

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Insertion of self-expanding metallic stents has become an established method of palliative treatment to relieve malignant biliary obstructions (1234). The use of covered stents in the biliary system was initially developed to address the issue of tumor ingrowth. A variety of covering materials have been manufactured and tested to prevent tumor ingrowth and to avoid the need for re-intervention (56789101112131415). In last 12 years, polytetrafluoroethylene (PTFE)-covered stents have been demonstrated as an effective treatment method (9101112131415), with the PTFE material serving as an effective barrier to prevent tumor ingrowth.
Although PTFE-covered stents can prevent tumor ingrowth and are associated with relatively low rates of stent occlusion (9101112131415), stent dysfunction induced by the food impaction and the deposition of biliary sludge composed of cholesterol crystals, calcium bilirubinate and palmitate, cholesterol, bacteria and/or fungi, microbial byproducts, proteins, dietary fibers, and glycoproteins is a major cause of stent dysfunction, especially when stents are placed across the ampulla of Vater (15161718).
A prospective multicenter study of 160 patients, introduced the efficacy of the double stent system (15). While the results of that study were promising, further reduction of the incidence of sludge incrustation was warranted. As duodenobiliary reflux and subsequent biofilm formation in a stent lumen may be important in initiating sludge formation and subsequent stent occlusion (181920212223), there is a need for antireflux stents that prevent covered stent dysfunction resulting from duodenobiliary reflux.
With this goal, we modified an inner covered stent of the double stent system to reduce duodenobiliary reflux. Our hypothesis was that a long inner covered stent placed in the distal duodenum or proximal jejunum will reduce reflux into biliary system. The purpose of our study was to investigate the safety and efficacy of a double-stent system with long duodenal covered extension in patients with malignant extrahepatic biliary obstruction.
Go to : 
MATERIALS AND METHODS
Patients
This was a prospective single center study that enrolled 48 consecutive patients (31 men, 17 women; mean age, 61 years; range, 31–77 years) with malignant extrahepatic biliary obstructions from May 2013 to December 2015. The study was approved by the Institutional Review Board of our Institution and informed consent was obtained from each patient. Patients were included if they had an extrahepatic biliary obstruction caused by a malignancy that could not be treated surgically, due to unresectability, late tumor stage, advanced age, or a comorbid condition; if an endoscopic attempt to drain the obstructed bile ducts was unsuccessful; and if they had recurrent endoscopic stent dysfunction caused by food impaction. Exclusion criteria included abnormal coagulation status (international normalized ratio ≥ 1.5 and platelet count ≤ 50000/mm3), and poor general health status (Eastern Cooperative Oncology Group performance status grade 4).
Device
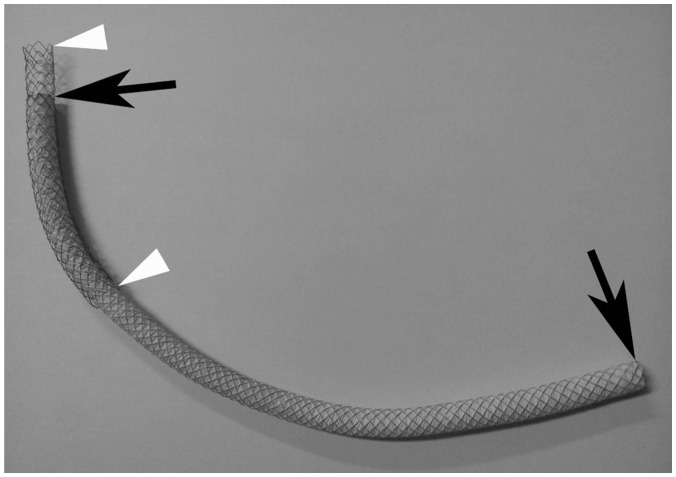
The double-stent system (GD Stent; TaeWoong Medical, Gimpo, Korea) (Fig. 1) is composed of two stents. The outer, self-expanding, uncovered stent (Niti-D stent) consisted of a double 0.007-inch-diameter nitinol wire in a tubular configuration, with an interlocking and diamond-shaped pattern. The outer uncovered stent was 10 mm in diameter and 8 cm in length. A 2-cm proximal uncovered metal extension was available for intrahepatic overstenting. The inner, conical-configured covered stent consisted of an outer expanded PTFE membrane and the inner supporting self-expanding uncovered stent (Niti-S stent) consisted of a single 0.006-inch-diameter nitinol wire. The proximal and distal diameters of the inner covered stent were 10 mm and 8 mm, respectively. The length of inner covered stent was 16 mm or 21 cm. Radiopaque gold markers were incorporated into the ends of both the inner and outer stents to increase stent visibility during placement under fluoroscopic guidance, and the two stents were knitted together by nylon sutures. The delivery system was a standard push-rod assembly consisting of a 9 Fr sheath and an inner catheter. Following deployment, these double stents shortened by 20%.
Technique
Prior to percutaneous transhepatic biliary drainage (PTBD), computed tomography (CT), magnetic resonance cholangiopancreatography or endoscopic retrograde cholangiopancreatography was performed to assess the anatomy and to plan the most appropriate approach for intervention. PTBD and stent insertion were performed under conscious sedation using intravenous pethidine hydrochloride (Demerol, Keukdong Pharmaceuticals, Seoul, Korea) and local anesthesia using 2% lidocaine (Jeil Pharmaceuticals, Daegu, Korea). Antibiotics were administered intravenously 2 hours before the procedure and for at least 48 hours afterwards. The intrahepatic bile duct was punctured using a 21-gauge Chiba needle (Cook, Bloomington, IN, USA) under the guidance of fluoroscopy or ultrasonography, and an 8.5 Fr drainage catheter (Cook) was inserted. Using cholangiography, we determined the location and length of the biliary stricture. The endoprosthesis was introduced over a 0.035-inch, 250-cm-long stiff hydrophilic guide wire (Terumo, Tokyo, Japan) or over an extra stiff Amplatz guide wire (Cook), and then deployed across the stricture to cover the bile duct approximately 2 cm proximal to the obstruction to prevent tumor overgrowth. In all patients, the distal portion of the stent was placed across the papilla to bridge the duodenum or jejunum (Fig. 2). Pre- and post-stenting balloon dilation was not performed in any patient.
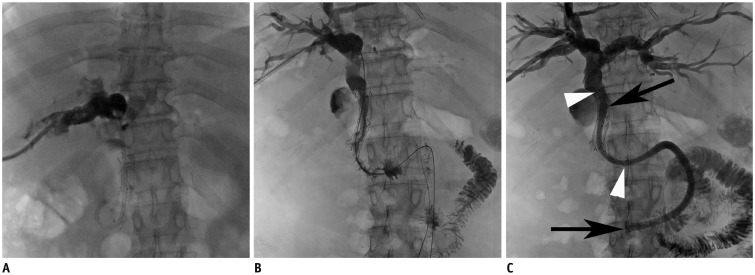
 | Fig. 253-year-old man with advanced gastric cancer.
A. Cholangiogram shows obstruction of common bile duct. B. Delivery system of double stents was placed via percutaneous route. Note inner covered stent (arrows) and outer uncovered stent (arrowheads). C. Cholangiogram after deployment of double stent (10 mm × 23 cm) shows adequate expansion of stent and fluent passage of contrast medium into jejunum. Malignant extrahepatic lesion was completely covered by inner covered stent (arrows). Note outer uncovered stent (arrowheads).
|
Prior to catheter removal, the biliary drainage catheter was clamped and left in place for 2–3 days to evaluate stent patency. During that time, patients ate a soft or normal diet. Correct position and function of the stent and food reflux were evaluated by follow-up cholangiography and bile aspiration performed through the catheter after clamp period. The catheter was subsequently removed if free contrast flow through the stent into the duodenum or the jejunum was documented and if serum bilirubin level was markedly decreased or normalized.
Follow-Up
All patients were evaluated clinically at the interventional radiology outpatient clinic, including measurements of their total serum bilirubin levels, 1, 6, and 12 months after their procedures, or if there were unexpected symptoms or signs such as jaundice, pain, or fever. The cutoff date for data analysis was December 31, 2016. Beginning 12 months after stent placement, all patients were interviewed by telephone monthly, until recurrence of obstructive jaundice or death, to evaluate overall stent patency and patient survival. Complications were diagnosed by clinical and laboratory examinations and, when necessary, by imaging modalities. Patients with recurrent jaundice were evaluated by CT or percutaneous transhepatic cholangiography. If stent occlusion was detected, the stent was revised percutaneously by inserting a biliary drainage catheter with/without balloon dilation or metallic stents.
Study Endpoints and Definitions
Major study endpoints were assessment of technical success, complications, successful internal drainage, patient survival, and stent patency. Technical success was defined as placement of the stent in an adequate position without migration. Complications were classified as major and minor according to the guidelines of the Society of Interventional Radiology Standards of Practice Committee (24). Successful internal drainage was defined as a decrease in serum bilirubin level to < 75% of the pretreatment value within the first month following stent placement. Patient survival was defined as the time interval between the initial stent placement and death or last follow-up. Stent patency was defined as the time interval between the initial stent placement and recurrence of the obstruction or death. Stent occlusion was defined as a radiologically confirmed biliary obstruction with serum bilirubin levels > 3 mm/dL, or as any condition requiring repeat intervention in order to improve the biliary drainage
Statistical Analyses
Paired-sample t test was used to compare the pre- and post-stenting serum bilirubin levels. Stent patency and patient survival rates were calculated according to the Kaplan-Meier method, and differences between curves were analyzed by the log-rank test. All statistical analyses were performed using of SPSS version 14.0 (SPSS Inc., Chicago, IL, USA), with p < 0.05 indicating statistical significance.
Go to :
RESULTS
Patient Characteristics
Baseline demographic and clinical data are presented in Table 1. A diagnosis of malignant extrahepatic biliary obstruction was confirmed in 21 (43.8%) patients by pathologic examination of endoscopic biopsy (n = 16), percutaneous biopsy (n = 3), and surgical biopsy (n = 2) specimens. In the remaining 27 (56.2%) patients, diagnosis was based on clinical and radiologic findings. Among 23 patients with malignant extrahepatic biliary obstruction caused by metastatic gastric cancer, 18 had undergone gastrectomy comprising total gastrectomy in (n = 6), subtotal gastrectomy (n = 3), and distal gastrectomy (n = 9).

Table 1
Patient Characteristics
![]()
Technical and Clinical Outcomes and Complications
The technical success rate of the double-stent placement was 100%. The radiopaque markers embedded in the device were visible fluoroscopically and allowed accurate stent placement in satisfactory positions without any complications. A single stent was sufficient to relieve malignant biliary obstruction in all 48 patients. Forty one patients received 10 mm × 23 cm stent and seven received the 10 mm × 18 cm stent. In the seven patients, the primary stenting technique consisted of direct placement of the double stent. In the remaining 41 patients with symptoms or signs of cholangitis, the stent was implanted 4–17 days (mean 5.3 days) after initial drainage (Fig. 3).
 | Fig. 364-year-old woman with pancreatic cancer. Patient had dysfunction of endoscopic metallic stent and subsequently inserted plastic stent.
A. Cholangiogram shows multifocal filling defects in bile duct and dysfunction of endoscopic metallic and plastic stent. B. After removal of plastic stent, bile duct and metallic stent were irrigated through drainage catheter. C. Cholangiogram after placement of double stents (10 mm × 23 cm) shows fluent passage of contrast medium through stent into jejunum. Note inner covered stent (arrows) and outer uncovered stent (arrowheads).
|
Procedure-related minor complication occurred in two patients. They experienced self-limiting hemobilia that completely resolved 1 and 2 days following stent placement and without transfusion. Procedure-related major complication occurred in one patient; acute pancreatitis occurred immediately after stent placement in one patient and was successfully treated by conservative management over 4 days. Late complication in two patients was acute cholecystitis at 131 and 135 days. Both cases were successfully treated by transhepatic gallbladder drainage. Acute cholecystitis was associated with tumor invasion of the cystic duct orifice in these two patients with advanced gastric cancer. Duodenal or jejunal complications related to the dual stent system were not observed during the follow-up period. Therefore, the overall complication rate was 10.4% (five of 48 patients).
Follow-up cholangiography after clamp test period (mean, 2.7 days; range, 2–3 days) showed patent stent in 43 (89.6%) patients and immediate stent dysfunction due to food reflux in three (6.3%). In the remaining two patients, follow-up cholangiography and subsequent removal of their drainage catheters could not be performed due to their early death. The two patients died 6 and 9 days after stent placement due to rapidly progressing underlying malignancy. Among the 43 patients with patent stent, 42 were free of external drainage catheter after follow-up cholangiography. In the remaining one patient with a patent stent, the drainage catheter could not be removed due to progressive increase in serum bilirubin level. Three patients experienced food reflux with stent dysfunction. Their drainage catheters could not be removed due to recurrent food reflux despite frequent irrigation of the bile duct and stent. Successful internal drainage was achieved in 42 (87.5%) of 48 patients. The mean serum bilirubin level which was 8.6 ± 6.6 mg/dL before drainage and decreased significantly to 2.6 ± 3.2 mg/dL one month after biliary stent insertion (p < 0.001).
Patient Survival
Clinical follow-up until death or the end of the study was available for all patients and lasted 9–448 days (mean, 105 days). Following stent placement, 47 (97.9%) of 48 patients died, whereas one (2.1%) remained alive. According to the Kaplan-Meier survival analysis, the median survival time was 92 days (95% confidence interval [CI], 61–123 days) (Fig. 4).

Stent Patency
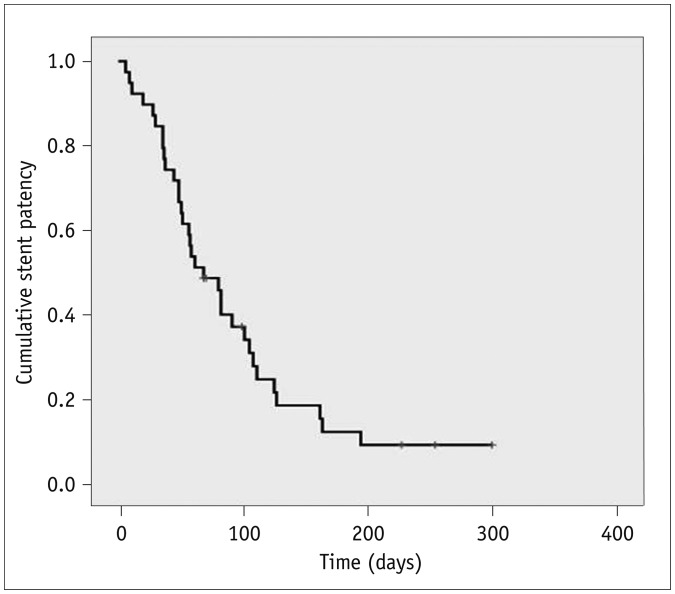
Kaplan-Meier analysis revealed a median stent patency time of 83 days (95% CI, 46–120 days) (Fig. 5). Stent occlusion was observed in ten (23.8%) of 42 patients after a mean interval of 130 days (range, 21–400 days). Among the ten patients, six had only jaundice and two had jaundice with cholangitis. The mean serum bilirubin level was 3.7 ± 2.3 mg/dL (range, 2.2–8.3 mg/dL). In the remaining two patients, stent dysfunction was suspected on follow-up CT. The ten patients were treated with PTBD. Stent occlusion was caused by food impaction with or without subsequent biliary sludge in all ten. Food materials and sludge were confined to duodenal extension in seven patients, and food materials and sludge were found in the bile duct as well as duodenal extension in three. None of these patients was managed by insertion of an additional stent due to firmly occluded duodenal extension by food materials and sludge (n = 2) and rapidly progressing disease with poor general condition (n = 8). Log-rank analysis revealed a higher incidence of stent occlusion in metastatic gastric cancer patients with pervious gastrectomy, but was not statistically significant (p = 0.069). Tumor ingrowth was not noted in any patient. Therefore, overall stent occlusion after stent placement occurred in 13 (33.3%) of 39 patients.
Go to :
DISCUSSION
Previous studies reported that duodenobiliary reflux is a major cause of cholangitis and plays an important role in stent dysfunction (181920212223). In these studies, patients with biliary metallic stents had episodes of unexplained fever or cholangitis, as seen from 6.5% to 22% and metallic stent placement across the main papilla may predispose patients to cholangitis because of disruption of the sphincter mechanism. A previous study using barium examination revealed free barium refluxes through the transpapillary biliary metallic stents in all patients (25). Moreover, the dietary fibers accelerate bacterial attachment, increase the amount of bile sludge formation, and potentially decrease the long-term patency rate of these stents (161718). A previous study that used confocal laser scanning and scanning electron microscopy described that networks of large dietary fibers covered with microorganisms resulting from duodenal reflux were a major contributing factor in stent occlusion (18). A recent prospective, randomized study in 77 patients with unresectable distal malignant biliary obstruction at a single center using covered stent system with antireflux valve and conventional covered stent reported that significantly longer stent patency rates in the antireflux stent group than in the conventional covered stent group (23). However, this stent system did not completely prevent duodenobiliary reflux on barium meal examination after stent placement. Therefore, a newly designed approach was needed to target the influence of duodenobiliary reflux on stent patency rates.
The present prospective study assessed the PTFE-covered stent system with long duodenal covered extension. The original design of the covered stent system was intended to treat malignant extrahepatic biliary obstruction (1415). We modified an inner covered stent to reduce the incidence of stent dysfunction caused by duodenobiliary reflux. In the present study, stent deployment was technically successful in all patients, and correct positioning was verified after all placements. There was no additional difficulty in placing this stent system compared with the conventional metallic stents. The introducer system was 9 Fr in diameter, which is acceptable size because the PTBD catheters used in our institution are of a similar size (8.5 Fr). The complication rate (10.4%) and successful internal drainage rate (87.5%) agreed with the results of previous studies using PTFE-covered stents (891011121314). Duodenal or jejunal complications related to the dual stent system were not observed during the follow-up period.
Stent occlusion occurred in 10 (23.8%) of 42 patients. The cause of stent occlusion was food impaction with/without biliary sludge. In prior studies using PTFE-covered stents, the stent occlusion rates ranged from 9–19% (9101112131415). It is difficult to compare our results with the prior findings. However, the stent occlusion rate we observed was similar to those in studies using PTFE-covered stents. Prior to the present study, we anticipated that a long inner PTFE-covered stent placed in the distal duodenum or proximal jejunum would reduce food reflux into biliary system and improve internal bile drainage. Moreover, the inner covered stent has no side holes, thereby avoiding reflux of duodenal contents into the inner stent, bypassing the distal end. However, this stent system did not completely prevent stent occlusion caused by food reflux. Among ten patients who had stent occlusion, food materials and sludge were confined to duodenal extension in seven patients and food materials and sludge were found in the bile duct as well as duodenal extension in three patients. The long duodenal extension could contribute to food stasis in the stent lumen. In addition, although the incidence of stent occlusion did not reach statistical significance, there was a higher tendency of stent occlusion due to food reflux in metastatic gastric cancer patients with previous gastrectomy. The altered peristaltic movement after gastric operation also could contribute to food reflux and subsequent stent occlusion. Presently, however, we did not observe stent occlusion resulting from tumor ingrowth or stent migration. It is also difficult to compare relatively shorter median patient survival and stent patency time of this study with results of previous studies, as most of the study patients had late stage of disease.
The present study has several limitations. First, this stent system is not yet commercially available outside of Korea. Second, median survival was only 92 days, which limited the ability to observe stent patency over a longer period of time. The relatively short life expectancy is likely related to the severity of the patients' underlying disease. Finally, because this study had no control group, further comparative studies with other existing covered stent may be needed.
In conclusion, percutaneous placement of a covered stent system with long duodenal extension is feasible and safe. However, this stent system may not completely prevent stent occlusion caused by food reflux.
Go to :
 XML Download
XML Download