

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
About 80% of all strokes in the anterior circulation are ischemic (1) and at least 20% of ischemic strokes are caused by carotid artery atherosclerosis (2). Luminal stenosis was a standard metric in the evaluation and intervention of stroke in the past. However, it is less reliable now as the majority of stroke patients exhibit mild to moderate rather than severe carotid stenosis (3). Moreover, it has been shown that only 5% of symptomatic patients with high-grade stenosis can benefit from excision of carotid plaques (4). In 2003, many scholars reached an agreement that it would be more appropriate to evaluate vulnerable plaques (VPs) (i.e., those likely to rupture or thrombose and potentially lead to stroke) than luminal stenosis (5,6). Pathological characteristics such as active inflammation, rich neovascularization, fibrous thin cap with large lipid-rich necrotic core, and plaque fissure are important features of VPs (7).
Various imaging techniques such as magnetic resonance imaging (MRI) (8), positron emission tomography-computer tomography (PET-CT) (9), intravenous ultrasound (IVUS) (10), and contrast-enhanced ultrasound (CEUS) (11) have been used to judge VP according to lumen stenosis and plaque morphology. However, they are expensive (MRI), invasive (IVUS and CEUS), or radioactive (PET-CT). The critical challenge in assessing VP with recently improved imaging modalities is that plaques with similar unstable morphologic features do not necessarily all have equal likelihood of rupture (12). It has been found that arterial stiffness is associated with the presence of intra-plaque hemorrhage, a risk indicator for plaque instability, in the general population (13).
Supersonic shear imaging (SSI) is a new ultrasonic elastography for real-time visualization of soft tissue viscoelastic properties, and shear wave velocity (SWV) or Young's modulus (YM) for region of interest (ROI) can be obtained quantitatively and dynamically (14). Specifically, an in situ transient plane shear wave is generated using acoustic radiation force impulse (ARFI) and the shear wave is then tracked using ultrafast ultrasound (US) imaging in real time during propagating. Within a given ROI defined by an electronic cursor, the maximum, mean, minimal, and standard deviation values of stiffness are produced (15). The most attractive aspect of using SSI in clinical practice is that diseased and healthy tissue can be distinguished since the propagation of a shear wave is directly proportional to a material's properties (16). An in vitro study has indicated that shear wave elastography (SWE) could quantify YM of carotid plaque phantoms with good reproducibility even in the presence of pulsatile flow (17). It has been proved that plaque stiffness measured by SWE may be superior to grayscale median for the evaluation of carotid plaque vulnerability (18). In fact, tissue stiffness measured by SWE is estimated by assuming that the generated shear wave propagates in an incompressible, homogeneous, isotropic, linear, elastic material and YM is typically estimated using the equation of “YM = 3 ρc2” (14). In the equation, the parameter c refers to SWV reflecting tissue stiffness (19). Here, SWV inside tissues at different depth is generated using ultrasonic focused beams and then tracked by an ultrafast scanner (14). However, atherosclerotic plaques do not always have these characteristics because they have multicomponent structures with irregular geometries undergoing large deformations resulting from pulsatile blood pressure. Despite a growing number of studies have used SSI in carotid plaque (20,21), only a few articles have mentioned this critical point (22). Thus, we focused on the parameter of SWV instead of YM.
Many previous articles have demonstrated that homocysteine level is significantly associated with ischemic stroke (23,24,25). For example, a cross-sectional study in Chinese adults has found that plasma level of homocysteine might be associated with advanced carotid plaque which constitutes high risks of stroke in male Chinese adults (23). High level of serum homocysteine in acute stroke is related to poor outcome (24) and long-term mortality (25). However, there is no paper about the relationship between plaque stiffness and homocysteine level. The objective of this study was to understand carotid plaque stiffness and its correlation with serum homocysteine level as well as provide more biochemical (homocysteine) and physical (SWV) information for clinicians to estimate the vulnerability of carotid plaque. We assessed the stiffness of carotid plaque by SSI and explored the clinical values of SSI via its connection with homocysteine level.
Go to : 
MATERIALS AND METHODS
Patients
We enrolled 142 ischemic stroke patients (76 males and 66 females) with carotid atherosclerotic plaques from October 2013 to August 2015. Their mean age was 66 years (range, 45–80 years). Ischemic stroke (IS) was diagnosed by two experienced neurologists according to CT or MRI findings. IS patient without extracranial carotid plaque detected by US was excluded from this study. Patients with obvious carotid pulsing, difficult breathing, uncontrollable hypertension, and other accompanying diseases such as seriously pulmonary and hepatic or renal dysfunction were also excluded. This study was approved by the Ethics Committee of the First Affiliated Hospital of the Medical College of Xi'an Jiaotong University on 5th July 2013. All patients provided written informed consents.
Atherosclerotic plaque was determined by at least 1.5 mm thickness of intima-medial protrusion into the lumen by conventional US (26). The lumen of artery and the bright echo zone caused by media-adventitia interface in the posterior wall were used as reference structure for defining echolucent and echogenic plaques, respectively (26). All participants were divided into two groups based on whether they had neurological symptoms or not. The symptomatic group was defined as having focal neurological symptoms related to ipsilateral brain hemisphere within the past six-month period while the asymptomatic group was defined as those who had no such symptoms but were detected through radiological findings by stroke physician (21).
Ultrasonic Equipment and Procedure
Ultrasound and SSI images were obtained using Aixplorer System (Supersonic Imagine, Aix en Provence, France) equipped with a 15-4 MHz linear array transducer under a uniform setting. The depth of image was 3 cm and the focus was equal to the level of plaque. The elastic scale ranged from 0–5.8 m/s. Gain was set at 60–70% and SWE option was penetration. Patients rested in supine position with head turned to the contralateral side. They could breathe freely. The unilateral common carotid artery and proximal segment of internal artery related to neurological symptom were scanned carefully with routine ultrasonography and US elastography. The number, location, echogenicity, and luminal stenosis of plaques were recorded at examination. When the trained examiner acquired a qualified grey scale image in longitudinal view, “SWE” button was activated. Box size of ROI was adjusted to include the carotid plaque. The probe was placed perpendicularly on the skin with slight pressure for 10 seconds to measure SWV as recommended by the manufacturer (27). Slight pressure was defined as placing the transducer very lightly on the top of a generous amount of coupling gel on the surface of the skin without deforming muscle thickness (27). The standardization compression of the probe is controlled by the equipped monitoring system for elastography quality. Real-time grey US and color-coded elastography were displayed on a split-screen. All patients were told to hold their breath and avoid swallowing for about 3–5 seconds in the middle of SSI examination. A 10-second length cine-loop with raw data was recorded.
SSI Analysis and Data Collection
Each plaque was examined independently by two trained sonographers (one intermediate and one senior) in a double-blind fashion. The SSI frame rate was 1 Hz. Approximately 10 frames were acquired in 10 seconds. The first three and the last three frames were discarded because of image instability. The remaining four frames were selected for elasticity measurements. Each plaque's elasticity was measured 8 times by the two independent sonographers who were blinded to the study. A series of data including SWVmean, SWVmax, and SWVmin (representing the mean, maximum, and minimum values of SWV, respectively) were auto-calculated by the Q-box software on each frame. They were then averaged for eight frames separately.
Serum biochemical indexes including triglycerides (TG), low-density lipoprotein (LDL), total cholesterol (TC), and homocysteine levels were tested. The normal reference for TG ranged from 0.4–1.6 mmol/L. For TC, the normal range was from 2.4–5.5 mmol/L. The normal level of LDL ranged from 2.07–3.10 mmol/L. Homocysteine level > 15 mmol/L was defined as hyper-homocysteinemia (H-hcy) (28).
Statistical Analysis
Statistical analysis was carried out using SPSS 18.0 (SPSS Inc., Chicago, IL, USA). Pooled analyses were performed for SWVmin, SWVmean, and SWVmax obtained from repeated measurement by the two independent sonographers. Intra- and inter-observer coefficients of variations (CVs) were calculated. SWVs differences between echolucent and echogenic carotid plaques were compared using Mann-Whitney U test. These data were displayed as mean followed by inter-quartile range. Correlations between SWVs and homocysteine levels were analyzed using Pearson correlation analyses. Binary logistic regression analysis was performed to determine the possible risk factors for symptomatic ischemic stroke. Receiver operating characteristic curves of SWVmean and homocysteine levels were used to assess the diagnostic power for carotid VP. A p value < 0.05 was considered statistically significant.
Go to :
RESULTS
Demographic and Clinical Characteristics
One hundred and forty-two ischemic stroke patients underwent routine ultrasonography and ultrasonic elastography by two sonographers. Thirteen patients were excluded, including 9 patients with both echogenic and echolucent plaques on the same side associated with symptoms and 4 patients whose internal carotid arteries were completely occlusive. Finally, a total of 129 (89.6%) patients were examined with SSI. The intra-observer CV was 13.7% and the inter-observer CV was 17.8%. These participants were divided into symptomatic (n = 85) and asymptomatic group (n = 44). Their demographic and clinical characteristics are summarized in Table 1.
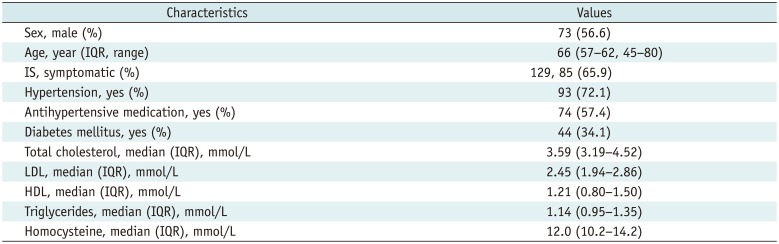
Table 1
Patients' Basic Characteristics
![]()
SWVs Difference between Echogenic and Echolucent Carotid Plaques
Of the 129 plaques, 78 were echolucent while 51 were echogenic. Only 1 (0.01%) plaque had stenosis of more than 50%. Measuring stiffness of echogenic and echolucent plaques with SSI is illustrated in Figure 1.
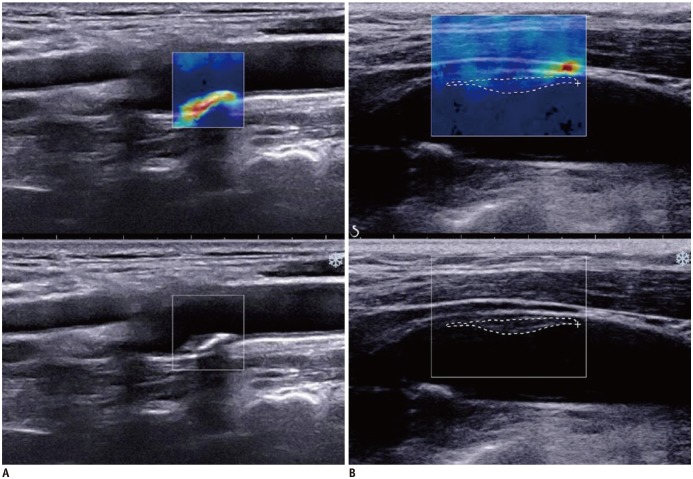 | Fig. 1SWVs measurements for echogenic and echolucent carotid plaques.
A. Maximum, mean, and minimum SWV for echogenic plaque on posterior wall of carotid artery was 5.64, 5.26, and 4.03 m/s, respectively. B. Maximum, mean, and minimum SWV for echolucent plaque on anterior wall of carotid artery was 3.59, 2.24, and 1.19 m/s, respectively. SWV = shear wave velocity
|
Echogenic plaques had higher SWVs than echolucent ones (SWVmin, 3.91 [3.24–4.17] m/s vs. 1.51 [1.04–1.94] m/s; SWVmean, 4.29 [3.98–4.57] m/s vs. 2.09 [1.69–2.41] m/s; SWVmax, 4.67 [4.33–4.86] m/s vs. 2.62 [2.32–3.31] m/s; all p values < 0.01). The numbers of the 78 echolucent plaque located on the anterior wall and the posterior wall were 18 and 60, respectively. For the 51 echogenic plaques, the numbers of plaques located on the anterior wall and the posterior wall were 14 and 37, respectively. The SWVs for echolucent plaques were still lower than those of echogenic plaques regardless whether plaques were located on the anterior wall or the posterior wall, all p values < 0.01 (Table 2).
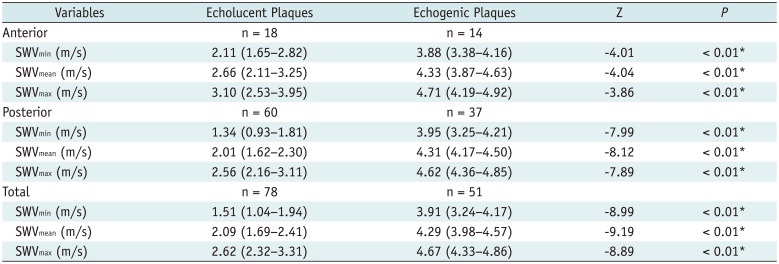
Table 2
Comparisons of SWV between Echolucent and Echogenic Plaques with and without Consideration of Their Depth on Anterior or Posterior Wall
![]()
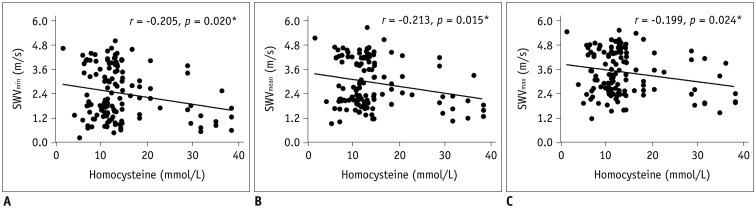
Correlation between SWVs of Carotid Plaque and Serum Homocysteine Level
Binary Logistic Regression Analysis
Based on the presupposition that symptom was the surrogate marker of VP, binary logistic regression analysis showed that sex (p = 0.008), LDL (p = 0.015), TG (p = 0.011), SWVmean (p = 0.004), and H-hcy (p = 0.010) had significant association with symptomatic ischemic stroke (Table 3). However, comorbidity such as hypertension and diabetes mellitus showed no statistically significant association. Besides, the area under curve (AUC) by homocysteine was 0.60 (95% confidence interval [CI], 0.50–0.70). It was improved after combing with SWVmean (AUC, 0.67; 95% CI, 0.57–0.77).
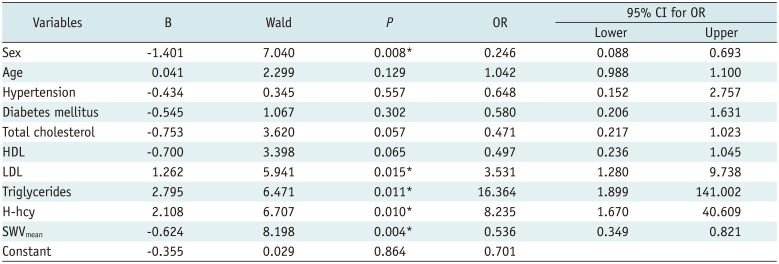
Table 3
Binary Logistic Regression Analysis
![]()
Go to :
DISCUSSION
Ultrasonic elastography (UE) is a new technique for obtaining tissue biomechanical characteristics. However, such important information cannot be acquired via conventional US. Since the first use of shear wave measurement to detect tissue elasticity using the acoustic radiation method (29), SWE has evolved from the initial one-dimensional transient UE to subsequent two-dimensional transient UE using ARFI and to current real-time SSI. Dahl et al. (30) have used ARFI to observe carotid plaques in vivo and demonstrate the feasibility of imaging mechanical properties of carotid plaques. It has been shown that SSI can distinguish between echolucent and echogenic plaques in a phantom setup with results similar to mechanical testing (22).
In our study, the reproducibility of plaque stiffness measured by SSI was close to that of a previous study (21). Our study revealed that SWVs for echolucent plaques were lower than those for echogenic plaques in the longitudinal view. This is consistent with Garrad's case report (20) showing that carotid plaques from a 70-year-old female who underwent SSI before carotid endarterectomy (CEA) had a higher stiffness (109.5 KPa) in the anterior wall but a lower stiffness (41.7 KPa) in the posterior wall with histologically revealed calcification and thrombus, respectively (20). Plaques that appear echolucent on routine US are usually lipid-rich or thrombus whereas echogenic plaques have higher content of fibrous tissue and calcification. We also found that the difference in SWV between echogenic and echolucent plaques was not affected by the depth of carotid plaque. However, plaque evaluated by ARFI in deeper areas such as on the posterior carotid wall might be biased because the radiation force reaching the vessel wall is weakened when absorption is high (30). Our results indicated that SSI had better quality than ARFI for measuring carotid plaque in deep area. Therefore, SSI is a feasible technique that can enable us to differentiate echogenic and echolucent plaques objectively.
This is the first study that reports on the correlation between SWV of carotid plaque and serum homocysteine level in ischemic stroke patients. Serum homocysteine level has been proved as an independent cardiovascular risk factors for stroke (3132). A prospective cohort study has confirmed that elevated homocysteine level can independently predict severe neurological impairment, poor functional outcome, and stroke recurrence in large artery atherosclerosis stroke subtype (31). Our finding demonstrated that SWVs and serum homocysteine levels were negatively correlated with each other. Besides, they were both significantly associated with symptomatic ischemic stroke. AUC was enhanced after combing SWVmean with H-hcy (AUC = 0.67) than H-hcy only (AUC = 0.60). These findings suggest that plaque SWV, similar to homocysteine, might be used as a potential predictive index for stroke. In the study, we were unable to provide SWV threshold with pathologic results as the gold standard. Nevertheless, the link between SWV and homocysteine inferred that lower SWV plaque might hint more dangerous compared to higher SWV plaque. Ramnarine's study has revealed that plaques associated with focal neurological symptoms had significantly lower mean YM than plaques in asymptomatic patients (62 kPa vs. 88 kPa; p = 0.01) (21).
In conclusion, SSI could be used clinically to distinguish stiffness between echogenic and echolucent carotid plaques. Moreover, carotid plaque SWV combined with H-hcy could improve its diagnostic power for symptomatic stroke. Therefore, parameters of SWV for carotid plaque together with serum homocysteine level might provide better understanding for ischemic stroke patients.
In this study, we did not evaluate all possible risk factors. Instead, we only focused on factors routinely available in our daily practice. This study has three main limitations. First, the sample size was relatively small and plaque characteristics were oversimplified (involving echolucent and echogenic plaques only). Second, temporal variation in SWV through the cardiac cycle was not evaluated in the present study. It has already been shown that plaque stiffness changes throughout the cardiac cycle (22). Third, we failed to provide a practically applicable SWV threshold with pathological results as pathologically golden standard because none of these participants underwent CEA. In addition, this cross-sectional study was from a single center with limitations, which may not be an accurate representation for all stroke patients. Nevertheless, this study reassured us that SSI, a non-invasive technique, might provide novel information (stiffness) to understand VPs in ischemic stroke patients.
Go to :
 XML Download
XML Download