

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Transcatheter arterial chemoembolization (TACE) is the standard treatment for patients with solitary large (tumor size larger than 5 cm in diameter) hepatocellular carcinomas (HCCs) or multinodular HCCs (12). However, the long-term efficacy of TACE is not satisfactory. In most studies, the complete tumor necrosis rate after TACE was only 10–20% and the median survival time 16–20 months (34567).
Radiofrequency ablation (RFA) is considered a safe and effective treatment for early-stage HCC (89); however, outcomes are favorable only regarding complete necrosis of tumors smaller than 3 cm (10). Microwave ablation (MWA), a method for performing thermal ablation of HCCs, has the capacity to achieve larger and faster ablations than RFA through maintaining guarded and consistently higher intratumoral temperatures (11).
Hence, alternative treatments strategies aimed at achieving better outcomes in patients with solitary large or multinodular HCCs are being explored. One such strategy is TACE plus MWA. Previous studies reported that TACE plus MWA is much more effective than conventional TACE in patients with large solitary HCCs (1213). However, to the best of our knowledge, no study has yet analyzed outcomes after TACE plus MWA in patients with large solitary and multinodular (not more than 10 tumors) HCCs.
The purpose of this study was to evaluate the clinical effectiveness and prognostic factors of TACE plus MWA in the management of large solitary and/or multinodular (not more than 10 tumors) HCCs.
Go to : 
MATERIALS AND METHODS
Patients
Our Institutional Review Board approved the use of clinical data for this retrospective study and the requirement for informed consent was waived. Between July 2011 and April 2015, a search of Henan Cancer Hospital's our institution's electronic medical records database identified 593 patients with large solitary or multinodular HCCs (with Child-Pugh class A liver function). A total of 276 patients underwent treatment with TACE+MWA or TACE alone. These two regimens were the main recommended treatments in our tertiary-referral hospital. The diagnoses of HCC were confirmed pathologically or clinically according to the American Association for the Study of Liver Diseases criteria (14). The diagnosis of liver cirrhosis was based on magnetic resonance imaging (MRI) findings, together with compatible clinical features of hypertension in the hepatic portal system, such as esophageal and gastric varices or an enlarged spleen with thrombocytopenia (15).
Inclusion criteria were: 1) aged 18–70 years; 2) Child-Pugh class A liver function; 3) HCC with a single tumor ≥ 5 cm in diameter, or 2–3 tumors with a maximum diameter > 3 cm, or 4–10 tumors regardless of size; and 4) received TACE + MWA or TACE treatment. Exclusion criteria were: 1) diffuse-type HCC; 2) HCC after surgical treatment or liver transplantation; 3) TACE combined with any treatment other than MWA, such as percutaneous ethanol injection, RFA, 125I-seed implantation, or sorafenib; 4) concomitant malignancy; and 5) lost to follow up. The inclusion criteria for ablation were: 1) patients with a large solitary tumor or with two or three nodules, each with a residual active area ≤ 5 cm in diameter after TACE treatment. 2) Patients with 4–10 HCC nodules, each nodule ≤ 3 cm in diameter. Application of these criteria yielded 258 patients who were allocated to the following two groups: TACE + MWA (n = 92) and TACE only (n = 166) (Fig. 1).
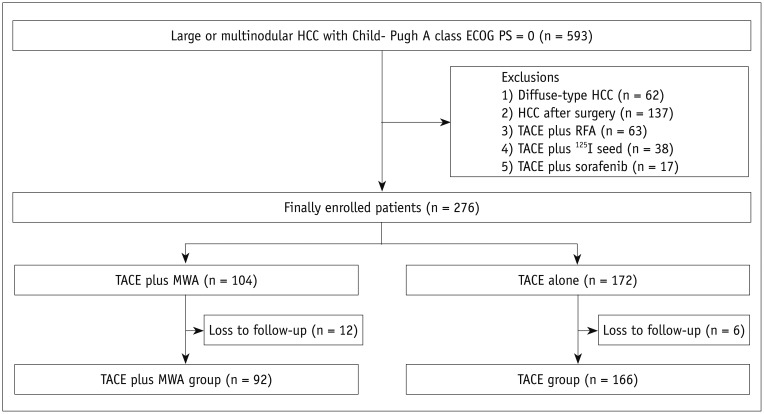 | Fig. 1Study flow chart showing selection of 258 patients who were finally included in study.Flow diagram of progress of 258 patients through enrolment, allocation, follow-up and data analysis phases of our study. ECOG PS = Eastern Cooperative Oncology Group Performance Status, HCC = hepatocellular carcinoma, MWA = microwave ablation, RFA = radiofrequency ablation, TACE = transcatheter arterial chemoembolization
|
Transarterial Chemoembolization
Transcatheter arterial chemoembolization was performed in all patients. After introduction of a 5F-RH catheter (Terumo, Tokyo, Japan) through the femoral artery, hepatic artery angiography was performed and the location, number, size, and blood supply of tumors evaluated. Next, a 2.7F micro-catheter (Terumo) was super-selectively inserted into the arteries feeding the tumors and lobaplatin (50 mg) was infused, followed by slow injection of an emulsion of epirubicin (30 mg) mixed with Lipiodol (5–15 mL). Gelatin sponge particles (150–350 µm; Alicon, Hangzhou, China) were injected until the flow was static and full saturation of the feeding arteries had been achieved (16). Liver and kidney function were evaluated 10 days after TACE prior to administering MWA to patients receiving combined therapy.
Microwave Ablation
Microwave ablation was performed approximately 10 days (range, 7–14 days) after TACE using a 16-G MWA cooled-shaft needle antenna (Eco Medical Equipment, Nanjing, China). The MWA needle was inserted to the proximal tumor margin under CT guidance, while the patient was under general anesthesia. The antenna was advanced to the distal margin through the center of each mass for tumors less than 3.0 cm in diameter. For tumors larger than 3.0 cm, an overlapping ablation technique was used to make sure that the ablation zone covered the entire tumor area. Two or three times MWA were needed for tumors larger than 5.0 cm or multinodular HCCs (4–10 tumors). The microwave power was set at 60–80 watts and the procedure lasted 5–10 minutes. Using real-time CT after the procedure, the final ablation was found to exceed the tumor size by 5 mm. Liver protection, anti-inflammatory, analgesic, and symptomatic treatment were prescribed after the MWA treatment.
Assessment of Therapeutic Efficacy and Follow-Up
One month after each session of TACE treatment or MWA, an abdominal dynamic contrast-enhanced MRI scan was performed to assess the therapeutic response and adverse effects (17). Patients with residual viable or recurrent tumors underwent further TACE or TACE plus MWA, whereas those with no evidence of viable tumors were followed up every 2 months. Serum alpha-fetoprotein (AFP) concentrations and MRI scans were evaluated as part of these follow-up visits. The tumor response was evaluated according to the modified Response Evaluation Criteria in Solid Tumors (1819). Local tumor control was assessed by the tumor control rate 6 months after treatment and time to tumor progression (TTP), defined as the interval from the date of commencing treatment to the date of identification of local progression. Overall survival (OS) was calculated from the date of commencing treatment to the date of either death or last follow-up. Complications were scored in the first treatment session, according to the Society of Interventional Radiology classification (20
21) i.e., those that necessitated major therapies, or resulted in prolongation of hospital stay, permanent adverse sequelae, or death were considered major complications. All other complications were considered to be minor.
Statistical Analysis
Statistical analysis was performed with a SPSS software package (version 18.0; SPSS Inc., Chicago, IL, USA). Quantitative data were compared by the Student's t test and categorical variables with the χ2 or Fisher test. Survival curves were calculated using the Kaplan-Meier method and compared using a log-rank test. A Cox proportional hazards regression model was used to analyze possible factors influencing tumor progression and OS. The statistical significance was defined as a p value of less than 0.05 (two-sided).
Go to :
RESULTS
Baseline Characteristics
This study included data on 258 patients, 92 of whom received 166 TACE + MWA treatments (median, 1.9; range, 1–4). A total of 166 patients in the TACE group received 676 TACE monotherapy treatments (median, 4.1; range, 1–13). The median follow-up time was 21.2 months (range, 4–45 months). The patients' baseline characteristics are presented in Table 1; there was no statistically significant difference between the two groups (p > 0.05).
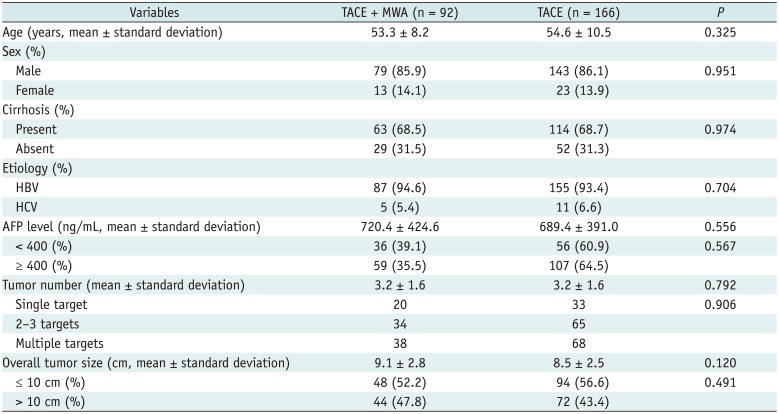
Table 1
Demographic and Baseline Characteristics of Two Treatment Cohorts
![]()
Local Tumor Control, Progression, and Associated Risk Factors
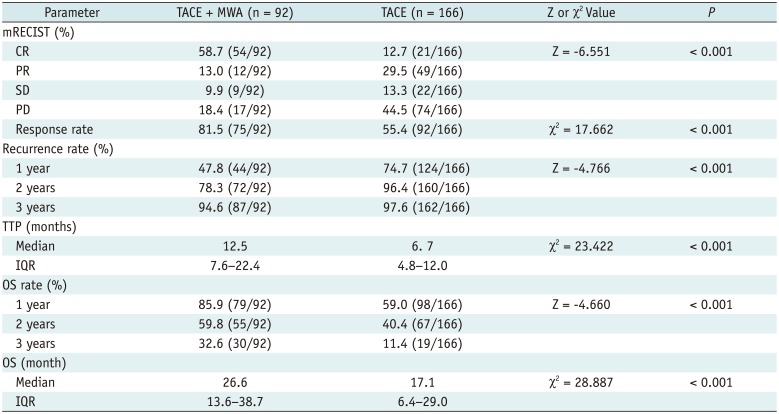
Rates of complete response (CR), partial response (PR), stable disease (SD) and progressive disease were 58.7% (54/92), 13.0% (12/92), 9.9% (9/92), and 18.4% (17/92), respectively, in the TACE + MWA group, versus 12.7% (21/166), 29.5% (49/166), 13.3% (22/166), and 44.5% (74/166), respectively, in the TACE group. The total response rate (CR + PR + SD) was 81.5% in the TACE + MWA group versus 55.4% in the TACE group (p < 0.001) (Table 2, Figs. 2, 3).
 | Fig. 257-year-old man with multinodular HCC who underwent TACE + MWA combination treatment.
A. Non-enhanced CT imaging revealed lipiodol deposits in multinodular HCC (arrowheads). B. CT image during MWA procedure showing antenna has reached opposite edge of tumor via its center (arrowheads). C. Contrast-enhanced MRI image (6 months post-ablation therapy) showing homogeneous hypointense non-enhancing areas (ablation beds, arrowheads) without residual enhancement, denoting successful ablation and complete response.
|
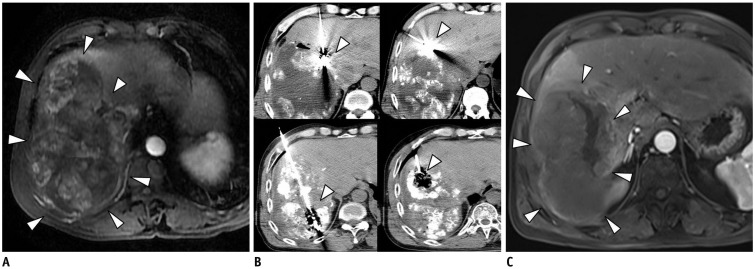 | Fig. 358-year-old man with HCC who underwent CT-guided MWA after TACE.
A. Diagnosis of HCC was based on findings on contrast-enhanced MRI and high AFP concentration (563 ng/mL). Lesion measures 13 cm in longest diameter (arrowheads). B. After TACE procedure, CT-guided MWA was performed to control residual tumor in target lesion (arrowheads). Patient underwent TACE + MWA combination therapy twice. C. Contrast-enhanced MRI scan 6 months after combination treatment showing non-enhancing thermal scar (arrowheads) at site of original tumor and no intrahepatic recurrence. AFP = alpha-fetoprotein
|
Table 2
Local Tumor Control and Survival of Two Treatment Cohorts
![]()
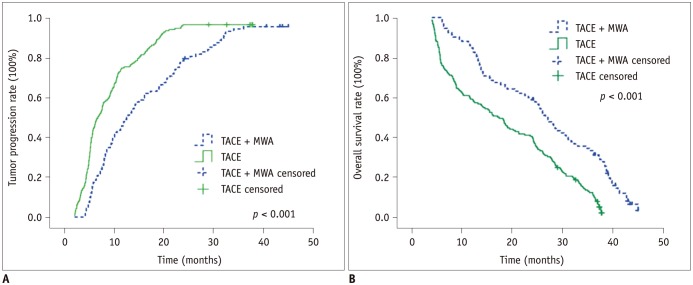
The median TTP was 12.5 months (inter quartile range [IQR], 7.6–22.4 months) in the TACE + MWA group versus 6.7 months (IQR, 4.8–12.0 months) in the TACE group. The cumulative 1-, 2-, and 3-year recurrence rates were 47.8, 78.3, and 94.6%, respectively, in the TACE + MWA group. These rates were significantly lower than the respective recurrence rates of 74.7, 96.4, and 97.6% in the TACE group (p < 0.001) (Table 2, Fig. 4A).
Univariate analysis revealed that an absence of cirrhosis (p = 0.081), three or fewer tumors (p = 0.001), overall tumor size ≤ 10 cm (p < 0.001), and TACE + MWA treatment (p < 0.001) could be correlated to an increase in TTP. Multivariate analysis by the Cox proportional hazard model revealed that three or fewer tumors (hazard ratio [HR] = 0.748, 95% confidence interval [CI]: 0.579–0.966, p = 0.026), tumor size ≤ 10 cm (HR = 0.410, 95% CI: 0.308–0.546, p < 0.001), and TACE + MWA treatment (HR = 0.349, 95% CI: 0.261–0.466, p < 0.001) were independently associated with an increased HR for TTP (Table 3).
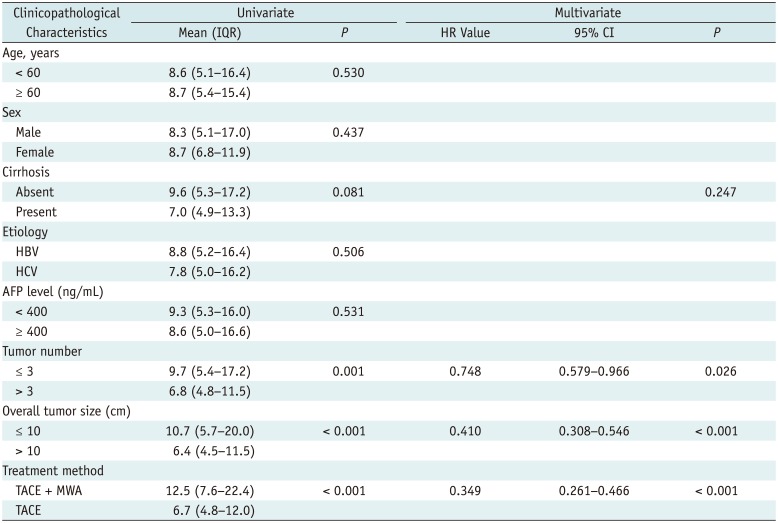
Table 3
Univariate and Multivariate Analyses of Prognostic Factors Associated with Tumor Progression
![]()
Overall Survival
The 1-, 2-, and 3-year OS rates were 85.9, 59.8, and 32.6%, respectively, in the TACE + MWA group. These percentages are significantly higher than the respective survival rates of 59.0, 40.4, and 11.4%, reported for the TACE group (p < 0.001). The median survival time was 26.6 months (IQR, 13.6–38.7 months) in the TACE + MWA versus 17.1 months (IQR, 6.4–29.0 months) in the TACE group (p < 0.001) (Table 2, Fig. 4B).
Overall survival could be correlated to cirrhosis (p = 0.074), number of tumors (p = 0.002), overall tumor size (p < 0.001), and TACE + MWA treatment (p < 0.001), as determined by univariate analysis. Multivariate analysis with the Cox proportional hazard model indicated that tumor number (HR = 0.694, 95% CI: 0.532–0.905, p = 0.007), overall tumor size (HR = 0.395, 95% CI: 0.295–0.527, p < 0.001), and TACE + MWA treatment (HR = 0.294, 95% CI: 0.214–0.405, p < 0.001) were independent factors for OS (Table 4).
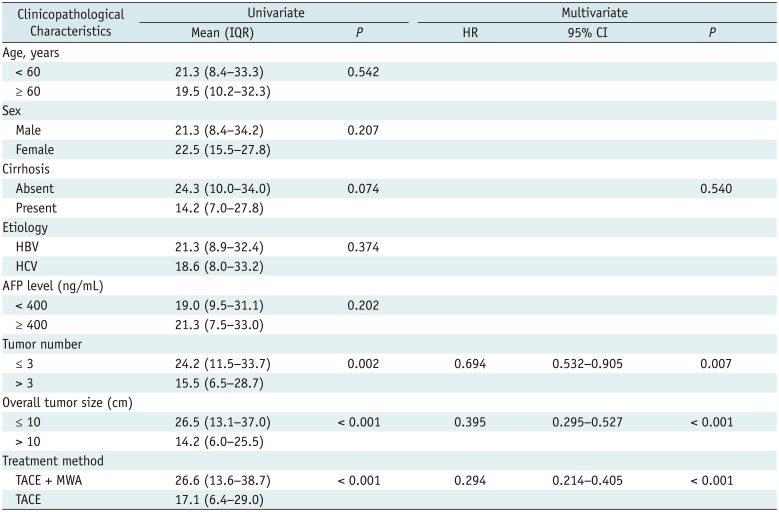
Table 4
Univariate and Multivariate Analyses of Prognostic Factors Associated with Overall Survival
![]()
Complications
There were no treatment-related deaths in either group. Major complications included liver abscess (n = 1) and subcapsular hematoma (n = 1) in the TACE + MWA group, and upper gastrointestinal bleeding (n = 2) and biloma with abscess (n = 4) in the TACE alone group. Minor complications in both groups included abdominal pain, fever, vomiting, grade 1–2 myelosuppression, and self-limiting pleural effusion. There were no significant differences between the two groups in terms of major and minor complications (p > 0.05) (Table 5).
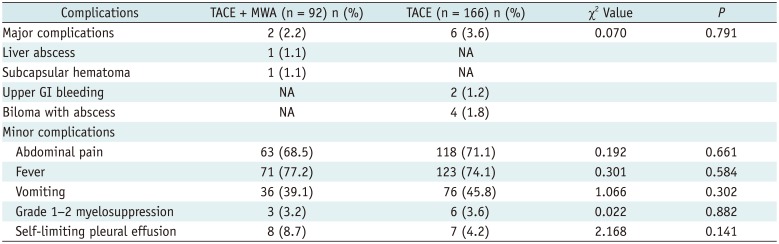
Table 5
Complications of Two Treatment Cohorts
![]()
Go to :
DISCUSSION
Although HCC is highly malignant, it usually remains undiagnosed until it progresses to multifocal or large intrahepatic lesions, at which point the patient is ineligible for surgical resection (1422). Thus, TACE is the standard treatment for large or multinodular HCCs (2324). However, after single or repeated TACE procedures, the tumor-supplying arteries may be occluded and snaking arterioles may have regenerated from the gastric, superior mesenteric, phrenic, and intercostal arteries, among other locations (2526), making it difficult to selectively catheterize tumor-feeding arteries to control residual tumor cells. Another reason for treatment failure is failure to completely occlude the tumor-supplying artery because of with the generation of small new collaterals to tumor remnants.
Better local tumor control and OS were achieved with TACE + MWA combination therapy versus TACE monotherapy in patients with Barcelona Clinic Liver Cancer (BCLC) stage A HCCs (2728). However, to the best of our knowledge, no studies have analyzed the clinical effectiveness and prognostic factors for survival after TACE and MWA combination therapy in patients with solitary large and multinodular HCCs. In the current study, we compared the treatment benefits of TACE + MWA and TACE alone in 258 patients with large or multiple tumors (not more than 10 tumors) and found that TACE + MWA achieved better tumor response rates, longer TTP and better OS rates in the study subjects. The superiority of TACE + MWA vs. TACE monotherapy may be attributable to: 1) Tumor emoblization caused by TACE embolization of tumor vessels by TACE that likely reduced the “cooling effect” of blood flowing through arteries feeding the tumor tumoral arterial blood flow (29); 2) TACE reduced or stabilized the size of large HCCs, facilitating MWA treatment; 3) TACE produced tumor tissue ischemia and inflammatory edema, thus increasing thermal effects of ablation (30); 4) Lipiodol was deposited in disseminating daughter lesions, facilitating their destruction in subsequent CT-guided MWA treatments; and 5) CT-guided MWA destroyed some hypovascular HCCs that were refractory to direct and precise TACE procedures (31). Our findings suggest that TACE + MWA combination therapy was associated with better objective outcomes and clinical benefits in patients with solitary large or multinodular HCCs, except for diffuse-type lesions.
We found that clinical outcomes such as TTP and OS in patients with a large solitary or multinodular HCCs were associated with tumor size, tumor number, and treatment method in patients with a large solitary or multinodular HCCs. TTP and OS were not significantly influenced by age, sex, AFP concentration, or accompanying cirrhosis. These results are consistent with findings from previous studies (32333435).
It is difficult to achieve complete necrosis of large HCCs with TACE or MWA (1136). Leung et al. (37) reported that size of the initial tumor size is a significant prognostic factor for local recurrence of liver malignancies treated by MWA. L et al. (38) studied treatment results in 923 patients with BCLC stage B HCCs. Liu et al. (39) reviewed treatment results in 312 patients with large solitary (> 5 cm) HCCs. They both reported that patients with HCCs ≤ 10 cm in size had significantly higher OS survival rates than those with larger HCCs. Kim et al. (40) found that select patients (with the sum of tumor number and maximum tumor size being no more than 11) benefited most from TACE among patients with BCLC stage B HCC. We found that the TTP and OS of patients with HCCs ≤ 10.0 cm in size were better than those of patients with larger HCCs. These findings were in agreement with similar previous studies and suggest that tumor size is independently associated with TTP and OS of patients with HCC and that patients with tumors of ≤ 10.0 cm in size should be prioritized for TACE and MWA combination treatments.
In this study, we found that patients with three or fewer tumors (with a maximum diameter > 3 cm) had better TTP and OS than those with more than three tumors. Peng et al. (41) reported that tumor number is a significant prognostic factor for recurrence-free survival and OS of patients with HCC treated by TACE + RFA. Higher mortalities due to tumor progression were reported by Yamakado et al. (42) for patients with intermediate-stage HCC and four or more tumors. The number of tumors reportedly predicts the degree of intrahepatic spread (4344). Our findings are consistent with these data in suggesting that the number of tumors is independently associated with TTP and OS of HCC patients; thus, TACE + MWA therapy should be recommended to patients with three or fewer tumors.
The present study has certain limitations. First, these data were obtained from a single tertiary-care center. A multicenter study with more patients is needed. Second, this was a retrospective study. A randomized controlled study is needed to confirm our findings. Third, 94% of our patients were positive for hepatitis B virus (HBV), which differs greatly from studies in Europe and the USA. Thus, a study including more HBV-negative patients with HCCs that is needed to comfirm our findings.
In conclusions, our findings indicate that combination therapy with TACE + MWA appears to be superior to TACE monotherapy in terms of delaying TTP and prolonging OS in patients with solitary large or multinodular (not more than 10 tumors) HCCs. Treatment method, tumor size, and number of tumors are significant prognostic factors for TTP and OS. Further randomized, multi-center, prospective studies are required to confirm the findings of this study in the future. Future randomized, controlled, multi-center, prospective studies are required to confirm our study results.
Go to :
 XML Download
XML Download