

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Central vein stenosis is an important complication in hemodialysis patients. These patients present with swelling and pain in the ipsilateral upper extremity, chest, and face. Moreover, significant stenosis of the central vein is a cause of dialysis shunt dysfunction, dilated superficial collateral veins, and cellulitis (1). In addition, dialysis shunt thrombosis (23) or prolonged hemostasis is a further complication arising from shunt dysfunction (1).
Standard endovascular treatment of symptomatic central vein stenosis is angioplasty with conventional balloon. The reported primary patency rates of this technique at 6 months and 12 months are 45 ± 8% and 29 ± 8%, respectively (4). Stenting is indicated in case of elastic central vein stenosis or recurrent stenosis within a 3-month period according to the National Kidney Foundation Kidney Disease Outcomes Quality Initiative (NKF-KDOQI) guidelines (5). However, stent placement is not suitable in some cases because of the position of stenosis, particularly near the bifurcation of the central vein including the merging of the right and left brachiocephalic veins and the site of merging of the subclavian and internal jugular veins. Early intra-stent restenosis is also a similar problem for shunt dysfunction, venous hypertension, and ipsilateral arm edema.
Paclitaxel-coated balloon angioplasty (PCBA) provides a good outcome in terms of significant reduction of restenosis in arterial disease (6789). A recent randomized controlled clinical trial favored the use of PCBA to treat dialysis access stenosis (10). However, there is limited data on the use of PCBA for the treatment of stenosis of the central vein. The purpose of this study was to report the 12-month results of angioplasty with paclitaxel-coated balloons for the treatment of early significant restenosis of central veins in hemodialysis patients.
Go to : 
MATERIALS AND METHODS
Patients
This study was approved by the Ethics Committee of our institute. The study was a retrospective study of all hemodialysis patients who underwent treatment by angioplasty with paclitaxel-coated balloons plus a high pressure balloon in our hospital from January 2014 to June 2015. The data were retrieved from the Radiology Department records and hospital databases. Nineteen patients met the inclusion criteria which included patients who had significant restenosis of the native or intra-stent central vein within 3 months after the previous conventional balloon angioplasty. However, three patients were excluded because of loss to follow-up or missing data. Consequently, the study population included sixteen patients.
Procedure
The patients underwent antegrade puncture with an 18-G needle into the venous limb of an arteriovenous graft or arm vein of an arteriovenous fistula. An angiogram was performed to evaluate the dialysis shunt from the arterial anastomosis of an arteriovenous graft or arteriovenous anastomosis of an arteriovenous fistula to the central vein. In case of significant central vein stenosis, a 7-French vascular sheath was inserted via the graft or shunt vein of the ipsilateral arm over a 0.035-inch hydrophilic guidewire. Another 7-French vascular sheath was inserted into the right common femoral vein via antegrade puncture. A total dose of 3000 IU of heparin was injected via the vascular sheath. Then, angioplasty was performed using two IN.PACT™ Admiral™ paclitaxel-coated balloons (Medtronic, Minneapolis, MN, USA) via vascular sheaths from the arm and the right common femoral vein with a diameter of 6–7 mm at normal pressure (8 atmospheres) for 3 minutes. All patients were additionally dilated with larger balloons due to recoil with a relatively significant residual stenosis. The additional balloon catheter was an ATLAS® high pressure balloon (BARD, Tempe, AZ, USA) with a diameter of 12–14 mm at 6–10 atmospheres for 2 minutes (Fig. 1) via vascular sheaths from the arm until full expansion of the balloon. Then, a final angiogram was performed to evaluate the residual stenosis. In some cases, if the initial angiogram showed tight stenosis of the central vein, predilatation with a conventional balloon (diameter 6 mm) was performed.

Follow-Up
All patients successfully underwent regular hemodialysis procedures and all of them attended follow-up at the hemodialysis center and vascular surgery clinic. Measurements of the arm and regular angiographic follow-ups were also scheduled every 3 months.
Definitions
According to the standard practice guideline provided by the Society of Interventional Radiology (11), procedural success was defined as less than 30% residual luminal diameter stenosis and resumption of normal dialysis for at least one session. Primary patency was defined as uninterrupted patency after intervention until restenosis of more than 50% of the luminal diameter. Major complications were defined as complications that required additional treatment, permanent sequelae or death. Minor complications were defined as problems requiring no or nominal therapy and no sequelae.
Statistical Analysis
The study outcomes included procedural success (< 30% residual stenosis) and primary patency of the treated central vein lesions, which were presented by performing a Kaplan-Meier analysis. The median primary patency durations were also compared between the last previous conventional balloon angioplasty and PCBA. p values less than 0.05 were considered statistically significant.
Go to :
RESULTS
A total of 16 hemodialysis patients with 16 stenotic central veins were enrolled in this study. There were 9 males and 7 females. The mean age of the patients was 66 ± 14 years (range, 40–82 years). All patients presented with ipsilateral arm swelling with increased venous pressure during hemodialysis. There were 10 cases of native central vein stenoses and 6 cases of intra-stent central vein stenoses. The 16 sites of central vein stenosis were the brachiocephalic vein (15 cases) and the subclavian vein (1 case). All patients had a history of multiple conventional balloon angioplasties of the central vein. The median patency duration of the last conventional balloon angioplasty was 2.5 months.
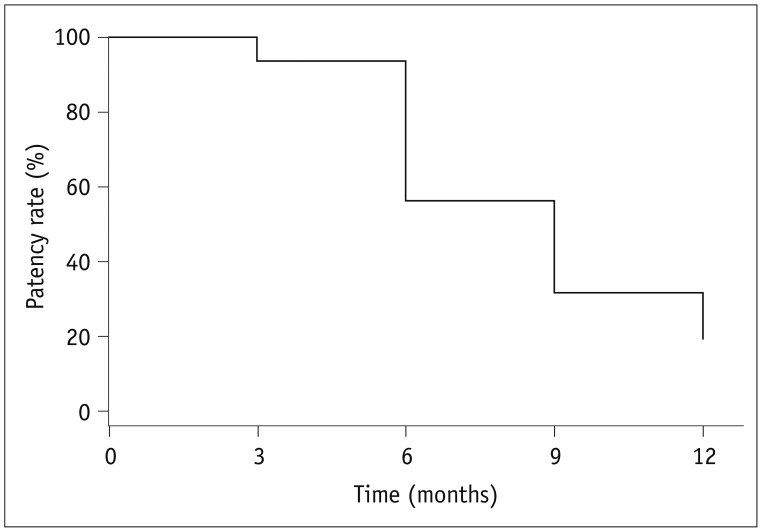
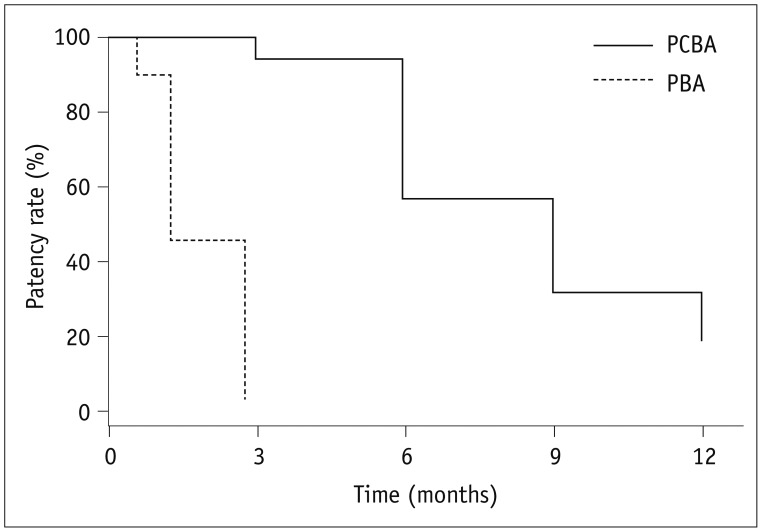
Procedural success was achieved in all 16 cases of central vein stenoses. There were no procedure-related complications. The mean circumferences of the ipsilateral arms before angioplasty and after angioplasty at 6 months and 12 months were 30.8 ± 4.6 cm, 27.2 ± 3.6 cm, and 26.8 ± 2.4 cm, respectively. The mean diameters of the central veins before angioplasty, immediately after the procedure and at 6 months and 12 months after the procedure were 3.7 ± 2.4 mm, 11.4 ± 1.8 mm, 7.8 ± 1.3 mm, and 6.9 ± 2.7 mm, respectively. All patients had undergone normal hemodialysis without any complications after the initial procedure. Primary patency rates at 6 months and 12 months were noted in 15 patients and 5 patients, respectively (Figs. 2, 3). One patient had significant restenosis of the central vein at the 3-month follow-up (Fig. 4). He was treated with a venous stent at the stenotic site. The median primary patency duration was 9 months and it was longer than the period of patency of 2.5 months with the previous conventional balloon (p < 0.001) (Fig. 5). The median primary patency durations of the right and left central veins were 7.5 months and 9 months, respectively (p = 0.809).
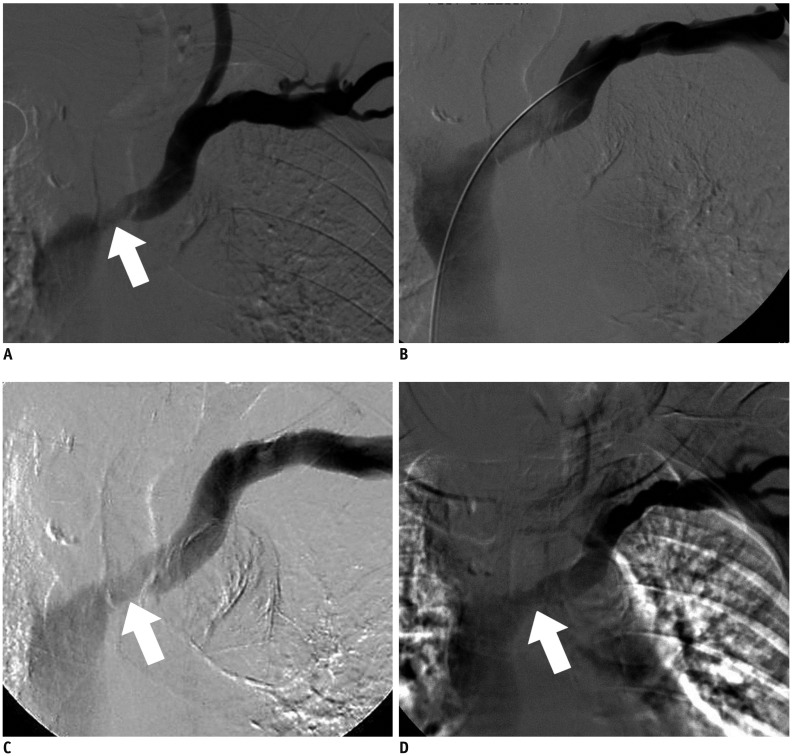 | Fig. 355-year-old patient with early recurrent significant stenosis of left brachiocephalic vein
A. Initial angiography shows significant stenosis of left brachiocephalic vein (arrow). B. Immediate angiography after procedure shows no stenosis of left brachiocephalic vein. C. Angiography at 6 months shows no recurrent stenosis (arrow). D. Angiography at 12 months shows no significant stenosis (arrow).
|
 | Fig. 465-year-old patient with early recurrent significant stenosis of left subclavian vein
A. Initial angiography shows severe stenosis of left subclavian vein (arrow). B. Immediate angiography after procedure shows no stenosis of left subclavian vein. C. Angiography at 3 months shows significant restenosis of left subclavian vein (arrow).
|
Go to :
DISCUSSION
The most common cause of central vein stenosis is a long-term central dialysis catheter, which results in chest wall and ipsilateral upper extremity swelling, engorged collateral veins, venous hypertension, and dialysis dysfunction. Endovascular treatment with conventional plain balloon angioplasty is a practical first-line treatment. However, restenosis occurs within a short period of time. Several studies have reported a primary patency rate ranging from 23% to 55% at 6 months and a rate ranging from 12% to 50% at 12 months (12131415). According to the NKF-KDOQI guidelines (5), stenting in the central vein is indicated in case of elastic recoil or recurrent stenosis within a 3-month period, which can prolong the patency time. Previous studies have shown that a bare metallic stent provided superior results for primary patency of 42–89% at 6 months and 14–73% at 12 months compared to plain balloon angioplasty (41516). However, multiple episodes of instent stenosis will decrease the patency duration due to neointimal hyperplasia. In this study, all cases had a history of early restenosis within 3 months after the last plain balloon angioplasty. The cause was progressive hyperplasia. Stent graft placement in the central vein is another option for treating the stenosis. The results for primary patency duration of stent graft placement varied from 32% to 67% at 12 months (1718). Even though stent graft has reduced the episodes of in-stent stenosis, stenosis of the stent can be frequently found at the distal and proximal ends of the stent due to in-growth of neointima. At our institution, we do not use a stent graft in central vein stenosis, because we believe that when thrombosis of a stent graft occurs, the collateral venous drainage is blocked, which results in linical symptoms of venous hypertension that would be more severe than placement of a bare metallic stent. In addition, the cost of a stent graft is higher.
Paclitaxel is an antiproliferative agent which can reduce neointimal hyperplasia of the vascular wall. A low dose of this agent causes cell cycle arrest in the G1 phase without apoptosis of the cells. This cytostatic effect results in reduction of neointimal hyperplasia due to inhibition of smooth muscle cell proliferation and migration (192021). PCBA has provided good outcomes with significant reduction in restenosis of peripheral arterial disease (6789). Moreover, a recent randomized controlled clinical trial has shown good outcomes of PCBA for stenosis in dialysis access (1022). Other recent non-randomized studies have also reported good outcomes of PCBA for the treatment of stenosis of native dialysis fistula and in-stent stenosis of dialysis fistula (2324).
Currently, there is lack of data on PCBA for the treatment of central vein stenosis possibly because of the narrow range of commercially available sizes of drug-coated balloons. Additionally, drug-coated balloons are also expensive. Only one study by Massmann et al. (1) showed that PCBA provided significantly greater freedom from target tissue revascularization than conventional balloon angioplasty (10 months vs. 5 months, p < 0.05). In this study, primary patencies at 6 months and 12 months were found in 15 of 16 lesions (93.8%) and 5 of 16 lesions (31.2%). However, angiogram showed significant restenosis of the left subclavian vein in one patient at 3 months. The subclavian vein has a high chance of external compression by the clavicle and the first rib. Therefore, in this case, the reason for early significant restenosis was possibly repetitive injury to the vein wall resulting in aggressive growth of endothelial cells. The median duration of development of significant restenosis after PCBA in this study was 9 months. This result was better than the median duration of 2.5 months when previous plain balloon angioplasty was performed for the same lesions. Further, the median time to significant restenosis after PCBA in this study was less than that in the study by Massmann et al. (1), which reported a median time of 12 months. The reason for this occurrence was possibly the use of two smaller drug-coated balloons (diameter 6–7 mm) with overlapping techniques, whereas the study by Massmann et al. (1) used a larger drug-coated custom-made balloon (diameter 10–14 mm) that provided better contact with the vascular wall surface which resulted in an increased chance of drug delivery into the venous wall. In our country, larger diameters of drug-coated balloons are not available. The largest available diameter of a drug-coated balloon in our country is 7 mm. In our opinion, even though we used two overlapping drug-coated balloons, their chemical effect was possibly not adequate enough, because some parts of the venous wall may not have come in contact with the drug-coated balloons. Additionally, some stenotic lesions still had residual resistance to the two small drug-coated balloons with the overlapping technique. For these two aforementioned reasons, a mechanical effect of a bigger high pressure balloon is needed to regain patency of the venous lumen.
This study had some limitations. First, this study used a retrospective design with a small number of enrolled patients. Second, the results were obtained from a single center. Third, we used two small-diameter drug-coated balloons that caused partial contraction of the venous wall. Fourth, this study lacked consistency in patient selection. We included recurrent stenosis of both native central veins and intra-stent central veins, which possibly caused inhomogeneous results. Lastly, there was no direct statistical comparison between the plain balloon angioplasty and PCBA groups.
In summary, PCBA can improve the patency rate in cases of early significant restenosis of the central veins. Although, the results of this study were positive in terms of an increase in the primary patency duration, a further randomized control trial of PCBA for recurrent central vein stenosis is necessary.
Go to :
 XML Download
XML Download