

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Peripheral arterial disease (PAD) affects 12–16% of the population over the age of 60. Intermittent claudication, its primary symptom, is detrimental to the patients' quality of life (1234). Typically, PAD follows a stable course as management is confined to conservative measures. One in ten PAD patients will develop critical limb ischemia, with the all-cause mortality in the critical limb ischemia cohort rising to 50% at 5 years (567). Ultrasonography (US) is safe, inexpensive, and can provide functional information about vessel stenosis. However, US is a less sensitive technique for imaging native vessel stenosis compared with CT angiography (CTA). However, the greatest limitation of US is the time required for evaluation of lower extremity (LE) (8). LE-CTA is the primary diagnostic imaging modality for PAD because of its high spatial resolution. However, intravascular contrast enhancement must be adequate for an accurate evaluation of the distribution and the severity of the lesions. A recent single-center study evaluated the diagnostic performance of 64-slice CTA, compared with invasive digital subtraction angiography for detection of stenosis > 70% on a per segment basis. CTA had an accuracy of 98%, a sensitivity of 99%, and specificity of 97% (9).
A fixed contrast medium dose and a fixed rate of contrast medium administration are widely used for LE-CTA. However, contrast enhancement is affected by patient characteristics including their age, sex, body size, cardiac output (CO), and other pathologic conditions (10). Acquisition parameters such as table movement speed and circulating time must be considered. The contrast injection time and the image acquisition time may have to be adjusted to slow down or time data acquisition to slower blood flow rates in PAD patients undergoing LE-CTA (11). Therefore, the effect of patient characteristics on vessel enhancement may differ between LE-CTA and other CTA studies. The evaluation of such effects is important. A literature search found no multivariate analyses that examined these issues. The researchers evaluated the effect of various patient characteristics on vessel enhancement at LE-CTA.
Go to : 
MATERIALS AND METHODS
This prospective study received Institutional Review Board approval. Prior informed consent to participate was obtained from all patients.
Study Population
Between March and June 2015, 170 patients were considered for participation in this prospective study. The inclusion criteria were 1) suspected PAD based on an ankle bronchial pressure index lower than 0.9 or intermittent vascular claudication; 2) no amputation of the lower limbs; 3) no renal failure (estimated glomerular filtration rate > 45 mL/min/1.73 m2) and no hemodialysis; and 4) no history of allergic reactions to iodinated contrast medium. The research excluded 14 patients with allergic reactions to iodinated contrast (n = 1), renal failure (n = 2), amputation (n = 9), and less than 40 kg lower body weight (n = 2). Consequently, 156 patients (98 men, 58 women aged from 43–96 years, mean 73.3 years) were enrolled.
Scan Protocol and Image Reconstruction
All patients were scanned with a 64-detector row CT scanner (LightSpeed VCT; GE Healthcare, Milwaukee, WI, USA). LE-CTA was performed from the celiac artery to the toes in the craniocaudal direction (12). The scanning parameters were 0.5-seconds rotation, 1.25-mm detector row width, 0.516 beam pitch, 41.2-mm table movement, and 50-cm scan field of view. The tube voltage was 100 kVp. The tube current was changed from 100–770 mA to maintain the image quality (noise index, 14) using automatic tube current modulation. The scan length along the z-axis ranged from 110–140 cm depending on the body size. The scanning time varied from 29.0–31.0 second.
Contrast Medium Injection Protocols
Using a power injector (Dual Shot; Nemoto-Kyorindo, Tokyo, Japan), the researchers delivered contrast medium (Omnipaque-300; Daiichi-Sankyo, Tokyo, Japan) via a 22-gauge catheter into the antecubital vein. To determine the scan timing, the researchers acquired a test-bolus scan at the patella level and obtained a time-density curve for the popliteal arteries. The test-bolus scan was comprised of serial low-dose scans (100 kVp and 50 mAs) without table movement. The inter-scan interval was 1.0 second. The contrast medium (15.0 mL) was injected at a rate of 3.0 mL/sec and followed with 20.0 mL of a saline solution delivered at the same injection rate. Acquisition of the dynamic monitoring scans began 18.0 second, after the start of contrast medium injection. To obtain a time attenuation curve, the researchers placed a region of interest (ROI) in the popliteal arteries at the patella level. When there was a difference in the peak time of the popliteal arteries, a performance was executed on the main scan using mean peak time of both popliteal arteries. The scan start time was defined as the arrival time plus 5.0 second, based on the time-enhancement curves of the test-bolus scan.
For LE-CTA, 85.0 mL of the contrast medium were intravenously administered at an injection rate of 3.0 mL/sec. This was followed with 20.0 mL of a saline solution delivered at the same injection rate.
Data Analysis
The ROI of popliteal arteries was measured by one observer. However, one observer measured of popliteal artery at the patella level by 3 times. To clarify, the researchers rewrote the following sentence in material and method.
The researchers measured the CT number of the popliteal artery at the patella level by 3 times on 3 consecutive slices for all patients, and all CT numbers were averaged (Fig. 1). The mean CT number and the scan delay at the popliteal artery were recorded in the 158 patients undergoing LE-CTA. An attempt was made to maintain a constant ROI area of approximately 7.0 mm2. The ROI range was 3.1–12.6 mm2. The researchers acquired the patients' age and sex from their electronic health records. Their total body weight (TBW) and height (HT) were measured prior to CTA scanning. The patients' CO was continuously displayed on a non-invasive CO monitor (Aesculon mini; Ospyka Medical, Berlin, Germany). The average CO during 30 valid cardiac cycles was recorded.
 | Fig. 1CT attenuation measurement in popliteal artery.
A. Volume-rendering image of at LE-CTA in 77-year-old man. B. Maximum-intensity projection at LE-CTA. C. Measurement sites of volume rendering image for popliteal arteries at level of patella. D. Measurement sites of axial image for popliteal arteries at level of patella. CT = computed tomography, LE-CTA = lower extremity CT angiography
|
Because others (1314) had suggested that protocols tailored to the body surface area (BSA) and lean body weight (LBW) reduced the effect of the body size on aortic enhancement, the research study also evaluated the body mass index (BMI), BSA, and LBW. The researchers used the Mosteller formula (15) to calculate the BSA {BSA (m2) = (square root of the product of the weight [kg] × HT [cm] / 60)}. The LBW (1617) was calculated with the formula (1.10 × W) − {128 (W2 / [100 × H]2)} for men and (1.07 × W) − {148 (W2 / [100 × H]2)} for women, where W is the weight in kilograms and H is height in meters.
Statistical Analysis
All continuous variables were presented as the mean ± standard deviation. The researchers used Student's t test to compare continuous variables and the chi square- and the Fisher exact test to compare categorical and skewed variables. The relationship between the patients' age, sex, TBW, BMI, BSA, LBW, CO and the scan delay and CT number of the popliteal artery was investigated using univariate linear regression analysis. The researchers calculated the Pearson product moment correlation coefficient (r) to assess the strength of associations. Then, they selected one representative index (TBW, BMI, BSA, or LBW) for multivariate regression analysis by the Pearson product moment correlation coefficient because the correlation coefficient between these factors tends to be very high, and multi-colinearity can result in wide confidence intervals and anomalous p values for independent variables. The Welch t test was used to compare the CT number of the popliteal artery on LE-CTA images of males and females.
To determine independent factors (i.e., the age, HT, BSA, CO and scan delay) with an effect on the enhancement and CT number of the popliteal artery, the researchers performed multivariate linear regression analysis. The researchers used the standardized coefficient (β) to assess the strength of associations in multivariate linear regression analysis.
Variables with p values less than 0.05 were considered statistically significant. Statistical analyses were with the free statistical software “R” (R, version 3.2.2; The R Project for Statistical Computing; http://www.r-project.org/). A nomogram was formulated based on the results of the binomial logistic model, by using the “rms” package in “R.”
Go to :
RESULTS
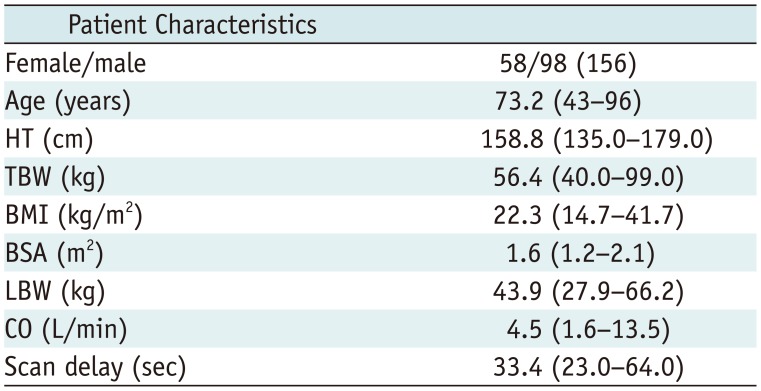
A summary of the patient characteristics is presented in Table 1. Of the 156 patients, 58 were female and 98 were male, their age ranged from 43 to 96 years (mean, 73.2 ± 9.9 years), the HT from 135.0 to 179.0 cm (mean, 158.8 ± 8.4 cm), and the TBW from 40.0 to 99.0 kg (mean, 56.4 ± 11.9 kg). The BMI ranged from 14.7 to 41.7 kg/m2 (mean, 22.3 ± 3.9 kg/m2), the BSA ranged from 1.2 to 2.1 m2 (mean, 1.6 ± 0.2 m2), the LBW from 27.9 to 66.2 kg (mean, 43.9 ± 7.8 kg), and the CO from 1.6 to 13.5 L/min (mean, 4.5 ± 1.8 L/min). The scan delay ranged from 23.0 to 64.0 second (mean, 33.4 ± 8.2 sec).
Univariate Linear Regression Analysis
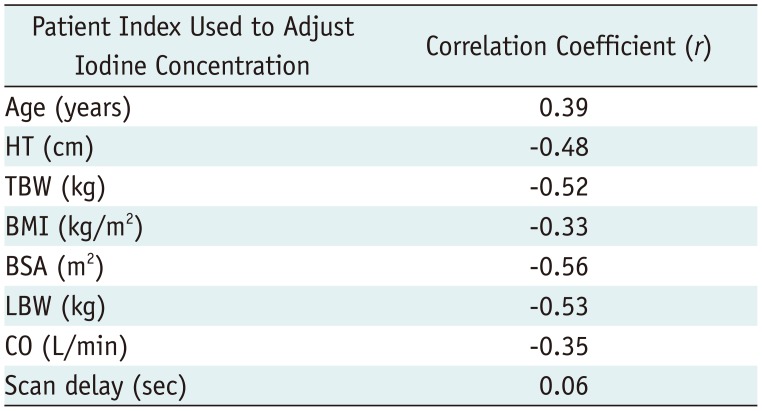
Univariate linear regression was used to assess the association between the CT number of the popliteal artery (dependent variable) and all contrast enhancement parameters (independent variables), except the scan delay. A significant positive correlation was seen between the CT number of the popliteal artery and the patient age (r = 0.39, p < 0.01). Linear regression analysis revealed an inverse correlation between the CT number of the popliteal artery and the HT (r = −0.48), TBW (r = −0.52), BMI (r = −0.33), BSA (r = −0.56), LBW (r = −0.53), and CO (r = −0.35) by linear regression analysis (p < 0.001 for all) (Table 2). There was no significant correlation between enhancement and scan delay (r = 0.06, p = 0.47) (Fig. 2). The mean CT number of the popliteal artery was significantly higher in females than males (460.4 ± 75.9 vs. 400.6 ± 80.0 Hounsfield units, p < 0.01). The researchers used the BSA as a representative index of the body size for multivariate regression analysis because its correlation coefficient was higher than that of the TBW, BMI and LBW.
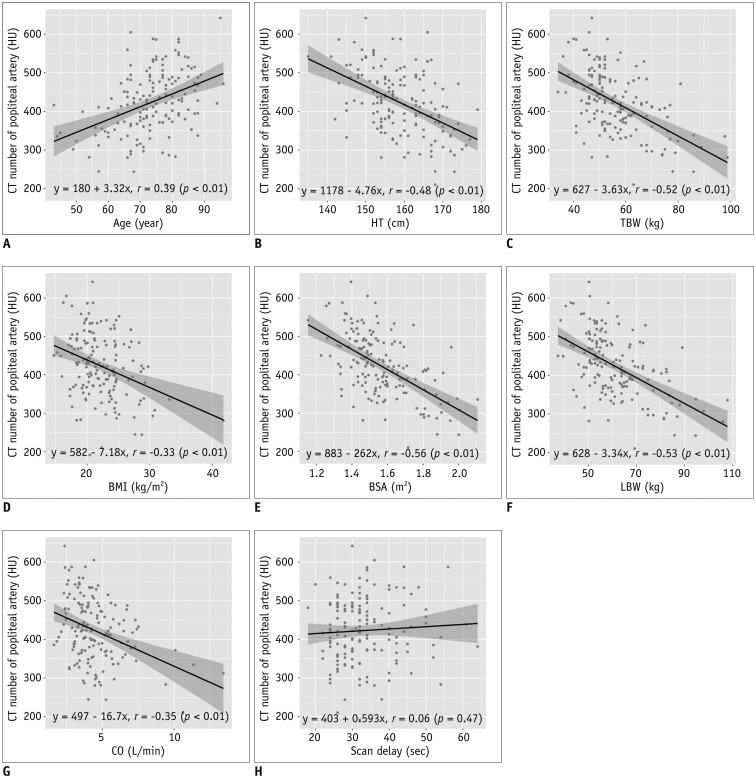 | Fig. 2Relationship between popliteal arterial enhancement and patient characteristics.Scattergrams of relationship between arterial enhancement obtained with protocol, using fixed dose of iodinated contrast material and patient age (A), HT (B), TBW (C), BMI (D), BSA (E), LBW (F), CO (G), and scan delay (H). There was significant positive correlation between CT number of popliteal artery and age (r = 0.39, p < 0.01). Correlation was inverse with HT (r = −0.48), TBW (r = −0.52), BMI (r = −0.33), BSA (r = −0.56), LBW (r = −0.53), and CO (r = −0.35) by linear regression analysis (p < 0.01 for all). There was no significant correlation between vessel enhancement and scan delay (r = 0.06, p = 0.47). BMI = body mass index, BSA = body surface area, CO = cardiac output, HT = height, HU = Hounsfield units, LBW = lean body weight, TBW = total body weight
|
Table 2
Effect of Age, HT, TBW, BMI, BSA, LBW, CO, and Scan Delay on CT Number of Popliteal Artery
![]()
Multivariate Linear Regression Analysis
Using multiple linear regression analysis, the patient's age, sex, BSA, CO, or the scan delay was the independent variable to avoid overestimating potentially linked variables. Table 3, which shows a multivariate linear regression analysis, only the BSA, CO, and age maintained their independent predictive values (BSA and CO, p < 0.001; age, p = 0.030). Standardized regressions (BSA, −0.49; CO, −0.24; age, 0.16) suggested that the effect of the BSA was higher than the other variables.
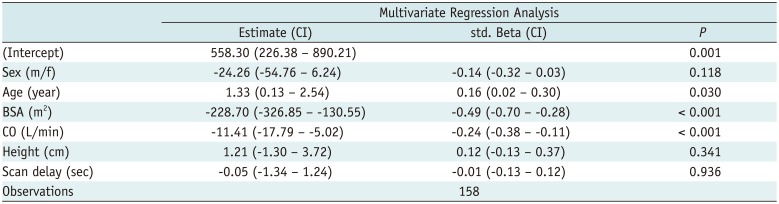
Table 3
Multivariate Linear Regression Analysis of Effect of Patient Characteristics on CT Number of Popliteal Artery
![]()
Go to :
DISCUSSION
The study suggested that by using univariate linear regression analysis, the patient age, HT, TBW, BMI, BSA, LBW, and CO were significantly related to CT number of the popliteal artery on LE-CTA images without scan delay. However, multivariate linear regression analysis demonstrated that patient BSA, CO, and age significantly affected enhancement of the popliteal artery on LE-CTA images.
Most importantly, the research found that the BSA and CO strongly affected popliteal artery enhancement, although the patient age maintained an independent effect. According to Bae (10), the blood volume and CO directly affect the enhancement of vessels, by contrast media while other patient characteristics have an indirect effect and manifest a complex relationship. Others (1819) have suggested that enhancement is increased in elderly patients. However, most earlier studies did not perform multivariate regression analysis or did not include the CO as an independent factor in their multivariate linear regression analysis. Consequently, whether the patient age affects vessel enhancement indirectly due to a change in the CO remains controversial. The research included the CO measured with a portable electrical velocimeter as an independent variable in the multivariate linear regression analysis and found that the patient age had some effect on their CO, and therefore on the enhancement of the popliteal artery. Arterial stiffness due to biological aging and arteriosclerosis (20) is related to the blood flow and may help to explain the effect of the age on popliteal artery enhancement. The researchers think that blood flow changes in the elderly may be reflected in the observed difference in their enhancement of the popliteal arteries.
Univariate analysis showed that patient sex and HT also affected contrast enhancement. However, based on the results of multivariate linear regression analysis, they exerted no statistically significant effect on arterial enhancement per gram of iodine. Bae (10) suggested that blood volume and CO directly affect vessel enhancement by contrast media, and that there is a complex relationship between the body size, age, and sex on the one hand, and the blood volume and CO on the other. They stated that this relationship is indirectly involved in changes in vessel enhancement. The research included the BSA and CO as independent variables in the multivariate linear regression analysis and proposed that they may obscure the relationship between the other independent variables and popliteal artery enhancement.
The research observed no correlation between the CT number of the popliteal artery and the scan delay in our LE-CTA studies. Bae et al. (21) reported in the porcine model that a decrease in the CO decreased the time required for the contrast medium bolus to arrive at the aorta and that the time to peak aortic and hepatic enhancement increased. Their finding is indicative of an increase in circulation time commensurate with a decrease in the CO. The time from the start of the contrast medium injection to peak aortic enhancement is related directly to injection duration or injection rate. Since blood flow rate is slower in patients with PAD, so is the image and data acquisition time (11). Therefore, the scan delay may not affect the CT number of the popliteal artery on LE-CTA images. Using the BSA, CO, and age may help to identify patients with poor vessel enhancement on LE-CTA scans. Since many patients with PAD present with concomitant chronic kidney disease (322), the contrast material dose for CTA of the lower extremities must be as low as possible. In these patients, optimized contrast injection protocols tailored to their BSA or LBW should be considered.
In this study, the researchers used lower beam pith than general examinations, because the rapid image acquisition with modern scanners may result in suboptimal opacification of the peripheral vasculature due to insufficient time to fill the vascular tree (12). Previous reports have suggested that reducing the pitch and increasing the contrast medium injection duration offer better filling of the peripheral artery. Fleischmann recommended the fixed scan duration of 40 seconds by adjusting the pitch in the 2010 (23). Therefore, the researchers developed this protocol to optimize the contrast enhancement in the lower extremity arteries.
The study has some limitations. The range and mean BSA of our Japanese patients is lower than of North American and European individuals. This study was a single-center study and the population was small. Lastly, the researchers did not investigate the relationship between contrast enhancement and image quality. Also, the research did not evaluate the image quality with respect to the severity of PAD such as obstruction, severe narrowing, or mild narrowing. In conclusion, the patient BSA, CO, and age significantly affect the CT number of the popliteal artery on LE-CTA images.
Go to :
 XML Download
XML Download