

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Radioembolization, an increasingly used treatment option for primary and metastatic liver cancers, involves intra-arterial delivery of microspheres containing yttrium-90 (90Y), a high-energy pure beta-emitter (12). Technical similarity to chemoembolization may be deduced based on the term of “radioembolization”; however, this term is a misnomer given that radioembolization has little embolic effect (1). More specifically, chemoembolization exerts ischemic effects due to embolization and cytotoxic effects due to the use of chemotherapeutic drugs, whereas radioembolization works mainly via local radiation and needs blood flow to achieve optimal radiation effects (34).
As a form of brachytherapy, radioembolization can cause radiation-related changes in the adjacent structures around the target lesion (56). Moreover, the delivery of radioactive microspheres to non-target organs can cause complications such as cholecystitis and gastrointestinal ulceration (56). Familiarity with the imaging features of various post-treatment benign changes and potential pitfalls is important to avoid misinterpretation of these findings as tumor progression or other diseases.
In this review, we discuss the interpretation of imaging features following 90Y radioembolization for liver malignancies including tumor response assessment, post-treatment benign changes, and potential complications. In addition, general strategies for pre-treatment evaluation and treatment procedures are presented to promote understanding of radioembolization.
Pre-Treatment Evaluation of Radioembolization
General Principles
During the selection of patients for radioembolization, a multidisciplinary approach involving experts who have expertise in radiology, nuclear medicine, hepatology, radiation, medical, and surgical oncology is needed to select the optimal candidates (7). Patients should complete comprehensive evaluation of tumor burden, hepatic reserve, and performance status. Unresectable liver-only or liver-dominant primary or metastatic liver malignancies are considered good candidates for radioembolization (7), and intrahepatic tumor burden ≤ 70% of the liver volume is generally considered to be acceptable (8). With respect to liver function, total bilirubin < 2.0 mg/dL and Child-Pugh class A-B7 would be required to tolerate the treatment (910). In addition, life expectancy ≥ 12 weeks and European Cooperative Oncology Group status 0–2 would be acceptable for radioembolization (7). In Korea, since 90Y microspheres are not reimbursed by the national health insurance, patients' economic status and their private health insurance are also important factors that determine the treatment options.
Screening Test: Hepatic Angiography and 99mTc-MAA Scan
Patients who are selected as candidates for radioembolization of liver tumors should undergo pretreatment simulation tests consisting of hepatic angiography and technetium-99m macroaggregated albumin (99mTc-MAA) scan (6).
On preparatory angiography, the anatomy of the hepatic artery and the presence of non-hepatic arteries originating from the hepatic artery are investigated. Recently, C-arm cone-beam computed tomography has become an essential tool for angiographic evaluation that is particularly useful to visualize small arteries (11). Angiographic information is critical because if radioactive microspheres are infused into the non-hepatic arteries during radioembolization procedures, serious complications such as gastrointestinal ulcers can occur (6). Thus, prophylactic embolization of non-target branch vessels, including an accessory left gastric artery, right gastric artery, hepatic falciform artery, and esophageal branches from the replaced left hepatic artery, can be performed, although there are controversies about the indications (91213).
Technetium-99m macroaggregated albumin scans aim to estimate extrahepatic deposition and lung shunting by simulating the microsphere biodistribution of 90Y (14). Immediately after 99mTc-MAA is injected into the hepatic artery in the angiography suite, patients are transferred to gamma camera for a lung shunt scan with or without single photon emission computed tomography (SPECT)/CT. Although SPECT/CT is not essential in dosimetry, it can provide more reliable assessment of 99mTc-MAA distribution on fusion images (Fig. 1), which may be useful to predict tumor response, to detect unexpected perfusion outside of the liver, and to elaborate dosimetry of the partition model (15). If radioactivity is detected in the non-target organs on 99mTc-MAA scan, prophylactic embolization can be performed or catheter position can be modified at the time of the procedure to avoid severe complications (13). Lung shunting is one of the major concerns of radioembolization because radiation pneumonitis can develop in case of an excessive intratumoral arteriovenous shunt (16). For the two commercially available 90Y products including TheraSphereé glass microspheres (BTG, London, UK) and SIR-Spheresé resin microspheres (Sirtex Medical, North Sydney, Australia), lung dose of 30 Gy for a single treatment and 50 Gy as a cumulative dose for TheraSphereé (6), and 20% lung shunting for SIR-Spheresé are the recommended upper limits (17).
If a patient is determined to be eligible to receive radioembolization, intra-arterial delivery of radioactive microspheres is commonly performed 1 or 2 weeks after the screening tests (1).
Treatment Methods
The procedure techniques of radioembolization are quite similar to those of chemoembolization, since both techniques require selective catheterization of the hepatic artery and involve transarterial delivery of therapeutic particles. However, radioembolization is usually performed in a less selective fashion compared to chemoembolization. In patients with localized disease, radioactive microspheres are administered via a segmental or lobar hepatic artery according to the tumor extent and liver function (18). In patients with multiple hepatocellular carcinomas (HCCs) or metastases of bilobar involvement, radioactive microspheres are usually infused at the lobar artery level with sequential split treatment (i.e., treating one lobe in the 1st session and then the other lobe in the 2nd session with a 4–6 week interval) to reduce treatment-related complications (18).
Radiation segmentectomy refers to radioembolization involving 2 or fewer hepatic segments by injection of radioactive microspheres at a high ablative dose into segmental hepatic arteries, which may result in complete necrosis of the tumor as well as non-tumorous hepatic parenchyma of a treated segment (1920). A segment treated by radiation segmentectomy gradually shrinks and it often looks like a surgical segmentectomy on follow-up imaging (21).
Radiation lobectomy represents injection of radioactive microspheres at a regular dose into a lobar artery to induce contralateral lobe hypertrophy (2223). This can be used as a bridge to liver resection in patients who initially have a small future liver remnant volume. Until now, portal vein embolization has been widely used as a standard technique for this purpose. Compared to portal vein embolization, radioembolization provides the potential benefit of offering concomitant control of liver tumors during the waiting time (23).
Immediate Post-Treament 90Y PET Imaging
Although 90Y is a pure beta-emitter, it emits very small amount of positron (0.003%) and, therefore, can be imaged by sensitive positron emission tomography (PET) scanners (24). Immediately after radioembolization, 90Y PET can demonstrate the actual distribution of radioactive microspheres (Fig. 2), and the absorbed radiation dose to each part of the lesion can be estimated (25). Therefore, 90Y PET imaging including PET/CT and PET/MR imaging may be useful in the prediction of tumor response as well as in the interpretation of follow-up imaging (2627).
Tumor Response Assessment for Radioembolization
Size- and Tumor Viability-Based Imaging Criteria
Effective radioembolization would finally induce reduction in the size of the tumor, and this size-based response can be useful in the prediction of survival outcomes (2829). However, the decrease in size after radioembolization occurs slowly, with a reported median time to response of 4–6 months according to the WHO criteria for responding patients with HCC (3031). On the other hand, tumor viability-based imaging criteria such as modified response evaluation criteria in solid tumor and European Association for the Study of Liver (EASL) criteria may enable earlier and more sensitive detection of tumor response to radioembolization than size-based criteria (3132), and can be useful in the prediction of pathologic complete response (33). Moreover, responders identified based on tumor viability-based imaging criteria have been reported to show favorable overall survival after radioembolization of liver tumors (303435).
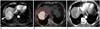
While an increase in tumor size is usually regarded as a finding suggestive of tumor progression, a paradoxical increase in tumor size at an early follow-up after radioembolization should be interpreted with caution because it can be caused by intra-tumoral hemorrhage, edema, and necrosis (Fig. 3) (3637). In addition, tumor growth increment during the time interval from pre-treatment imaging to the administration of 90Y can also cause size discrepancy between pre- and post-treatment imaging. Usually, it takes 3–4 weeks from the initial imaging study to radioembolization, because there are multiple required steps before treatment, including simulation test, hospital admission, and delivery of radioactive microspheres from the manufacturing facility.
On an early follow-up, persistent tumoral enhancement or residual enhancing areas are common imaging features (Fig. 4), and they do not have a predictive value for viable tumor (37). While a decrease in the degree of tumor enhancement is a finding suggestive of effective treatment, this change usually takes several months after radioembolization (38). Reactive edema and granulation tissue formation after treatment may result in enhancement without a viable tumor (36). A recent study showed that pathologic complete response was not infrequent in cases that show a partial response according to EASL criteria (33). Therefore, differentiation of a non-responding viable tumor from the well-responding portion is often challenging on contrast-enhanced imaging. Although the clinical indication for an additional intervention has not been well established (39), if the enhancing part increases on a serial follow-up, it is generally regarded as a viable tumor requiring additional therapy (Fig. 5). On the contrary, if the enhancing part does not show interval increase paralleled by a stable or decrease in serum tumor marker levels, it can be observed without further treatment.
Diffusion-Weighted MR Imaging
Diffusion-weighted MR imaging (DWI), which reflects tissue cellularity and integrity of the cell membrane, can provide functional information about the tumor (40). As alterations in DWI-derived parameters can precede the morphologic changes in the tumor after treatment, they can be useful in the early prediction of tumor response speeding up the “go or no-go” decision making process (40).
In the monitoring of tumor response after radioembolization, tumor necrosis after effective treatment corresponds to an increase in the apparent diffusion coefficient (ADC) value of the tumor (Fig. 6) (41). For liver tumors treated with radioembolization, there have been several reports showing that greater increase in tumor ADC on early follow-up may be a favorable predictor for the later tumor response and survival outcome (4243). In addition, both cellular swelling immediately after treatment and increased cellularity due to tumor progression can cause reduction in the ADC value (4144), interpretation of tumor ADC should be performed with caution according to the follow-up interval after treatment.
Intravoxel incoherent motion (IVIM)-DWI, which is based on the concept of bi-exponential signal decay as a function of b values, is receiving increasing attention as a quantitative tool for assessing tumor response (444546). As IVIM-DWI can estimate microcirculation and molecular diffusion separately, it might be useful in the evaluation of changes in tissue perfusion, cellularity, and necrosis after anti-cancer treatment (45). Recent studies have shown the potential usefulness of perfusion-related parameters derived from IVIM-DWI as early predictors of prognosis in patients with hepatic metastases after radioembolization (4748).
Tumor Marker
The levels of serum tumor markers (e.g., alpha-fetoprotein in HCC, carcinoembryonic antigen in colorectal liver metastases, and carbohydrate antigen 19–9 in intrahepatic cholangiocarcinoma) generally decrease after radioembolization (294950). Response classification based on the tumor markers may correlate with future imaging response and survival outcomes (4951). However, the time-dependent change in a tumor marker does not always correspond to the imaging response (52). The response of tumor markers usually precedes the response of imaging, and combined interpretation of a tumor marker and imaging during follow-up after radioembolization may provide more accurate information about the need for additional treatment. As discussed earlier in this article, when interpreting persistent enhancement on an early follow-up, responders and non-responders for tumor markers may have different probabilities for the presence of a pathologically viable tumor.
Benign Post-Treatment Imaging Findings
Radiation Effect on Non-Tumorous Hepatic Parenchyma
While microspheres are preferentially deposited in hepatic tumors (53), non-tumorous hepatic parenchyma around the tumor and in the vascular territory of the treated segment is exposed to irradiation, and thus, may present radiation-induced changes. This finding usually appears without significant clinical manifestations or alteration in liver function tests (52).
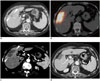
Imaging features of radiation effect on hepatic parenchyma after radioembolization have not yet been well described. However, radiation-induced changes in the liver after external radiation have been reported in the previous studies (545556) and can be applied in the interpretation of post-radioembolization examinations with caution. After external radiation therapy, the irradiated hepatic parenchyma frequently shows arterial hyper-enhancement on an early follow-up until 6 months which may interfere with accurate assessment of tumor response in HCC (54). Lack of washout appearance on the delayed phase can be helpful in differentiating radiation effect from tumor progression (54). On the portal venous phase and delayed phase images, the irradiated hepatic parenchyma can present various enhancement patterns according to the radiation dose and time interval after the treatment (55). Typical time-dependent changes are as follows: type I (within 3 months), hypo-attenuation on the portal venous phase and iso-attenuation on the delayed phase (Fig. 7B); type II (3–6 months), hypo-attenuation on the portal venous phase and hyper-attenuation on the delayed phase (Fig. 7C) ; type III (after 6 months), iso- or hyper-attenuation on the portal venous phase and hyper-attenuation on the delayed phase (Fig. 8C) (55). Type I and II enhancement patterns may be explained by the radiation-induced acute veno-occlusive disease, resulting in delayed contrast inflow without and with reduced contrast clearance (56). Type III enhancement patterns may be related to distortion of the liver architecture and fibrotic change (55). By reflecting the time-dependent changes, serial imaging studies may show a shift in the enhancement patterns. In addition, the volume of hepatic parenchyma showing a radiation effect is usually decreased on an additional follow-up (56) (Figs. 7, 8).
Gadoxetic acid-enhanced MRI can provide functional information about hepatocyte uptake and, therefore, it may be useful in the detection and evaluation of the extent of radiation effect in the hepatic parenchyma. The irradiated hepatic parenchyma may show decreased signal intensity on hepatobiliary phase imaging of gadoxetic acid-enhanced MRI (Fig. 9). Value of hepatobiliary phase imaging following radioembolization should be further validated in terms of correlation with clinical manifestations and prognosis.
Radiation Necrosis of the Hepatic Parenchyma
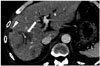
During radiation segmentectomy, excessive high dose radiation is selectively delivered into the focal area of the liver, and it may lead to necrosis, not only in the tumor but also in the hepatic parenchyma of the treated segment (Fig. 3) (52). Radiologically, hepatic parenchyma showing radiation necrosis shows poor or no enhancement, and shrinks with passage of time. Focal radiation necrosis should not be misdiagnosed as a new hypovascular tumor or progression of the previous disease. By showing the distribution of radioactive microspheres, 90Y PET following radioembolization can help in the differential diagnosis. If the matched area shows high activity on 90Y PET, radiation necrosis should be considered as a differential diagnosis for the new hypovascular lesion (Fig. 10).
Peritumoral Ring Enhancement
After loco-regional treatment of hepatic tumors, nodular or peripheral ring-like enhancement around the treated lesion is usually considered to indicate local recurrence or a residual viable tumor (57). However, this may not be true following radioembolization. Peritumoral ring enhancement is frequently seen after radioembolization and it may persist for several months (Fig. 8) (3133). This finding is suggestive of a pathologic complete response with a high positive predictive value rather than the presence of a residual viable tumor (33). Pathologically, this imaging finding would correspond to granulation tissue related to the inflammatory treatment response and/or a fibrous pseudocapsule surrounding the tumor (58). Thus, this imaging finding should not be misinterpreted as local recurrence or a residual viable tumor. While peritumoral ring enhancement commonly shows circumferential enhancement with even thickness without wash-out on the portal venous and delayed phases, a marginal recurrent tumor shows nodular enhancement with wash-out.
Perivascular Edema
Transient perivascular edema is often seen 3–6 months after radioembolization, probably due to the deposition of microspheres in the peritumoral vascular plexus (51). It manifests as low-attenuating lesions with perivascular distribution on contrast-enhanced imaging studies (Fig. 11). Without knowledge of this transient phenomenon, it can be mistaken for an infiltrative tumor, which leads to an incorrect diagnosis of tumor progression, or for a hepatic attenuation change arising from a vascular problem (52). When low-attenuating lesions with perivascular distribution occur, and if the serum tumor marker level decreases without progression of the primary tumor, perivascular edema can be diagnosed easily.
Contralateral Lobe Hypertrophy
Radioembolization induces contralateral lobe hypertrophy of the untreated lobe and concomitant atrophy of the ipsilateral hepatic lobe (Fig. 7), which may be explained by the radiation effect and alteration in portal venous flow (5). The degree of hypertrophy of the contralateral lobe has been reported to be greater after radioembolization than after chemoembolization, and therefore, radioembolization may have an advantage as a bridge to liver resection (222359). Moreover, during the time to contralateral lobe hypertrophy, radioembolization has the potential to attain local tumor control (23).
Changes in the Gallbladder Wall
Gallbladder wall edema, mural hyper-enhancement, and mural rent (Fig. 1C) are common benign findings after radioembolization and they usually do not have any clinical consequences (660). These changes may be due to the aberrant embedment of radioactive microspheres in the gallbladder wall through the cystic artery or small perforator arteries (52). The diagnosis of radiation cholecystitis should be made prudently even in cases of radiologic abnormality of the gallbladder, which will be described further in detail.
Perihepatic Fluid Collection and Pleural Effusion
Adjacent structures such as pleura and liver capsule may also be exposed to radiation, resulting in a small amount of perihepatic ascites (Fig. 5B) and pleural effusion, particularly in cases of tumors adjacent to the Glisson's capsule or the right pleura (51). They are regarded as transient reactive changes, and do not require any specific treatment. The appearance of perihepatic ascites and pleural effusion on follow-up imaging without any clinical symptoms or laboratory abnormality should not be misinterpreted as radioembolization-induced liver disease (REILD), indicating hepatic toxicity after radioembolization (5).
Dystrophic Calcification
Intratumoral dystrophic calcification can develop after radioembolization, probably secondary to tumor necrosis or degenerative changes (61). Dystrophic calcification can be easily identified as a high attenuated lesion within the tumor on CT images (Fig. 10D). This finding is occasionally encountered in colorectal liver metastases after chemotherapy and/or radiation therapy (6162). However, little is known about the predictive value of intratumoral dystrophic calcification after radioembolization with respect to pathologic tumor response or survival outcomes.
Complications
REILD
Radioembolization-induced liver disease may develop in 0–4% of cases after radioembolization due to exposure of the hepatic parenchyma to a high dose of radiation (6). As the embolic effect of radioembolization is minimal, ischemic change due to embolization would not significantly contribute to liver damage (63). Contributing risk factors include underlying liver cirrhosis and previous or subsequent exposure to systemic chemotherapy (64). REILD may manifest with a wide spectrum of clinical manifestations, including abdominal pain, jaundice, and ascites, and laboratory abnormalities, including hyperbilirubinemia, elevated alkaline phosphatase, and gamma-glutamyl transpeptidase (6). Most patients can be treated conservatively, but some cases may progress to hepatic failure (6566). Therefore, for the determination of treatment protocols, both treatment efficacy and potential liver toxicity should be considered. Radiologic findings of REILD include liver parenchymal edema and hepatomegaly, which are quite nonspecific (5). In clinical practice, if a post-treatment patient shows clinical and laboratory abnormalities suggestive of liver dysfunction and does not have any evidence of disease progression or biliary obstruction on imaging studies, REILD should be highly suspected.
Radiation Pneumonitis
If excessive radioactive microspheres flow into the pulmonary artery through tumor-induced arteriovenous shunting in the liver, the lung parenchyma would be irradiated and radiation pneumonitis may develop (67). The incidence of radiation pneumonitis is less than 1% in cases where standard dosimetry is used (6). To avoid the risk of radiation pneumonitis, a pretreatment 99mTc-MAA scan is routinely performed to measure the lung shunt fraction, which is used in patient selection (16). If radiation pneumonitis develops, patients will present with non-productive cough, dyspnea, and fever (67). Typical CT imaging features include ill-defined, patchy opacities, and ground glass opacities in a symmetric pattern with relative sparing of the peripheral and hilar portions, resulting in “bat-wing” appearance (67). These imaging findings of the acute stage may resolve after corticosteroid treatment. If radiation pneumonitis progresses to radiation fibrosis, linear scarring, volume loss, traction bronchiectasis, and honeycombing appearance can be observed in the chronic stage (51).
Radiation Cholecystitis
Radiation cholecystitis can develop due to non-target administration of radioactive microspheres into the cystic artery and it may require cholecystectomy or percutaneous cholecystostomy (68). The reported incidence of radiation cholecystitis requiring surgery is 0–2.4% (60). This complication should be suspected in patients presenting with right upper quadrant pain, fever, and nausea occurring shortly after radioembolization, and gallbladder wall thickening and/or pericholecystic fluid collection seen on imaging studies (69). However, as mentioned earlier, gallbladder abnormalities are frequently detected on post-radioembolization follow-up imaging in patients without any symptoms (60). Indeed, clinically significant radiation cholecystitis is rare and conservative treatment is the initial management, although some refractory cases require surgery (70).
For preventing radiation cholecystitis, microspheres should be administered into the hepatic artery distal to the cystic artery whenever feasible (68). Prophylactic embolization of the cystic artery can be performed, although there are controversies about the benefit considering the low incidence of clinically significant radiation cholecystitis and increased risk of ischemic cholecystitis due to cystic artery occlusion (71). In addition, temporary occlusion of the cystic artery using a detachable coil can be attempted as it reduces microsphere uptake in the gallbladder during the radioembolization procedure and minimizes the risk of ischemic cholecystitis by removal of the coil after the procedure (72).
Gastrointestinal Ulceration
Non-target administration of radioactive microspheres into the microvasculature of the gastrointestinal tract may cause gastrointestinal ulceration (73). The incidence of gastric ulcer has been reported to range from 0.1% to 3.1% (74). This is the main rationale for prophylactic embolization of aberrant vasculatures during pretreatment hepatic angiography. Deposition of radioactive microspheres in the gastric or duodenal wall leads to direct radiation toxicity as well as chronic ischemic changes due to microvascular injury (7576). Gastrointestinal ulcer caused by 90Y can present several months after treatment and can be accompanied by severe abdominal pain (77). As it seldom heals with medical treatment, surgical resection of the affected gut should be considered (73). A high index of suspicion is needed to make the diagnosis of radioembolization-associated gastrointestinal ulceration as the clinical, endoscopic, and imaging features are nonspecific.
CONCLUSION
Radioembolization using 90Y is being actively investigated as an effective and safe treatment option for various kinds of hepatic malignancies. As it works by delivering intense radiation to liver tumors with little embolic effect, it results in unique post-treatment imaging findings different from those following chemotherapy or chemoembolization. For tumor response assessment after radioembolization, imaging changes in size, enhancing tumor burden, and diffusion restriction as well as serum tumor markers can be useful, and a combination may improve the diagnostic accuracy. Common post-treatment benign changes such as peritumoral ring enhancement and perivascular edema should not be interpreted as tumor progression. Radioembolization can cause several complications due to the radiation effect in the surrounding structures or aberrant deposition of microspheres in the non-target organs such as gallbladder, gastrointestinal tract, and lungs. Management decisions about imaging-detected complications should be made based on the correlation of clinical symptoms and laboratory findings.








 XML Download
XML Download