

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Gastrointestinal stromal tumors (GISTs) are the most common type of mesenchymal tumor in the gastrointestinal tract arising from the interstitial cells of Cajal (1). Distant metastasis occurs at rates between 23% and 47%, with 20% to 60% of these cases affecting the liver (23). For treatment of metastatic GISTs, the introduction of imatinib mesylate has resulted in notable improvements in the clinical outcomes for patients (45). Although up to 80% of patients exhibit an initial response to imatinib treatment, secondary resistance eventually develops in most patients (67). Therefore, a combination of surgery and imatinib treatment is now widely used in clinical practice for GIST cases, and the treatment protocol is referenced in current practical guidelines on GIST management (89).
Radiofrequency ablation (RFA) has recently been evaluated as an alternative form of treatment in several cases of unresectable GIST with liver metastasis (310111213). RFA may be a useful therapeutic option for patients with metastatic GIST and should be performed at the time of best clinical response, followed by post-procedural imatinib maintenance therapy (14). Among RFA techniques, intraoperative RFA (IORFA), with or without surgical resection, has been reported to yield several advantages when compared with percutaneous RFA, including a broader indication for surgical resection as a treatment for various hepatic metastases (10). By combining IORFA with resection, more patients may become candidates for surgical treatment because the surgeon would be able to resect larger tumors while ablating residual smaller tumors (1516). A combination therapy comprising surgical resection and IORFA has yielded potential benefits in certain cases; however, consequent long-term survival rates or broadening of surgical indications have rarely been reported (17).
In this study, we aimed to evaluate the feasibility and safety of IORFA for the complete removal of unresectable hepatic metastases secondary to GIST, with or without combined hepatic resection during continued imatinib therapy.
Go to : 
MATERIALS AND METHODS
The local Institutional Review Board provided study approval and waived the requirement for informed consent because of the retrospective design. Between August 2009 and February 2017, 24 patients with hepatic metastases of GIST that were histologically proven were included in the current study. Firstly, the feasibility and benefit of surgical resection in patients with hepatic metastasis from GIST were considered after a discussion by oncologists and surgeons. Patients with surgically unresectable hepatic metastases (e.g., a daughter tumor in another lobe that would cause hepatic insufficiency if resected) were considered for IORFA.
The inclusion criteria were as follows: 1) complete resectable hepatic tumors by surgical resection with additional IORFA or by IORFA alone after discussion on multidisciplinary team; 2) an unacceptably high risk of hepatic insufficiency after resection alone; 3) tumors in locations unfavorable for surgical resection, such as in the center of liver; and 4) tumors in locations unfavorable for percutaneous RFA, such as in the subcapsular location. The exclusion criteria were as follows: 1) large size (> 3 cm) and number (> 5) of target tumors for IORFA; and 2) target tumors for IORFA were abutting a major structure (e.g., portal vein, hepatic artery, or bile duct). The number, size, and location of liver metastases were assessed to evaluate the feasibility of surgical resection and IORFA, using ultrasound (US), computed tomography (CT), and magnetic resonance image (MRI) one month before surgery.
Background Data of Included Patients
Table 1 lists patients' sex, age, primary tumor characteristics, pre-surgical imatinib administration status, primary and metastatic resection data, and IORFA status. IORFA and/or surgical resection were curatively performed for complete removal of hepatic metastasis. In total, 76 hepatic metastases were treated, of which 47 had been surgically resected (2.4 ± 1.3 per patient; mean size, 2.8 ± 1.6 cm) and 29 had undergone IORFA (1.2 ± 0.5 per patient; mean size, 1.6 ± 0.6 cm). The mean age of the patients was 53.9 ± 12.5 years. The locations of the primary GISTs were the stomach in 10 patients (41.7%), the small intestine in 13 (54.2%), and the large intestine in one (4.2%), and their mean size was 7.1 ± 3.0 cm. Of the 24 patients, 19 (79.2%) received imatinib therapy prior to surgery, whereas five (20.8%) underwent surgical resection before imatinib therapy. All included patients received imatinib therapy as standard treatment after IORFA or surgical resection.
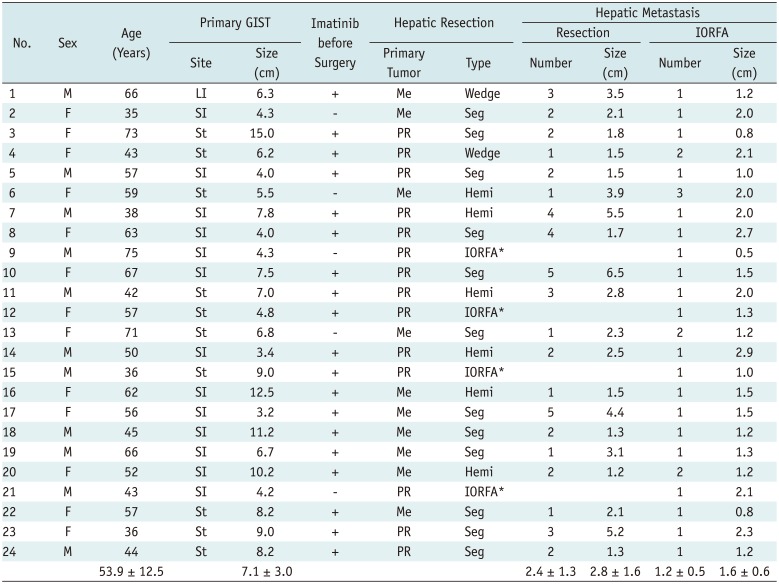
Table 1
Patient Characteristics and Treatment Detail
![]()
Surgical Resection
At the time of laparotomy, intraoperative hepatic ultrasonography (AVIUS; HITACHI ALOKA Ltd, Tokyo, Japan) was performed to identify, count, and characterize the nature and vascular proximity of the metastatic tumors. The locations of the metastases and their relationships with surrounding vascular and biliary structures dictated whether to perform a formal anatomic resection. In general, the extent of surgery was determined based on the estimated hepatic functional reserve, which was assessed using a combination of preoperative liver biochemistry, distribution of metastatic tumors within the liver, and predicted remnant liver volume after resection. Resection was classified as less than a hemihepatectomy (e.g., wedge or segmentectomy), hemihepatectomy, or extended hepatectomy (≤ 5 liver segments) (18).
Following removal of their primary GISTs, 14 patients (58.3%) also underwent hepatic resection during the same procedure. The remaining 10 patients (41.7%) underwent hepatic resection for residual or recurrent hepatic metastases at a mean interval of 27.6 ± 25.6 months following removal of their primary GISTs. Of the total 24 patients, 20 (83.3%) underwent IORFA following hepatic resection and four (16.7%) underwent IORFA alone. In addition, two of the 20 who had IORFA underwent wedge resection (10.0%), 12 underwent segmentectomy (60.0%), and six underwent hemihepatectomy (30.0%) (Table 1).
IORFA
Intraoperative radiofrequency ablation was performed by an interventional radiologist who had 18 years of experience in performing oncological interventions, including RFA under real-time US guidance with a 7-MHz convex probe (AVIUS; HITACHI ALOKA Ltd). Before the surgical resection of possible metastatic liver tumors, an intraoperative US evaluation was performed to identify the liver metastatic tumors; these findings were compared with preoperative CT or MRI findings. After the surgical resection was done for the surgically resectable tumors, a single 17-gauge internally cooled electrode (Proteus; STARmed Co., Goyang, Korea) was inserted in the center of the tumors under real-time US guidance (Fig. 1). If the tumor was ovoid in shape, insertion of the electrode along the longer side was attempted. The electrode was then connected to a 480-kHz electric current generator (VIVA RF system; STARmed Co.) that delivered a maximum output of 200 W. Correct positioning was confirmed by US before applying radiofrequency energy for 12 minutes in the automatic impedance mode. Post-ablation intraoperative US images were evaluated immediately after the procedure. The endpoint of IORFA was confirming the tumors inside the echogenic ablated zone with more than 5 mm-circumferential margins.
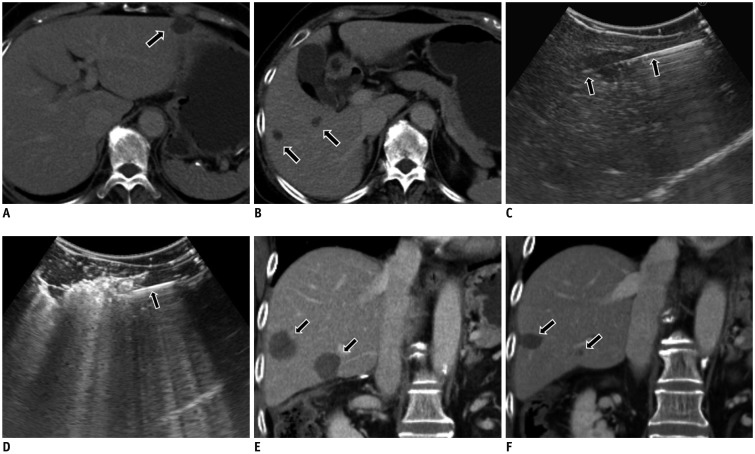 | Fig. 171-year-old female patient (No. 13) presented with three liver metastases.
A. Metastatic tumor in left lateral segment (arrow on axial CT) was surgically resected. B. Two tumors (arrows) in right lobe were ablated because of suspected hepatic failure after extensive hepatectomy. C. Radiofrequency electrode (arrows) was placed in hepatic tumor under intraoperative ultrasound guidance. D. Echogenic bubble was noted at tip of electrode (arrow) during ablation. E. Coronal CT image obtained seven days after IORFA shows two ablated zones (arrows) with complete coverage. F. Coronal CT image obtained 13 months after IORFA shows no evidence of local tumor progression. Ablation zones (arrows) indicate considerable decrease in size. CT = computed tomography, IORFA = intraoperative radiofrequency ablation
|
Follow-Up, Definitions and Evaluation of Data
Contrast-enhanced CT, MRI, and/or positron emission tomography were used to evaluate the target tumor or recurrence at one, three, six, and 12 months, and annually thereafter.
The reporting standards of the Society of Interventional Radiology were used to define success, outcomes, and complications (19). Technical success was achieved when a treated tumor was ablated with sufficient margin (more than 5 mm) at the time of the procedure. Technical effectiveness was defined as complete tumor ablation shown on imaging follow-up 1–3 months after IORFA. As the lesions commonly appear hypoattenuating before and after ablation, full coverage of the index tumor by the non-enhancing ablation zone was regarded as complete ablation (3). The overall and cancer specific patient survival period were defined as the interval, in months, between the initial IORFA and the patient's death from any cause or from cancer, respectively.
All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS) for Windows, version 13.0 (SPSS Inc., Chicago, IL, USA). Overall and GIST-specific survival rates were calculated using the Kaplan-Meier method.
Go to :
RESULTS
Therapeutic Response and Complications
The mean follow-up duration was 50.7 ± 34.7 months. Each tumor was subjected to a single IORFA procedure, 100% of which were technically successful and effective for the treated metastases. Two patients (8.3%) had major complications, namely biliary stricture and hepatic abscess. These complications were attributed to either the surgical resection or the IORFA procedure. Patient 17 underwent IORFA for a 1.5-cm-sized perihilar tumor and presented with symptomatic biliary stenosis at the 15-month follow-up, which was successfully treated with endoscopic drainage. Patient 19 had a hepatic abscess following surgical resection, which was successfully treated with percutaneous drainage and antibiotic administration. Two patients (8.3%) had persistent pain as a minor complication that improved with conservative treatment. Imatinib therapy was resumed postoperatively in all included patients (Table 2).
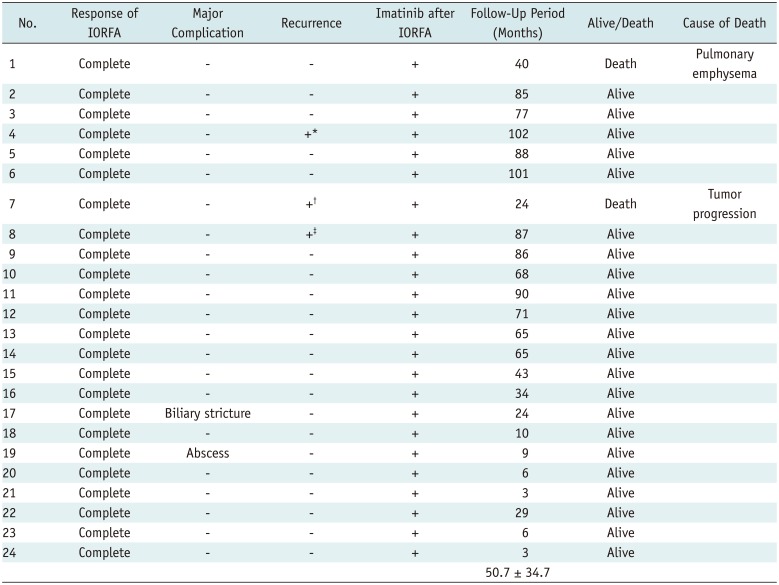
Table 2
Treatment Results and Clinical Outcomes after IORFA
![]()
Three patients (12.5%) developed recurrent tumors during the follow-up period. Patient 7 recurred with multiple distant tumors in the liver and peritoneum 16 months after a technically successful IORFA (Fig. 2). The primary tumor had been a 7.8 cm GIST in the small intestine, and their metastatic tumors were completely removed by lobar resection (n = 4) or IORFA (n = 1) at initial. The patient also received imatinib therapy before and after IORFA. Despite continued imatinib therapy plus cisplatin-based transarterial chemoembolization for the relapsed hepatic metastasis, the patient died 24 months after IORFA. Patient 8 had a marginal recurrent tumor around the ablated zone in the liver 51 months after an effective IORFA procedure. Patient 4, who had presented with a gastric GIST with hepatic metastasis, developed a gastric recurrence 95 months after IORFA. We concluded that patients 4 and 8 were resistant to imatinib and therefore changed their chemotherapy regimens. No other patient developed intrahepatic or extrahepatic recurrence or metastasis during the follow-up period.
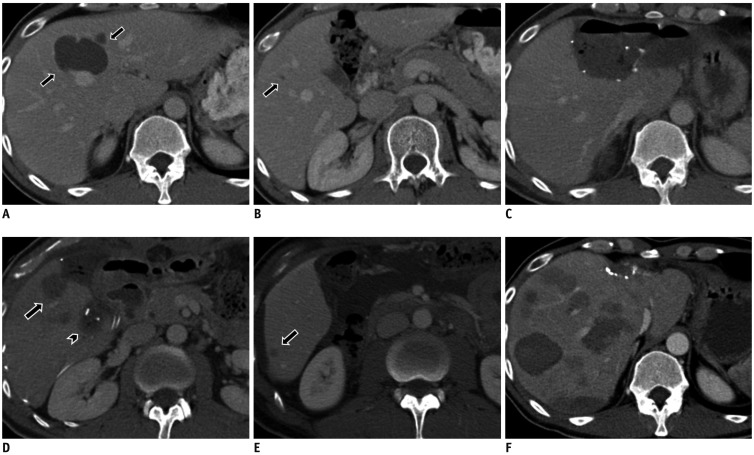 | Fig. 238-year-old male (Patient 7) presented with five liver metastases.
A. Metastatic tumors in segment 4 (arrows, axial CT) were surgically resected with sub-capsular metastatic tumors. B. Tumor (arrow) in right lobe could not be removed surgically because of risk of hepatic failure after extensive hepatectomy. C. Left lobectomy was performed to remove bulk of main metastases. D. IORFA (arrow) was performed for tumor located deep in right lobe. Partial hepatectomy (arrowhead) for sub-capsular tumor is visible. E. Axial CT image obtained five months after IORFA shows single recurrence (arrow) in right lobe. F. Axial CT image obtained 10 months after IORFA shows progression of multiple tumors and recurrence in remaining liver.
|
Survival
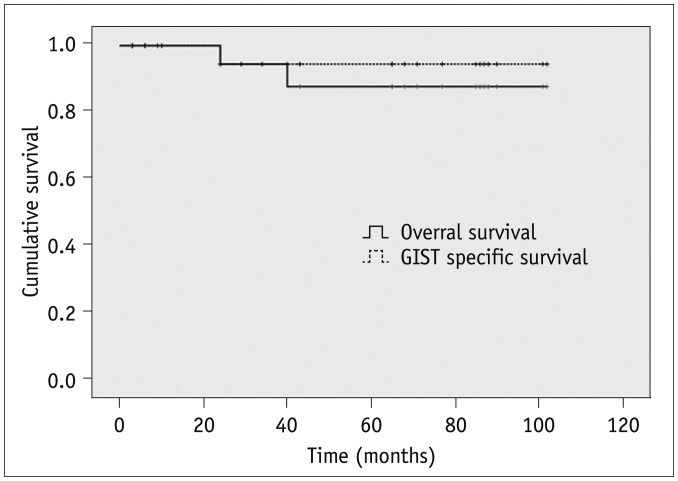
Two patients (1 and 7) died, and 13 remained alive without residual tumors at the time of the last imaging follow-up. Patient 7 (mentioned above) died from tumor progression 24 months after IORFA. Patient 1 died from aggravated pulmonary emphysema 40 months after IORFA, and had no evidence of GIST recurrence at any point during follow-up.
The cumulative overall survival rates were 100, 94.4, and 87.7% at one, three, and five years, respectively. The GIST-specific survival rates were 100, 94.4, and 94.4% at one, three, and five years, respectively (Fig. 3). The median survival time was not calculated because the survival curve did not decrease to 50%.
Go to :
DISCUSSION
Managing hepatic metastasis from GISTs remains a challenging clinical problem. Liver resection, which may be curative, is the preferred treatment when the indications for complete resection are met (2021). However, a large tumor burden or multiple tumor locations in the hepatic parenchyma may contraindicate resection because of the risk of leaving insufficient liver tissue that can result in postoperative liver failure (22). In the current study, in which we aimed to treat metastases that would otherwise be considered unresectable because of the risk of hepatic insufficiency, IORFA was applied either alone (n = 4) or with resection (n = 20). This combination approach allowed surgery in patients who had unresectable tumors, because the surgeon can resect larger tumors and ablate smaller ones. IORFA was used alone in the following situations: patients had tumors in unfavorable locations for surgical resection; when there was an unacceptably high risk of hepatic insufficiency after resection; or if the patient could not tolerate a major parenchymal resection.
The introduction of tyrosine kinase inhibitors (TKIs) revolutionized the treatment of metastatic GISTs; these agents target specific molecular abnormalities that are crucial to tumor physiology (2324). Although the exact role of surgical resection remains unclear, it is generally recommended either for responders within six months of initiating TKI therapy (to minimize the risk of acquiring secondary mutations responsible for TKI resistance) or for patients who demonstrate early signs of TKI resistance on CT (e.g., slowed or halted tumor shrinkage) (2526). Disease relapse during imatinib therapy has mainly been attributed to tumor resistance caused by the development of secondary mutations. An increase in the dose of imatinib mesylate, or changing to another targeting agent (e.g., sunitinib, nilotinib, or sorafenib), could improve the outcomes and stabilize the disease for some patients (27). However, TKI treatment appears to be critical for achieving long-term survival when there is recurrent or metastatic GIST. Given that the combination of TKI therapy and surgery seems to prolong survival, it is vital that measures are developed to prevent acquired resistance (2829).
If surgical resection is not feasible, the administration of multiple TKIs or TKI therapy in a neoadjuvant setting might improve the survival of a patient with unresectable liver metastases (2029). However, the authors of the current study attempted to administer IORFA with surgical hepatic resection to broaden the indications of surgical resection, and thus include patients with apparently unresectable liver metastases. Pawlik et al. (15) also administered IORFA for unresectable hepatic metastases of GIST either in combination with surgical resection or alone. These authors reported that patients who were treated with IORFA either alone (84.6%) or in combination with surgical resection (88.9%) had a significantly higher rate of recurrence, compared with patients who underwent resection alone (57.1%). Pawlik et al. (15) further reported a median overall survival duration of 47.2 months, with one-, three-, and five-year actual overall survival rates of 91.2, 65.4, and 27.1%, respectively.
In the current study, we achieved a therapeutic response of 100% and a tumor recurrence rate of 6.7%. The GIST-related survival rates were 100, 94.4, and 94.4% at one, three, and five years, respectively. Note, however, the median survival duration was not calculated because the survival curve did not decrease to 50%.
There are three main explanations for the low tumor recurrence and high survival rates in this study. First, the combination of RFA and imatinib may be responsible because 73.3% and 100% of our patients received imatinib before and after surgery, respectively. By contrast, in the study by Pawlik et al. (15), only 39.5% and 39.4% received imatinib before and after surgery, respectively. Second, the sizes of the metastatic tumors may be important. In the current study, the mean maximum sizes of the resected and ablated tumors were 3.0 ± 0.6 cm and 1.6 ± 0.7 cm, respectively, whereas Pawlik et al. (15) reported a median size of 3.9 cm for all included tumors. During planning for our study, metastatic tumors > 3 cm were not indicated for IORFA, which might explain the improved results. Third, US guidance during IORFA may have played a role, because an interventional radiologist performed IORFA under real-time US guidance. This method yields a more accurate and precise ablation zone compared with palpation alone, especially for cases involving deeply located metastatic tumors. Finally, complete removal by IORFA and/or surgical resection may have been important. In the current study, a surgeon, an oncologist, and an interventional radiologist reported that all included patients achieved non-detectable GIST on radiographic images after surgery.
In the current study, a multidisciplinary team initially planned IORFA prior to the surgical procedures for complete removal of the hepatic tumors. Generally, compared with percutaneous RFA, IORFA has some advantages and disadvantages. Advantages include good patient tolerance due to the use of general anesthesia and the ease and accuracy of targeting due to the intraoperative US guidance. Disadvantages include unavailability of US fusion imaging and change of orientation of the tumor location due to the surgical mobilization of tissue outside the tumor site.
The major limitations of this study are its retrospective design, small sample size, and the lack of a control group. A prospective randomized study with a larger sample should be performed to confirm our findings. Another important limitation is that the inclusion and exclusion criteria were vague. When the decision to resect hepatic metastases was made, it was hard to give an exact prediction of residual hepatic function after hepatic surgery. To overcome this limitation, the multidisciplinary team, including an oncologist, surgeon, and interventional radiologist, discussed the tumor resectability and potential for clinical benefit to patients before making their final decisions. Moreover, the inclusion and exclusion criteria for IORFA were otherwise clear in terms of the size, number, and location of hepatic tumors considered suitable for treatment.
In conclusion, the present study indicates that IORFA produces acceptable outcomes in appropriately selected patients with unresectable hepatic metastases from GISTs. Assuming a well-designed multidisciplinary intervention, IORFA with or without surgical resection might be helpful in providing effective local tumor control and longer disease-free survival in patients with unresectable hepatic metastases from GISTs or who exhibit partial response to imatinib.
Go to :
 XML Download
XML Download