

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Prostate Imaging-Reporting and Data System Version 2 (PI-RADSv2) is a language of prostate magnetic resonance imaging (MRI) for communicating the probability of clinically significant prostate cancer (csPCa). PI-RADSv2 scoring uses a 5-point Likert scale to assess csPCa, and study data have suggested that a score of 4 or greater indicates a high probability of csPCa (12). The pooled sensitivity and specificity were 85−89% and 71−73%, respectively (23).
In terms of estimating the likelihood of PCa, PI-RADSv2 scores are somewhat similar to prostate-specific antigen (PSA). The probability of PCa increases as the serum PSA level increases (e.g., < 4; 4−10; and ≥ 10) (4). Likewise, in recent studies, the detection rates of PCa increased sequentially according to PI-RADSv2 scores (56). This situation indicates that PI-RADSv2 may provide guidelines with respect to further investigations such as biopsy, like PSA.
Prostatic lesions showing higher PI-RADSv2 scores are more likely to be proven as csPCa by targeted biopsy (7). Meanwhile, for the lesions with scores less than 3, an additional targeted biopsy may not be necessary because of low cancer detection rate (8). Also, the application of PI-RADSv2 may reduce the total number of biopsy cores. A previous study demonstrated comparable diagnostic performance between two-core targeted biopsy using PI-RADSv1 from prebiopsy MRI and 12-core systematic biopsy in detecting csPCa (9). For biopsy-proven low-grade PCa, PI-RADSv2 from postbiopsy MRI may aid in reducing the risk of underestimation by predicting the risk of Gleason score (GS) upgrading (10). This would aid in the decision regarding optimal management.
In PI-RADSv2, the lesions with higher scores, suggestive of csPCa, are likely to be apparently visible and/or large on multiparametric MRI (mpMRI) or surgical specimen. These radiologic and pathologic characteristics are inevitably associated with aggressiveness or prognosis of PCa (1112). Here, we will discuss the potential roles of PI-RADSv2 in assessing various aspects of PCa beyond its primary role in csPCa detection.
PI-RADSv2 Scoring and MRI Protocols
For PI-RADSv2 scoring, mpMRI consists of diffusion-weighted imaging (DWI) with/without dynamic contrast-enhanced (DCE) MRI for evaluating peripheral zone (PZ), and T2-weighted imaging (T2WI) with/without DWI for evaluating transition zone (TZ) (13). When the finding of the primary MR sequence is indeterminate for csPCa (e.g., a score of 3), findings of the secondary MR sequence (e.g., focal early enhancement in the DWI-suspected PZ lesion; focal areas of restricted diffusion, measuring 1.5 cm or greater, in the T2WI-suspected TZ lesion) can determine a final score of 3 or 4. The final PI-RADSv2 score using a 5-point scale is not for detecting every PCa, but for estimating the probability of csPCa.
It is recommended that some parameters of the essential MR sequences for scoring (e.g., T2WI, DWI, and DCE MRI) should be similar because they often have a complementary role in lesion characterization in the same prostatic region (14). At our institution, the field-of-view is uniformly 20 cm, and the slice thickness is 4 mm or less for the three MR sequences.
For acquiring an apparent diffusion coefficient (ADC) map, the monoexponential fit with the lowest b-value of 50−100 s/mm2 and the highest b-value of 800−1000 s/mm2 is appropriate. For analyzing high b-value DW images, PI-RADSv2 recommends image acquisition at a b-value of 1400−2000 s/mm2 by means of either a direct or synthetic method because of better lesion conspicuity without significant loss of signal-to-noise ratio (1516).
In DCE MRI, a temporal resolution of 7 seconds or less is preferred to assess focal, early enhancement in the prostate gland (13). Semi-quantitative or quantitative analyses of DCE MRI using dedicated software are optional. T1-weighted imaging (T1WI) is also recommended to evaluate post-biopsy hemorrhage, delineate the gland, and detect lymph node (LN) or skeletal metastases although it is not integrated into the process of PI-RADSv2 scoring. The MRI protocols required for PI-RADSv2 interpretation have been well summarized in a previous review article (14).
Beyond Cancer Detection
Gleason Score
Analysis of DWI enables assessment of histologic tumor aggressiveness (17). Because the degree of restricted diffusion reflects the architectural distortion of the extracellular space and tumor cellularity (18), PCa with higher GS typically manifests as a focal hyperintense lesion on high b-value DWI with low ADC value. Hence, there is an inverse correlation between tumor ADC and GS. In visual analysis of DWI, lesion conspicuity is greatly affected by differences in restricted diffusion between cancerous and benign tissues (19). Thus, PCa with higher GS and diffusion restriction shows good lesion conspicuity on DWI.
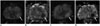
In PI-RADSv2, DWI is a major MR sequence for PZ evaluation, and it also determines the likelihood of csPCa when the findings of T2WI are equivocal for TZ (e.g., a T2WI score of 3) (13). Therefore, PI-RADSv2 scores are closely associated with lesion conspicuity on DWI. Based on this background, a certain degree of relationship among the degree of diffusion restriction, PI-RADSv2 scores, and GS is expected. In recent studies, PI-RADSv2 scores showed a positive correlation with GS (20). This helps PI-RADSv2 to verify the biopsy results (10, 21) (Fig. 1).
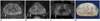
However, it is still uncertain which MR parameter is better correlated with GS. Basically, the interval of PI-RADSv2 scores is much greater than that of ADC values. Therefore, a particular score of PI-RADSv2 may comprise various ranges of GS (1) (Fig. 2). Conversely, there also may be a significant overlap of GS between neighboring PI-RADSv2 scores. For determining whether the PI-RADSv2 score is 4 or 5, the lesion size is an important factor (e.g., 1.5 cm). Thus, for GS 7 or greater PCa, the PI-RADSv2 score can be 4 when the tumor is small, while the score can be 5 when the tumor is large. Further studies are required to confirm which parameter better represents GS.
Tumor Volume
A tumor volume of 0.5 cm3 is the most commonly applied threshold to determine csPCa (22). However, mpMRI is inadequate for detecting small PCa. Tumor volume less than 1.0 cm3 is often associated with false negative diagnosis by means of mpMRI (2324). In addition, there are many benign mimickers in the prostate gland simulating PCa such as focal inflammation, stromal hyperplasia, central zone, anterior fibromuscular stroma, or surgical capsule (25). Thus, in case of a small PCa, there is a risk of false positive diagnosis by using mpMRI (e.g., a false diagnosis of the anterior fibromuscular stroma as a large anterior TZ PCa).
Vargas et al. (26) reported that more than 50% of PCa with GS 4 + 3 or greater were underestimated by PI-RADSv2 when the tumor volume is less than 0.5 cm3. Seo et al. (10) reported that more than half of the underestimated cases (e.g., PI-RADSv2 score less than 4 for csPCa) had tumor volume less than 1.0 cm3. Based on these data, there may be a discrepancy in the cutoff value of tumor volume between MR detectability and Epstein criteria (Fig. 3).
Multiparametric magnetic resonance imaging may also have a limitation in detecting sparse PCa. Sparse PCa consist of a mixture of scattered cancer cells and normal PZ tissues (27). Therefore, the volume of cancer cells in sparse PCa is inevitably smaller than that in dense PCs within the same region. Accordingly, it is expected that sparse PCa cannot be easily differentiated from adjacent normal prostatic tissues. Langer et al. (27) reported that ADC and T2 values of sparse PCas are similar to those of normal PZ tissues.
Based on these data, it should be determined whether the current Epstein criteria (1) GS > 3 + 3; 2) tumor volume ≥ 0.5 cm3; or 3) presence of extraprostatic extension [EPE]), especially for the tumor volume, are indeed the appropriate goal of PI-RADSv2, or they need to be changed: for example, 1) GS 3 + 3 PCa with tumor volume ≥ 1.0 cm3 or GS ≥ 3 + 4 PCa with any volume, or 2) only GS ≥ 3 + 4 PCa. Clinically, there is a debate regarding the tumor volume threshold for defining csPCa (282930).
Extraprostatic Extension
Extraprostatic extension is a well-established adverse prognostic factor in PCa (31). Thus, radiologic investigation for EPE is important in terms of predicting the prognosis and surgical planning. The MR findings of organ-confined PCa may lead to a nerve-sparing approach in surgery (32). Conversely, a more wide excision may be required to secure the safety margins when EPE is highly suspected. In prostate MRI, T2WI is the mainstay for assessing EPE because of its high spatial resolution (1333).
The imaging criteria for EPE suggested in PI-RADSv2 are as follows (13): 1) asymmetry or invasion of the neurovascular bundles, 2) a bulging prostatic contour, 3) irregular or spiculated margin, 4) obliteration of the rectoprostatic angle, 5) a tumor-capsule interface of greater than 1 cm, or 6) breach of the capsule with evidence of direct tumor extension or bladder wall invasion. In PI-RADSv2, the findings of definite EPE on a major MR sequence (e.g., DWI for PZ and T2WI for TZ) lead to a final score of 5.
In a previous study conducted by Kayat Bittencourt et al. (34), the analysis of a major MR sequence alone allowed comparable performance with combined analysis of mpMRI for EPE. Another study demonstrated that a score of 5 showed higher rates of EPE than a score of 4 (48.7% vs. 11.5%; p < 0.001) (35). Krishna et al. (36) also found that the rate of EPE sequentially and significantly increased according to PI-RADSv2 scores. These data indicate that PI-RADSv2 has the potential to assess the risk of EPE.
However, there may be controversy regarding the imaging criteria for ‘definite’ EPE because the degree of suspicion may be relatively different for each MR criterion. For example, measurable extracapsular extension may be a stronger indicator than findings of capsular abutment or irregularity caused by cancer (37). Also, MR findings of subtle capsular or extracapsular changes could be inconsistently interpreted depending on the discretion of radiologists (Figs. 4, 5). Furthermore, integrating T2WI in the evaluation of EPE is somewhat discordant with the dictionary definition of ‘definite EPE on DWI’ when PZ is evaluated. More discussions regarding the definition of ‘definite EPE’ may be required as the current PI-RADSv2 only provides various imaging findings of EPE without any specific grading system for each finding unlike the initial version of PI-RADS.
Lymph Node Metastasis
The status of pelvic LNs influences treatment planning. However, the currently available most optimal method for LN assessment is surgical LN dissection (32). Radiologically, pelvic LN metastases in PCa are often small (38). Thus, the use of the classical size criterion (e.g., 0.8−1.0 cm in short-axis diameter) alone is associated with the risk of underestimation in LN assessment (3940).
Previous studies have shown great promise in terms of advanced LN imaging: 1) MRI using ultra-small particles of iron oxide or 2) choline-based or prostate specific membrane antigen-based positron emission tomography scan (4142434445). However, these techniques have not been utilized at every institution (46). Therefore, the selection of optimal candidates to maximize the effectiveness of advanced imaging or pelvic LN dissection (PLND) is important in daily practice, as it reduces the medical cost or morbidity.
In practice, various clinical nomograms aid in selecting the patients who need PLND. The parameters used in nomograms are usually PSA, clinical stage, and biopsy information including GS and tumor burden (474849). Thus, the status of the primary lesion is closely related to the nodal status (1150). However, these parameters (e.g., stage, GS, or tumor burden) do not directly provide information regarding the anatomical status of PCa, thus miscalculation of the risk can occur (51).
As discussed earlier, PI-RADSv2 scores are associated with the status of GS, tumor volume, and EPE of PCa. Thus, there may be a certain degree of relationship between PI-RADSv2 scores and risk of pelvic LN metastasis. A recent study demonstrated that PSA, GS, and tumor stage were significantly different between patients with a score of 5 and the other patients (52). In the study, a cutoff score of 5 provided a positive predictive value of approximately 20%, while the negative predictive value was roughly 99% for normal-sized LN metastasis (Fig. 6). Therefore, the authors suggested that PI-RADSv2 may help predict a very low risk group for LN metastasis. Prospective validation is necessary for practical application.
Postoperative Biochemical Recurrence
Literatures have suggested that mpMRI may predict post-treatment prognosis following surgical (12) or non-surgical (53) treatment. Apparently visible lesions are more likely to be aggressive PCa with worse clinical outcomes, compared with PCa with poor lesion conspicuity. Zhang et al. (54) reported that PI-RADS version 1 was independently associated with time to biochemical recurrence (BCR), and adding the MR parameters to the clinical nomogram significantly increased the performance. Park et al. (20) reported that the 2-year BCR-free survival rates were significantly different among three PI-RADSv2 subgroups (approximately, 100% for patients with score 1−3; 90% for patients with score 4; and 70% for patients with score 5). This might be because various pathologic conditions of an index tumor or the risk of nodal invasion is reflected in PI-RADSv2. From this point of view, PI-RADSv2 may be one of the useful predictors for postoperative BCR. Long-term follow-up data and combined analysis of PI-RADSv2 scores with clinical parameters are currently necessary.
DISCUSSION
Prostate Imaging-Reporting and Data System Version 2 is an emerging tool for interpreting prostate MRI and it needs further validation regarding various aspects of PCa. Nevertheless, the data so far are promising. Based on the data discussed in this article, PI-RADSv2 seems to reflect tumor GS, tumor volume, EPE, nodal status, and postoperative BCR. Combined analysis of PI-RADSv2 scores with clinical parameters may maximize its effectiveness and may help in management planning. Therefore, as a non-invasive tool, PI-RADSv2 may play a role in evaluating various aspects of PCa as well as in detecting csPCa.




 XML Download
XML Download