

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Secondary hypertension is the term embracing hypertension related to a specific etiology. It accounts for about 10% of all hypertensive patients (12). It should be suspected in cases of new or sudden onset of hypertension in patients before the third or after the sixth decade of life, persistent hypertension despite medication, or patients with typical signs and symptoms indicating specific disorders (3). Common etiologies of secondary hypertension can be categorized in accordance with the anatomy or physiology as follows: renal parenchymal diseases, renovascular stenosis, other vascular diseases, endocrinologic disturbances, diseases of the central nervous system, obstructive sleep apnea, and drug- or diet-related conditions (4).
Secondary hypertension is clinically important because identifying its etiology and treating the condition can effectively lower the blood pressure (56). However, routine screening for secondary hypertension is neither essential nor cost-effective due to its low prevalence. Radiologists should understand the role of each imaging modality and be familiar with the appropriate selection of diagnostic tests and their findings to help the referring physicians in prompt identification of patients with treatable causes. Therefore, in this article, we present the roles of multiple imaging modalities and typical imaging findings indicating a specific etiology of secondary hypertension. We also present a diagnostic algorithm consisting of patients' symptoms, laboratory findings and appropriate imaging modalities, depending on the specific condition of secondary hypertension.
Diagnostic Algorithm for Identifying Causes of Secondary Hypertension
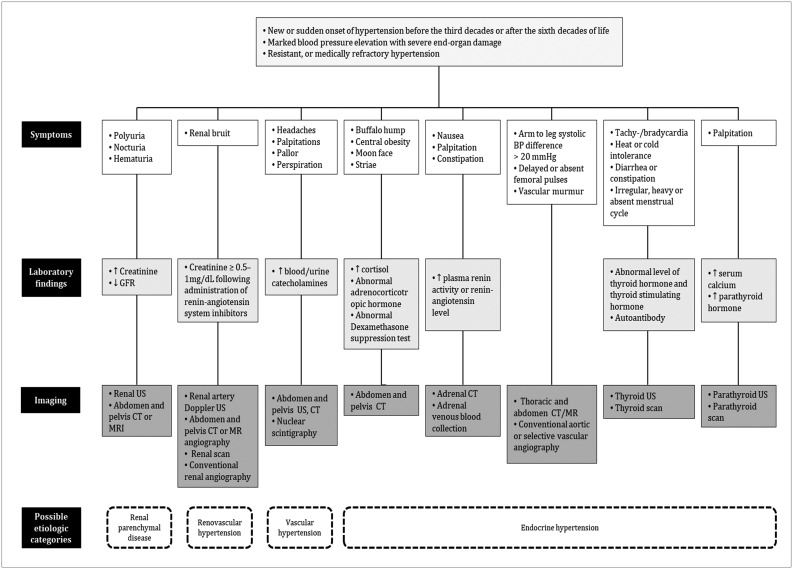
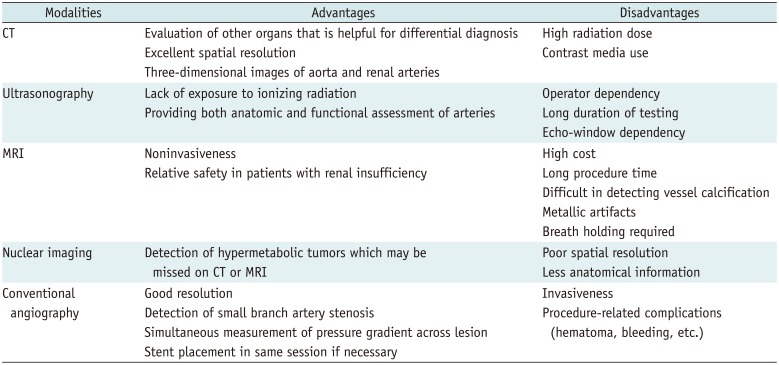
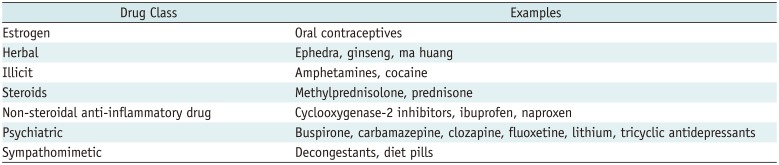
Once the patient is identified as being hypertensive, detailed history taking and physical examination should be performed to determine if it is related to a specific cause. Some clinical symptoms and signs may provide clues. Laboratory findings and multimodality imaging further discriminate specific causes. Figure 1 illustrates a flow chart consisting of patients' symptoms, laboratory findings, and appropriate imaging modalities depending on each specific condition of secondary hypertension. Before conducting diagnostic tests, keeping the pros and cons of each diagnostic modality in mind can prevent patients from undergoing unnecessary tests and thereby protect them from potential harm (Table 1). Some medications may have hypertensive effects, and therefore, the possibility of drug-induced hypertension should be excluded during the initial history taking (Table 2) (4).
Multimodality Imaging Spectra in Patients with Secondary Hypertension
Renal Parenchymal Diseases
This entity consists of up to 80% of all categories of secondary hypertension (78), and accounts for 2–5% of all causes of hypertension. A vicious cycle is formed where chronic kidney disease (CKD) and hypertension aggravate each other (9). Thus, early application of antihypertensive agents intervening in the renin-angiotensin-aldosterone (RAA) system, such as angiotensin-converting enzyme inhibitors or angiotensin receptor blockers, is important (10). Renal parenchymal hypertension is suspected when a hypertensive patient shows proteinuria, hematuria, elevated blood urea nitrogen and creatinine, and decreased glomerular filtration rate. Renal ultrasonography (US) or computed tomography (CT) is considered for morphological evaluation of the kidneys (4). Diabetic nephropathy, glomerulonephritis, nephrosclerosis and polycystic kidney disease (PKD) are common causes in this subgroup.
Chronic Glomerulonephritis
Three factors are known to contribute to hypertension in chronic glomerulonephritis: 1) sodium and water retention, 2) excessive activity of the RAA system, and 3) increased sympathetic tone (1112). Therefore, diuretics, calcium channel blockers or RAA system inhibitors are indicated for the treatment of this entity. Renal transplantation can be considered in refractory cases.
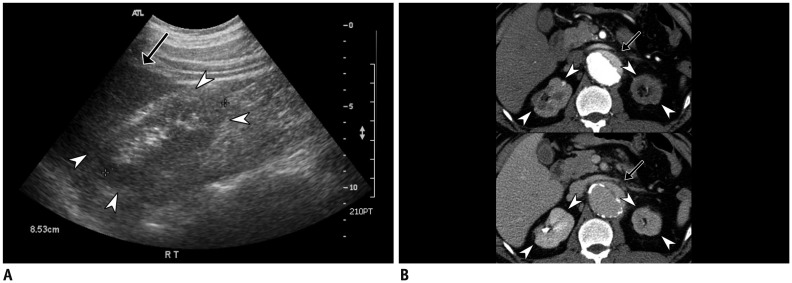
Ultrasonography demonstrates increased parenchymal echogenicity compared to that of the liver and spleen, with a small kidney, defined as the one less than 9 cm in length, or the one smaller than its counterpart with discrepancy greater than 1.5 cm (13). CT depicts cortical thinning and irregularities in the kidneys with atrophic changes (Fig. 2).
Polycystic Kidney Disease
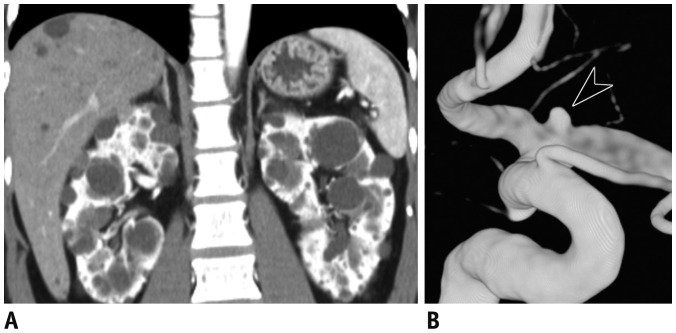
Polycystic kidney disease is inherited either in an autosomal dominant or recessive manner, with the former being much more common (14). It is characterized by progressive development of numerous renal cysts with gradual decline in renal function. Nearly all patients meeting the criteria for CKD and 60% of patients with preserved renal function develop hypertension (1516). US and CT show well-defined, thin-walled bilateral renal cysts, along with cysts in other organs such as liver, ovary, spleen, seminal vesicles, prostate and pancreas depending on the type. In patients with a history of prolonged dialysis, increased incidence of renal cell carcinoma is reported, and thus, their renal cysts may be followed-up on the basis of Bosniak classification (17) (Supplementary Table 1 in the online-only Data Supplement).
About 10–20% of the patients with autosomal dominant PKD have accompanying intracranial aneurysms (18). Therefore, brain CT or magnetic resonance (MR) angiography is indicated for evaluation of the presence and size of a cerebral aneurysm in patients with a family history of hemorrhagic stroke (Fig. 3) (1920).
Renovascular Hypertension
Steno-occlusion of the renal artery accounts for about 1% of all hypertensive cases (21) and it affects 15–30% of patients with renovascular disease (22). Renovascular hypertension is mediated by renin and occurs in response to renal ischemia. Physical examination may detect an abdominal bruit, and imaging modalities would demonstrate kidney size discrepancy.
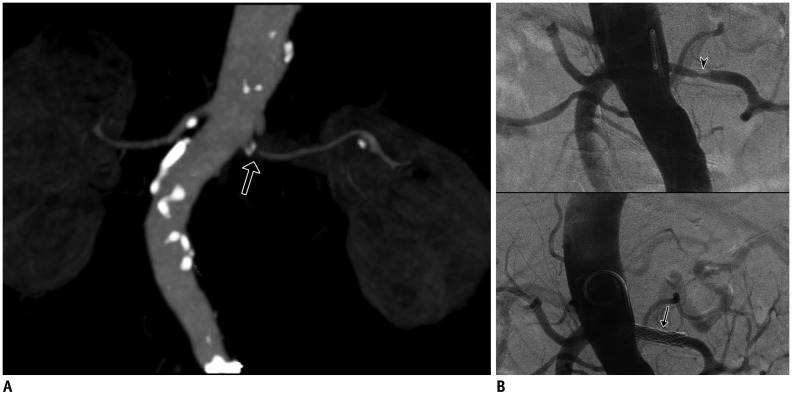
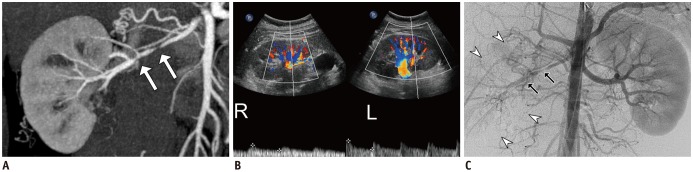
The most common etiology differs according to the age group: atherosclerosis in the elderly, and fibromuscular dysplasia (FMD) in the young group. An atherosclerotic change is characterized by progressive luminal stenosis mainly involving the renal arteries, along with other arteries because of its systemic nature. When it affects the renal arteries, it typically involves the proximal segment, within 2 cm from the ostia (Fig. 4) (22). On the other hand, FMD affects the middle or distal segment of the renal arteries. It is an idiopathic vascular disorder with a predilection for renal arteries in young adults, and it occurs more often in females than in males (23). The characteristic “string of beads” appearance of the affected artery represents alternating segments of thin and thick portions of the collagen-containing medial layer, and it is observed in the medial dysplasia type (Fig. 5). Other types such as intimal fibroplasia or adventitial fibroplasia may appear as smooth, concentric stenosis or even aneurysm. Doppler US may reveal a decreased flow with the pulsus tardus et parvus wave pattern.
Although CT or MR angiography effectively assesses renovascular stenosis, conventional angiography is occasionally necessary for obtaining higher resolution in validating branch vessels (24). Conventional angiography is also essential when a therapeutic option, such as transluminal angioplasty, is considered (Fig. 4). Caution is advised when patients with compromised renal function undergo contrast-enhanced imaging, as iodine or gadolinium based contrast media is a known risk factor for contrast-induced nephropathy and nephrogenic systemic fibrosis, respectively (2526). For these patients, MR angiography without contrast material or Doppler US can be an alternative.
Vascular Hypertension
Diseases affecting blood vessels other than renal arteries can also manifest as hypertension. Any condition causing steno-occlusion of the aorta is included in this entity, such as coarctation of the aorta (COA), aortitis, or systemic diseases that may affect the blood vessels (4). Common clinical vignettes include audible bruits over the neck, chest, or abdomen, and difference in blood pressure between the upper and lower extremities (27).
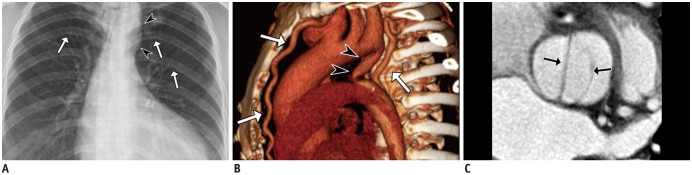
Coarctation of the aorta is a constrictive congenital anomaly of the aorta and the second most common cause of hypertension in children and young adults (28). The incidence of hypertension increases rapidly as patients get older, and it is reported to be 1.36% in the pediatric age group and 28.9% and 45.7% in the age groups of 20 to 29 and 30 to 39 years, respectively (29). It is classified into the preductal and postductal types, according to the location of the coarctation in relation to the ductus arteriosus (3031). Other frequently associated cardiovascular anomalies are bicuspid aortic valve, ventricular septal defect, mitral valve anomalies, and even cerebral aneurysm (32). It is known that 15% of Turner syndrome patients present with COA (33). Clues on a chest radiograph include left ventricular hypertrophy, small aortic arch contour and/or notching of the ribs. CT or MR demonstrates location of the stenotic portion, various collaterals, and other associated anomalies (Fig. 6). Early detection and surgical correction are warranted to achieve a better prognosis. If left unrepaired, the mortality reaches as high as 90% at age 50 (34).
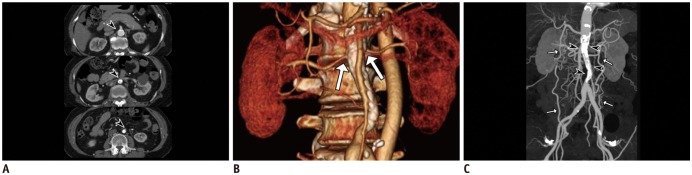
The mid-aortic dysplastic syndrome is a type of COA, which is characterized by segmental narrowing of the distal thoracic or abdominal aorta, or both, either due to a congenital or an acquired cause (35). Incomplete fusion or overfusion of embryonic dorsal aortas during fourth week of gestation is thought to be a congenital cause, whereas Takayasu arteritis, neurofibromatosis (NF), FMD, retroperitoneal fibrosis are common causes in acquired cases (3637). Renal artery involvement is common in these patients, and the main cause of death is the cardiovascular complication arising from progressive hypertension (36). CT, MR or conventional angiography shows characteristic segmental narrowing of the aortic mid-portion with involvement of visceral branches such as the renal or superior mesenteric artery. Depending on chronicity, various collaterals may develop via internal mammary, epigastric and circumflex iliac arteries (Fig. 7). Characteristic CT findings in acquired cases include vascular calcification and/or concentric vascular wall enhancement (38).
Endocrine Hypertension
The endocrinologic etiologies comprise about 3% of secondary hypertension cases. They are characterized by excessive hormone secretion, and in many cases, they are correctable unless the diagnosis is made after end organ damage occurs. Screening tests targeting excessive hormones have a relatively higher diagnostic performance than those targeting other causes of secondary hypertension (39).
Primary Aldosteronism
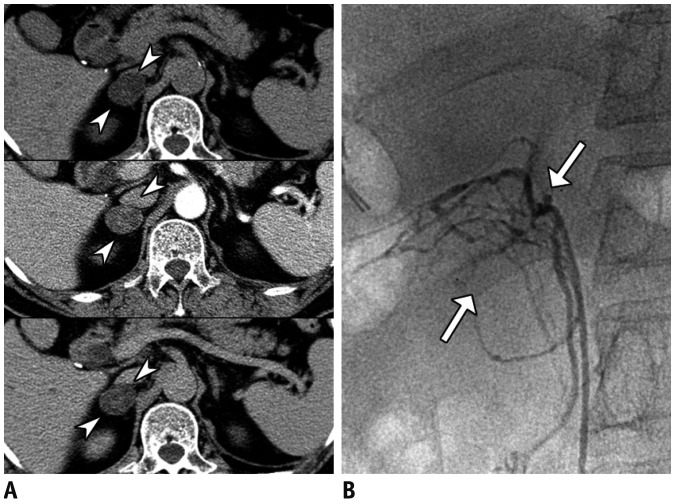
Primary aldosteronism is characterized by excessive aldosterone secretion from adrenal adenoma or bilateral adrenal hyperplasia. Patients present with hypertension and hypokalemic metabolic alkalosis with an absence of a history of diuretic therapy (4041). Plasma aldosterone/renin ratio ≥ 20 sensitively indicates this condition (42).
When lipid component is evident within the adrenal mass on precontrast CT or chemical shift MR imaging, benign lesions including adenomas are readily diagnosed (4344). However, when an adrenal incidentaloma is lipid-poor, multiphasic contrast-enhanced CT is usually required. The following formulae named absolute percentage washout (APW) and relative percentage washout (RPW) are utilized for characterization of an adrenal incidentaloma (45):
APW = 100 × (venous attenuation − delayed attenuation) / (venous attenuation − precontrast attenuation)
RPW = 100 × (venous attenuation − delayed attenuation) / venous attenuation
Venous attenuation refers to the CT number obtained in the portal venous phase, usually acquired within 70–90 seconds after contrast administration. Delayed attenuation is obtained from the time period varying between 5 and 15 minutes after contrast injection depending on the researcher's need (4647). The diagnostic accuracy of APW greater than 60 and RPW greater than 40 for diagnosing adrenal adenoma was found to be 94.2% for lipid-poor adrenal incidentaloma (48). When MR and CT are inconclusive, radionuclide studies and/or adrenal venous sampling can be considered (Fig. 8) (49) .
Cushing's Syndrome
Cushing's syndrome is characterized by autonomous and excessive secretion of cortisol. It should be considered when a hypertensive patient presents with central obesity, moon face, buffalo hump, or red striae. Less specific features include diabetes mellitus, dyslipidemia, osteoporosis, and urolithiasis, with laboratory clues being eosinopenia and hypokalemia (39).
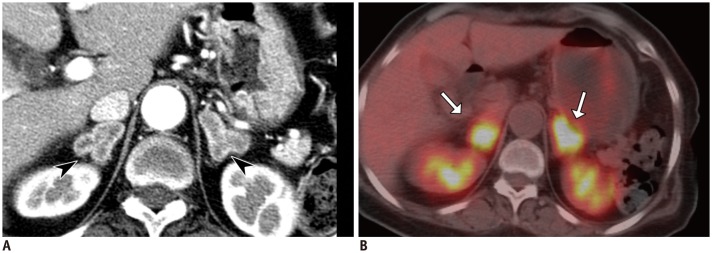
Excluding exogenous corticosteroid use, which is the most common cause of Cushing's syndrome, pathology can be localized anywhere in the hypothalamic-pituitary-adrenal axis (50). Pituitary MR imaging is indicated in patients with adrenocorticotropic hormone (ACTH)-dependent type of Cushing's syndrome since corticotroph adenoma of the pituitary gland comprises most of the cases (80–85%) (51). Adrenal CT should be considered to detect incidentaloma in ACTH-dependent type of Cushing's syndrome without pituitary pathology, or in ACTH-independent type (52). Patients with excessive ACTH secretion may demonstrate bilateral adrenal cortical hyperplasia with strong enhancement on CT and hypermetabolism in bilateral adrenal cortices on whole body positron emission tomography (PET) (Fig. 9).
Pheochromocytoma
Pheochromocytomas are rare tumors originating from the adrenal medulla. When they occur in the extra-adrenal paraganglia, they are referred to as paragangliomas. Due to excess of catecholamines and their metabolites, episodic headaches, palpitations, sweating and pallor develop frequently (53). The traditional “10% rule” has been known to be applicable to their extra-adrenal locations, the rate of bilaterality, multiplicity, and malignancy (54). In familial cases, they are often associated with multiple endocrine neoplasia type II, von Hippel-Lindau syndrome, and NF type I (53). Laboratory tests are performed by measuring the metanephrine level in a 24-hour urine or plasma sample.
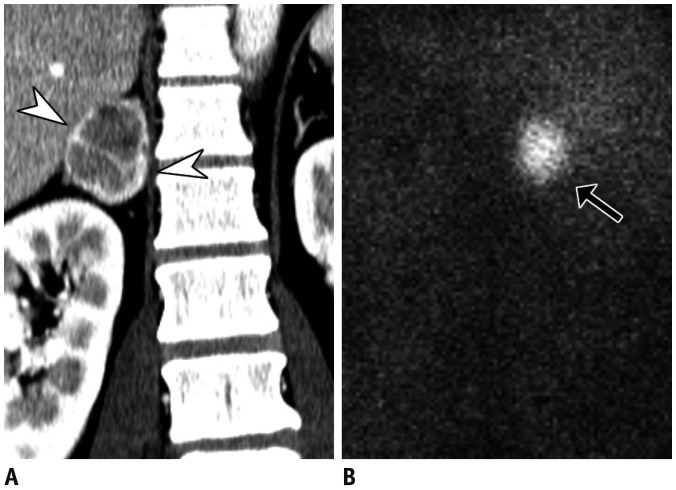
Pheochromocytomas can have a varied appearance on CT due to variable contents of fat, hemorrhage and/or calcifications, but the solid components are usually well enhanced. Typical MR findings include T1-hypo- and T2-hyperintensities. Nuclear imaging tests such as 123I-metaiodobenzylguanidine scintigraphy or PET may show high diagnostic accuracy in false-negative cases on CT or MR (Fig. 10) (55).
Thyroid Dysfunction
Either hyper- or hypothyroidism can cause systemic or pulmonary hypertension. Patients with hyperthyroidism usually manifest with systolic hypertension, via upregulation of catecholamine action and β-adrenergic receptors (56), while those with hypothyroidism show elevated diastolic blood pressure, with exaggerated sympathetic tone and α-adrenergic response (57).
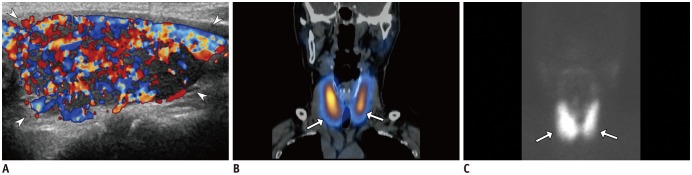
Ultrasonography is the most common imaging modality for thyroid assessment. Although thyroid dysfunction does not necessarily accompany abnormal US findings, certain etiologies of hyper- or hypothyroidism are associated with diffuse thyroid diseases or thyroiditis. In these cases, thyroid can show diffuse enlargement and heterogeneous echogenicity, with variable vascularity (Fig. 11). Nuclear scintigraphy with various radiotracers (99mTc, 131I or 123I) can be useful in the evaluation of thyroid function and metabolic activity (58).
Hyperparathyroidism
Hyperparathyroidism can be classified into primary and secondary forms. It results from either a pathologic condition of the parathyroid gland itself (adenoma, most commonly), or compensatory hyperplasia following other systemic conditions, such as CKD, vitamin D deficiency, and malabsorption in the gastrointestinal tract (59). It is estimated that 40–65% of patients with hyperparathyroidism develop hypertension (60). Since the parathyroid hormone regulates calcium metabolism, patients may manifest with nephrolithiasis, hypercalciuria, and overt skeletal diseases.
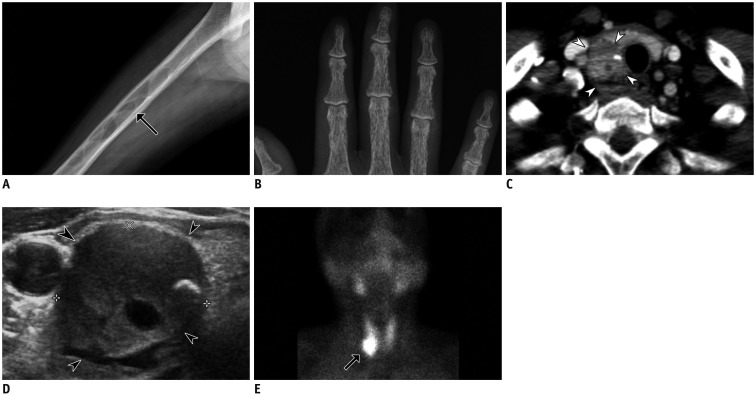
When a nodule exceeding 1 cm in size is found in an extrathyroid location on US or CT, parathyroid adenoma or hyperplasia can be suspected (61). Sestamibi scan is commonly used because it is taken up more avidly and retained longer by adenomatous and hyperplastic parathyroid than by the thyroid tissue. Therefore, characteristics of hyperfunctioning parathyroid tissue are clearly noted on delayed images, approximately 2 hours after Sestamibi administration (61). Plain radiographs can be helpful in assessing the skeletal manifestation, including subperiosteal resorption, rugger-jersey spine, and brown tumors. Parathyroid adenomas are hypoechoic compared to the overlying thyroid gland on gray-scale US due to relative hypercellularity. Multiphase CT may be useful for detection of the adenoma; a precontrast scan may discriminate hypodense adenoma from iodine-rich thyroid gland, while an enhanced scan may show a hypervascular nature. Larger lesions may show heterogeneous attenuation or calcifications (Fig. 12) (62).
CONCLUSION
Common causes of secondary hypertension include renal parenchymal diseases, renovascular stenosis, vascular diseases, and endocrinologic disturbances. Although some clinical vignettes strongly indicate secondary hypertension, imaging workup is essential for the differential diagnosis as symptoms are often nonspecific. US can be the initial modality of choice for renal parenchymal disease, renovascular hypertension, thyroid and parathyroid dysfunctions. CT is widely used for evaluation of renal parenchyma, adrenal incidentalomas, thyroid or parathyroid nodules, as well as for vascular assessment in cases of vascular or renovascular diseases. MR can be an alternative in patients who have difficulty in undergoing CT. MR angiography without contrast media can be recommended for patients with renal dysfunction. Conventional angiography can be used not only for diagnosis but also for therapeutic revascularization in patients with vascular or renovascular hypertension. Nuclear scan with various radiotracers can provide further information on the function of endocrine organs. Radiologist should be familiar with the role of each imaging modality and the characteristic findings of each cause of secondary hypertension, and they should select.
 XML Download
XML Download