute and/or convalescent stage of the illness. CT (n=6) and MR imaging (n=6) were performed 3 to 18 days and 5 to 40 days, respectively, after the onset of the condition. Four patients underwent follow-up MR imaging 11 to 45 days after onset, and one of these underwent further follow-up imaging 48 days after onset. For MR imaging, a 1.5 T imager (Magnetom; Siemens, Erlangen, Germany) was used in four cases, and a 1.0 T imager (from the same source) in two. All patients underwent spin-echo T1-weighted (repetition time [msec]/echo time [msec]: 500-800/20-25), fast spin-echo T2-weighted (2,200-2,500/60-90), and fluid-attenuated inversion recovery MRI sequences. Contrast-enhanced (IV injection of 0.1 mmol/kg of gadopentetate dimeglumine) T1-weighted spin-echo images were obtained in all patients except one (case 2).
Two radiologists evaluated the imaging features, focusing on the involved area, attenuation at CT and signal intensity at MR imaging of the lesion, and whether or not enhancement was observed.
RESULTS
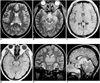
The brain CT and MR imaging findings are summarized in Table 2. Brain CT performed 3-18 days after the onset of illness revealed diffuse brain swelling (n=2), low attenuation in both thalami (n=1), or no abnormal findings (n=3). In all patients, initial MR images of the brain obtained 5-40 days after onset revealed multiple patchy areas of focal abnormality. The thalamus was involved either bilaterally (n=5) or unilaterally (n=1), thalamic lesions being homogeneously hypointense on T1-weighted and hyperintense on T2-weighted images. In no patient did the signal intensities observed on initial and follow-up MR images suggest hemorrhage. Lesions were also seen in the midbrain (n=5), the medial area of the temporal lobe (n=4; 3 bilateral and 1 unilateral), the pons (n=3), both hippocampi (n=3), the insular cortex (n=2; 1 bilateral and 1 unilateral), the medulla (n=2), the lateral temporal lobe cortex (n=1), both cingulate gyri (n=1), both basal ganglia (n=1), and the cortex of the left hemisphere (n=1). Follow-up MR images obtained in four patients showed that in two (cases 1 and 5) (Figs. 1, 2), the extent of the lesion had increased markedly. In one of these two (case 5) the lesion subsequently became smaller, and this was associated with diffuse brain atrophy and periventricular white matter change, suggesting microcystic cerebromalacia or gliosis. In the remaining two patients (cases 2 and 4), follow-up MR imaging of the lesion revealed no apparent change. Contrast-enhanced T1-weighted MR images showed no parenchymal enhancement, though diffuse corticosulcal vascular or leptomeningeal enhancement was seen in two patients (cases 3 and 5).
DISCUSSION
A wide range of pathogenic organisms, the most common of which are viruses which include herpes simplex types 1 and 2, herpes zoster, arboviruses and enteroviruses, cause acute encephalitis (1, 11). In general, acute viral encephalitis causes diffuse parenchymal infiltration of inflammatory cells, and this leads to chromatolysis and pyknosis of neurons and at times extensive necrosis (1, 11). These pathologic findings are reflected by areas of low attenuation on CT, low signal intensity on T1-weighted MR images, and high signal intensity on T2-weighted MR images, depending on the degree and severity of inflammation.
In our cases, although no specific viral etiology was proved in any patient, the CT and MR imaging findings appear to be similar to those of JE in terms of the frequency of involvement of the thalamus and brain stem, and -inparticular-, of the substantia nigra and pons. In JE, pathologic changes occur mainly in the gray matter and predominantly affect the diencephalon, mesencephalon, brain stem and cerebellar Purkinje cells, involving both thalami and the substantia nigra the most severely (3, 12-13). It has been reported that the CT and MR imaging findings of JE are consistent with the distribution of pathologic change. Previous articles describing these findings stated that the thalamus was usually symmetrically involved and other areas including the basal ganglia, midbrain, pons, cerebellum, cerebral cortex and spinal cord also showed frequent involvement (3-8). Hemorrhagic changes were very often seen in the primary lesion of JE, especially in the thalamus. Kumar et al. (5) reported that in all JE patients, follow-up images obtained 10-60 days after the onset of illness showed hemorrhagic lesions in the thalamus. Kimura et al. (8) reported that HMPAO uptake in the bilateral thalami and putamina, as seen on single-photon emission CT (SPECT), increased markedly in all the four patients in whom JE was confirmed, a finding which might be useful in differentiating JE from HSE and other types of encephalitis. In our cases, the hippocampus and medial area of the temporal lobe were also frequently involved, though these sites were very rarely involved in JE (3-8). Therefore, in our cases, imaging findings of no hemorrhagic foci, a low rate of involvement of the basal ganglia and cerebellum, frequent involvement of the hippocampus and medial area of the temporal lobe, and the negative result of serologic tests militate against a diagnosis of JE.
In our cases, lesions were also seen in the medial area of the temporal lobe, hippocampus and insular cortex, regions which are more frequently involved in HSE than in JE. HSE is known to lead to abnormal lesions in characteristic locations of the brain; the medial temporal lobe, subfrontal area, insular cortex and cingulate gyrus are preferentially involved, and rhombencephalitis involving the midbrain has sometimes been reported (2, 14-15). In these preferred areas, HSE lesions are seen as focal areas of low attenuation on CT, and as areas of low and high signal intensity, respectively, on T1-weighted and T2-weighted MR images. In addition, a parenchymal or gyral pattern of enhancement and foci of subacute hemorrhage may be observed slightly later. These imaging findings can help make a diagnosis of HSE fairly certain and prompt, though involvement of the thalamus, as in our cases, is very unusual in HSE.
In our cases, dual infection with the JE and the HSE virus was a possibility. In analogous experiments in mice, JE viral antigen was localized in herpes virus-infected areas of the brain, suggesting that the JE virus gains access to the central nervous system (CNS) at sites of blood-brain barrier disruption caused by the HSE virus (12, 16), and imaging findings suggested a combination of JE and HSE. However, repetitive serologic tests failed to identify either the JE or HSE virus. Unilateral thalamic involvement was also reported in a CNS lesion associated with Epstein-Barr virus infection (17), though the good prognosis and fleeting imaging abnormality seen in this infection are different from the observed findings in our cases.
The possible involvement, in our cases, of a new or different viral agent, for which serologic tests were not performed, could not be excluded. In our series, repeated serologic testing for JE involved the hemagglutination inhibition test, which in an appraisal of a recent diagnostic assay for JE showed a sensitivity of about sixty percent (18). The use of polymerase chain reaction for detecting HSE virus DNA in CSF has been reported as the most sensitive noninvasive method for early diagnosis of HSE (19), but in our cases the technique failed to demonstrate that either the JE or HSE virus was an etiologic agent. The mortality rate for JE has been reported as 20-50% (20), and in cases of herpes encephalitis, acyclovir effectively reduces mortality and morbidity if administered early (19). Compared with the prognosis of JE and HSE reported previously, that of our patients was very poor despite the fact that in all cases, acyclovir was injected intravenously since the onset of the condition.
Yagishita et al. (21) reported acute encephalopathy with bilateral thalamotegmental involvement in infants and children, which can be a postviral or postinfectious brain disorder. There was, however, no clinical or laboratory evidence of encephalitis (no pleocytosis in the CSF). Although the involved sites in our patients were similar to those in Yagishita's, the CSF findings and age range are completely different.
The acute disseminated and immune-mediated forms of encephalomyelitis may have clinical and CSF features similar to those of our cases. The pathological findings of the first of these are, however, diffuse bilateral perivenular inflammation and demyelination, mainly involving the cerebral white matter, and for this reason - unlike in our cases, in which the gray matter was involved - MR imaging usually demonstrates bilateral abnormalities in the cerebral white matter (22). Bilateral increased signal intensity on T2-weighted images of the basal ganglia and thalamus has been reported in patients with sporadic and variant Creutzfeldt-Jakob disease (CJD) (23, 24). CJD, however, shows no leukocyte response in CSF and has clinical features different from those of our patients (25).
In conclusion, the CT and MR imaging findings of acute encephalitis involving the thalamus were similar to a combination of those of JE and HSE. Further investigation, aimed at documenting the specific causative agent showing these imaging features, as well as histopathologic study, is needed.



 XML Download
XML Download