

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Cases of chronic liver diseases (CLD) caused by the hepatitis B or C viral infection are estimated to have reached approximately 280 million worldwide. The prevalence of nonalcoholic fatty liver disease is rapidly increasing; in particular, nonalcoholic steatohepatitis is estimated to affect 10–15% of the population in the United States of America (12). To assess the severity of fibrosis caused by various CLD, hepatologists can use either invasive (liver biopsy) or noninvasive techniques (3). Because a liver biopsy provides information regarding the fibrosis stage, necro-inflammation, and fatty infiltration and reveals specific markers in certain hepatic diseases, this morphologic examination is considered to be the “gold standard” method for the assessment of liver diseases (45). However, we must take into account that after a diagnostic liver biopsy, severe complications, including death, may occur in 1–5% of the cases (6). In addition, liver biopsy has limitations of sampling bias due to the uneven distribution of liver fibrosis and the small size of the specimen (approximately 1/50,000 of the total volume of the liver), and considerable inter- and intra-observer diagnostic discrepancies in the biopsy assessments of liver fibrosis (7).
For these reasons, there is a need for noninvasive methods to assess the degree of fibrosis in liver diseases, including serologic tests for several direct and indirect markers of liver fibrosis (8) and elastographic techniques such as transient elastography (TE) and an ultrasound (US)-based shear wave elastography (SWE) method (91011). Several published studies have reported that TE (FibroScan; Echosens, Paris, France) is a reliable diagnostic tool for the noninvasive evaluation of liver fibrosis (1213). In recent years, several US-based point shear wave elastography (pSWE) methods and two-dimensional (2D)-SWE using acoustic radiation force impulse quantification have become commercially available for the noninvasive assessment of liver fibrosis (101415). Shear wave-based elastographic methods can be implemented in standard US systems that are used for several other purposes (e.g., standard US examination, Doppler evaluation, contrast-enhanced US); therefore, these devices may be more cost effective for the simultaneous evaluation of chronic liver disease and surveillance of hepatocellular carcinoma (16). Among these techniques, the Virtual Touch Quantification (VTQ; Siemens AG, Erlangen, Germany), which is a type of pSWE technique, has been studied the most. More recently, 2D-SWE techniques have appeared on the market, and although they are promising and involve larger sample volumes than the pSWE techniques, there are several published studies regarding this technique (1517).
S-Shearwave elastography (S-Shearwave; Samsung Medison, Hongcheon, Korea) was recently developed and is based on the same physical principles as VTQ; therefore, it is expected to show promising results in measuring liver stiffness (LS) in hepatic fibrosis patients, similar to other pSWE techniques (1819). LS measurements using pSWE techniques such as VTQ and S-Shearwave require only a few minutes using conventional US probes. So, it can easily be performed during a regular liver US session (1819). However, the fibrosis cutoff values for US elastographic techniques are manufacturer dependent because of the variability in velocity measurements (9). So, depending on the US equipment used, its levels of technical success and reliable measurement of tissue stiffness and reproducibility of LS measurements for assessing LS must be determined before its clinical adoption for liver US examination (2021). However, until now, there has not been any studies that validate this new pSWE (S-Shearwave) and compare the performance of S-Shearwave with other previously introduced SWE techniques.
Therefore, the aims of this study were to estimate the validity of a new pSWE (S-Shearwave) technique by evaluating the reproducibility of measurements, and to compare the performance of S-Shearwave to that of VTQ considering the LS values measured by TE as the referenced standard.
MATERIALS AND METHODS
Study Population
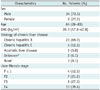
This prospective study was approved by our Institutional Review Board, and written informed consent was obtained from all patients. From July to September 2016, 33 patients who were referred to the Radiology department for US examination before locoregional treatment of suspected small malignant liver tumors. Among them, 30 patients were diagnosed with CLD based on laboratory tests or clinical findings (22) and 3 patients had no parenchymal liver disease. The most common etiology of CLD was chronic hepatitis B (23/33, 69.7%), followed by chronic hepatitis C (4/33, 12.1%) (Table 1).
Liver stiffness values obtained by TE were used for the assignment of hepatic fibrosis stage in accordance with the referenced values provided by a previous meta-analysis (1223). Detailed characteristics of the study population are provided in Table 1. To assess the technical success rate (SR) and reliable measurement of the two pSWE techniques, the results of all 33 patients were included. For the comparison of two pSWE techniques (VTQ vs. S-Shearwave), only patients who had reliable LS values in both examinations and TE were included (Fig. 1).
Virtual Touch Quantification and S-Shearwave Measurements
Virtual Touch Quantification was performed using the Siemens Acuson S2000 Virtual Touch US system (Siemens AG), and S-Shearwave was performed using the Samsung RS 80A US system (Samsung Medison). In general, at least 10 measurements should be obtained; although, some studies suggest that a smaller number of measurements may have similar accuracy (1316). Technical failures and unreliable results occur more frequently in patients with liver cirrhosis than in patients with a normal liver (13). Hence, 15 measurements were made with each instrument per patient. All patients fasted for at least 6 hours prior to the examination and were placed in the supine position with the right arm maximally abducted above the head to stretch the intercostal muscles. One attending radiologist, who was blinded to the TE results and had 6 years of experience in US elastography and 20 years of experience with liver USs, performed VTQ and S-Shearwave. The LS measurement was done using the intercostal approach by placing the region of interest in the right anterior segment of the liver. The focal liver lesions and vessels were carefully avoided and a measurement depth of 25–45 mm was maintained from the liver capsule (Fig. 2). While the LS values were being measured, patients were instructed to hold their breath for approximately 5–7 seconds (1624). After all 15 measurements were acquired, we removed the measurement with lower than 0.4 calculated reliability measurement index (RMI) in order to increase the reliability (20). RMI is an automatically calculated value in the S-Shearwave that is obtained by the weighted sum of the residual of the wave equation and the magnitude of the shear wave when performing each stiffness measurement (20). The median value of LS measurements was automatically calculated and expressed in kilopascals (kPa). To avoid potential bias, the summary of the serial measurements of each technique was not available to the operator until two examinations were completed (1624).
Additional sessions were done with S-Shearwave to evaluate intra- and inter-observer agreement. After the initial measurement of S-Shearwave, another session of measurements was performed by the same operator within 8 hours to evaluate the intra-observer reproducibility of the LS measurements using S-Shearwave. The LS measurements were repeated within 1 hour of the second measurement by one of three other radiologists with 1–5 years of clinical experience, who was blinded to the TE results and the results of the other exam. The mean, median, and standard deviation values of the LS measurements were provided in US units. The interquartile range (IQR) was calculated using statistical software.
Definition of Technical Failure and Reliable (or Unreliable) Measurement
Technical failure of SWE methods was defined as failure to acquire 10 valid measurements after at least 15 trials. The reliable measurement of LS was defined as a measurement in which the IQR/median LS of 15 measurements was less than 30% (13).
A reliable measurement of TE was defined as the median of 10 valid LS measurements with a SR (ratio of number of successful acquisitions to total number of acquisitions) greater than or equal to 60% and an IQR/median ratio (IQR = difference between 75th and 25th percentiles, essentially the range of the middle 50% of the data) of less than 30%, as described in detail previously (25). The TE measurement was defined as having failed if no valid measurement was obtained after at least 10 attempts.
Standard of Reference for Hepatic Fibrosis
Because TE is a validated method for the evaluation of liver fibrosis (1226), it was considered the reference method against which the performance of VTQ and S-Shearwave techniques was assessed. To discriminate between the various stages of fibrosis with TE, we used the latest published LS cutoffs as proposed in Chon et al.'s meta-analysis (12): 7.9 kPa for moderate fibrosis (F ≥ 2), 8.8 kPa for severe fibrosis (F ≥ 3), and 11.7 kPa for liver cirrhosis (F = 4).
Transient elastography was measured by a technologist who was blinded to both VTQ and S-Shearwave results. The median interval of TE for the two examinations was 20 days (range: 5–31 days). For each patient, 10 valid TE measurements were performed under fasting conditions. The patient was in the supine position, using the intercostal approach, with the right arm in maximal abduction, as described in detail previously study (27). A standard XLprobe was used. The median value was calculated and expressed in kPa (13).
Statistical Analysis
The χ2 analysis was used to determine whether the technical success and reliable measurements of the two pSWE methods were significantly different. The Wilcoxon signed-rank test was used to compare the LS measurements obtained by VTQ and S-Shearwave. The Spearman correlation coefficient was then obtained to determine the correlation between the two pSWE techniques (28). A Bland–Altman analysis was used to evaluate the agreement between the VTQ and S-Shearwave techniques (29). The agreement between the two methods was further investigated by calculating the intraclass correlation coefficient (ICC) from the mean VTQ and S-Shearwave LS measurements. The intraand inter-observer reproducibility of the LS measurements using S-Shearwave was evaluated by calculating the ICC in 28 patients who underwent two sessions of S-Shearwave. As in previous studies, an ICC greater than 0.75 was considered to be a good agreement (30). To estimate the magnitude of change in LS measurements that can confidently be detected in a single individual, a 95% limit of agreement between repeat S-Shearwave measurements was obtained and then followed by the Bland-Altman method. The estimate was expressed as a percentage of the mean (29).
The areas under receiver operating characteristic curve (AUROC) curves and their 95% confidence intervals (CIs) were built for VTQ and S-Shearwave with regard to the diagnosis of severe fibrosis (F ≥ 3) or liver cirrhosis (F = 4) (31). The optimal cutoff values were determined using the highest Youden Index. The results for sensitivity (Se) and specificity (Sp) were recorded. The DeLong test was used to compare AUROC curves. A 95% CI was calculated for each predictive test, and a p value less than 0.05 was considered statistically significant. Because the fibrosis staging system using TE is not a binary reference, the use of only a receiver operating characteristics curve analysis may have led to an overestimation of the diagnostic performance. Thus, the overall performance was obtained using the Obuchowski measure with a R package (32). All statistical analyses were performed using commercially available software programs (SPSS version 21, IBM Corp., Armonk, NY, USA; MedCalc, version 14, MedCalc Software, Mariakerke, Belgium) and a free software program (R version 3.4.1; R Package for Statistical Computing, www.r-project.org).
RESULTS
The presumed distribution of liver fibrosis calculated from TE examinations showed that liver cirrhosis (F4) was the most common fibrosis stage (13/33, 39.4%), followed by severe (F3) and moderate (F2) liver fibrosis (27.3% and 21.2%, respectively), and lastly, mild (F1) or no (F0) liver fibrosis (12.1%) (Table 1) (23).
Technical Success Rate and Reliable Measurements
Among the 33 patients who underwent pSWE imaging with both techniques, five patients were excluded due to lack of TE data within 3 months (n = 1), unreliable measurement of TE (n = 1), technical failuare on S-Shearwave measurement (n = 1), unreliable measurement of VTQ (n = 1) and unreliable measurement of S-Shearwave (n = 1). Indeed , two pateints show unreliable measurements for S-Shearwave but one patient was already excluded due to unreliable measurements for VTQ. Ultimately, 28 patients were included for cross validation of VTQ and S-Shearwave measures.
There were no technical failures with VTQ and one technical failure with S-Shearwave because of severe obesity (body mass index [BMI] = 39). There was no significant difference in the technical SRs of VTQ (100%, 33/33) and S-Shearwave (96.9%, 32/33) (p = 0.63). Approximately 3.1% (1/33) of the VTQ measurements were unreliable and 6.3% (2/32) of the S-Shearwave measurements were unreliable. There was no significant difference in the reliable measurement rate (p = 0.61). All three unreliable measurements were observed by the operator in patients with obesity (BMI = 36), with or without a subjective poor sonic window because of advanced liver cirrhosis. Among these, one patient also failed to demonstrate a reliable measurement with S-Shearwave. One patient, where a technical failure was experienced with S-Shearwave, showed a reliable measurement with VTQ.
Correlation of LS Values between VTQ and S-Shearwave
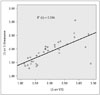
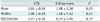
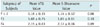
In the 28 patients who had reliable VTQ and S-Shearwave measures, the LS value for both exhibited a good, positive correlation (r = 0.78, p < 0.0001) (Fig. 3). Significant correlations among LS values by VTQ elastography and S-Shearwave were also obtained in various subgroups of the study's sample (Table 2). The mean LS values for S-Shearwave were not significantly different from those for VTQ: 1.88 ± 0.36 m/s vs. 2.01 ± 0.56 m/s, p = 0.25 (Table 3). The mean LS values assessed by S-Shearwave were not significantly different from those obtained by VTQ in hepatic fibrosis stages F ≤ 2 to F4 (Table 4).
Inter- and Intra-Observer Reproducibility of S-Shearwave Measurements
The intra-observer reproducibility of S-Shearwave measurements was calculated by comparing the repeat LS values obtained from 28 patients. The ICC of 28 S-Shearwave measurements was 0.99 (95% CI 0.97–0.99), which indicates very good reproducibility. The 95% Bland-Altman limit of agreement for the repeat S-Shearwave measurements was -0.029 of the mean (Fig. 4A). With respect to inter-observer reproducibility of the S-Shearwave technique, ICC values were 0.98 (95% CI 0.95–0.99) which indicates very good reproducibility. The Bland-Altman limit of agreement for the repeat S-Shearwave measurements was −0.014 of the mean (Fig. 4B).
Performance of VTQ and S-Shearwave in Detecting Significant Fibrosis, (F ≥ 2), Severe Fibrosis (F ≥ 3) and Liver Cirrhosis (F = 4)
For LS cutoff values greater than 1.33 m/s, VTQ had 100% Se, 75.0% Sp, 88.86% positive predictive value (PPV), and 100% negative predictive value (NPV) (AUROC = 0.89, 95% CI 0.73–0.97, p < 0.0001) to differentiate between subjects with or without significant fibrosis (≥ F2). The S-Shearwave cutoff value discriminating between these two categories was greater than 1.54 m/s, with 88% Se, 87.5% Sp, 93.3% PPV, and 78.5% NPV (AUROC = 0.80, 95% CI 0.63–0.92, p = 0.002). The AUROCs of the two methods were not significantly different (p = 0.13) (Fig. 5A).
Both VTQ and S-Shearwave techniques were efficient in differentiating between mild and moderate fibrosis (F ≤ 2) from patients with severe fibrosis and cirrhosis (F ≥ 3), respectively (Fig. 5A). For LS cutoff values greater than 1.56 m/s, VTQ had 86.4% Se, 81.8% Sp, 90.36% PPV, and 92.3% NPV (AUROC = 0.87, 95% CI 0.70–0.96, p = 0.0001) to differentiate between subjects with or without severe liver cirrhosis. The S-Shearwave cutoff value discriminating between these two categories was greater than 1.67 m/s, with 86.4% Se, 80.8% Sp, 89.2% PPV, and 92.2% NPV (AUROC = 0.84, 95% CI 0.67–0.94, p = 0.009). The AUROCs of VTQ and S-Shearwave for predicting the presence of severe cirrhosis (F ≥ 3) was not significantly different (p = 0.51) (Fig. 5B).
For cirrhosis detection, VTQ had 100.0% Se, 82.4% Sp, 98.36% PPV, and 96.3% NPV (AUROC = 0.89, 95% CI 0.74–0.97, p = 0.0006) using a cutoff value of 1.72 m/s; and S-Shearwave had 100.0% Se, 82.3% Sp, 97.9% PPV, and 95.8% NPV (AUROC = 0.94, 95% CI 0.80–0.99, p = 0.007) when applying the cutoff value of greater than 1.75 m/s. The AUROCs of the two pSWEs for predicting the presence of liver cirrhosis (F = 4) were also not significantly different (p = 0.48) (Fig. 5C).
In both methods, the Obuchowski measures were similarly high (0.94 and 0.95 for S-Shearwave and VTQ, respectively).
DISCUSSION
In our prospective study, both the VTQ and S-Shearwave techniques provided excellent levels of technical success and reliable measurement, and there was no significant difference between them. Unreliable measurements were recorded in two patients with the S-Shearwave technique; one owing to obesity and the other due to a poor sonic window. That result corresponded with previous studies reporting less than 3% measurement failure with SWE (2325). In addition, the mean LS measurements obtained by VTQ (2.01 ± 0.56 m/s) and S-Shearwave (1.98 ± 0.66 m/s) did not reveal any significant difference (p = 0.25) and showed good correlation (r = 0.78). Considering that both pSWE techniques are based on similar physical principles of developing shear waves and measurement of shear wave propagation, these results were expected (33, 34). Our results demonstrating reliable SWE measurements (VTQ: 96.9%, 32/33 and S-Shearwave: 93.7%, 30/32) are well correlated with those of Yoo et al. (35), who compared ElastPQ and VTQ in 85 patients (95.3% vs. 97.5%). Furthermore, the S-Shearwave technique showed similar accuracy compared to VTQ in the diagnosis of severe fibrosis (F ≥ 3, AUROC 0.84 and 0.87, respectively) and cirrhosis (F = 4, AUROC 0.94 and 0.89, respectively) using the LS values of TE as a standard of reference for liver fibrosis.
To our knowledge, many studies have already investigated the reproducibility of US elastography with respect to both intra- and inter-observer variability (363738). In our study, the reproducibility of the S-Shearwave results was excellent for both intra-observer (ICC = 0.99) and inter-observer (ICC = 0.98) variability. Our results are similar to the intra-observer reproducibility of another pSWE LS measurement (ICC = 0.99) (35) and were slightly better than the intra-observer reproducibility of VTQ reported in a previous study (ICC = 0.945) (39). Moreover, in our study, even though the two operators had different levels of experience in US elastography, the S-Shearwave method showed an excellent ICC in inter-observer reproducibility. This result is different from that of a previous study which showed that operator experience is related to the intra-observer variability of SWE (40). This discrepancy could be attributed to the S-SWE technique of automatically measuring RMI. Initial studies in both phantom and in vivo studies showed that RMI values are strongly correlated with reproducible measurements (20), and therefore, we may assume that RMI filtered out unreliable measurements and resulted in an improvement of inter-observer agreement in the LS measurement of S-Shearwave.
The diagnosis and stage of liver fibrosis, with the exception of early compensated liver cirrhosis, are important in treatment decisions and surveillance of patients with chronic liver disease (14). In daily practice, more than one SWE method can be used for the longitudinal assessment of liver fibrosis during the management of chronic liver disease over time. Therefore, for the longitudinal assessment or monitoring of liver fibrosis, the interchangeability of LS measurements by different SWE techniques may be of significant value. According to our results, although both VTQ and S-Shearwave exhibited similar values of the LS measurements, accuracy in diagnosing significant fibrosis and liver cirrhosis, and similar cutoff values for the fibrosis stages provided by the meta-analysis of LS measurements (14), these techniques cannot be used interchangeably because of the different cutoff values. Given the small number of patients included in the study's sample (28 patients), further research with a larger sample size is warranted.
Several noninvasive imaging methods, either US- or MR-based SWE techniques, have been evaluated to date for the assessment of LS and are showing good diagnostic accuracy for stage F ≥ 2 fibrosis and excellent diagnostic accuracy for liver cirrhosis (41). In the literature, most studies have been performed using TE followed by pSWE, 2D SWE, and MR elastography (MRE), and to date, comparable results have been reported for the assessment of liver fibrosis by these imaging methods (354142). Thus far, only TE has been accepted as a noninvasive test for the assessment of liver fibrosis in the European and American guidelines for the management of patients with chronic hepatitis C virus infection (4344) and the WHO guidelines for the prevention, care, and treatment of persons with chronic hepatitis B virus infection (45). However, point and 2D SWE can provide the advantage of being integrated into conventional US systems, thus enabling hepatocellular carcinoma surveillance with the same machine. Such is not possible with TE (41). Several papers have suggested an additional diagnostic benefit when elastography is used with conventional ultrasonography, as this enables the early identification of patients with compensated liver cirrhosis that would not be detectable by conventional ultrasonography (no liver cirrhosis signs) or laboratory values (no thrombocytopenia) (41464748). Since 2D SWE methods allow detailed monitoring of shear waves over a large area of liver parenchyma, they provide an advantage over both TE and pSWE (21). However, minimizing probe pressure when imaging superficial tissues is required to avoid artifacts near the surface (21). The MRE technique also provides quantitative maps of tissue stiffness over large regions of the liver. Furthermore, it is much less operator dependent and less affected by obesity or ascites (49), all of which may limit the application of pSWE. However, pSWE seems to be more time efficient and easy to access in daily practice than the MRE is and has comparably good performance in most patients (46).
The current study has several limitations. Since there was no pathological staging of liver fibrosis, we could not evaluate the diagnostic performance of the S-Shearwave technique in the staging of liver fibrosis using pathologic results. However, it should be mentioned that a liver biopsy for fibrosis staging is not completely reliable due to the significant sampling error and interobserver variability and has a potential for complications (67). In addition, we included only a small number of patients (28) so further prospective studies with a larger number of patients, including healthy volunteers, are needed to determined cutoff values for the liver fibrosis stages. Additionally, we used the LS cut off values for the staging of liver fibrosis that have been proposed for patients with chronic hepatitis B even though we included heterogeneous epidemiology of liver disease (12). However, a large percentage (69.7%, 23/33) of the patients in this study had chronic hepatitis B. Finally, although there are other clinically available SWE techniques such as 2D SWE, we merely compared two commercially available pSWE techniques.
In conclusion, the S-Shearwave method provided a high technical SR and reliable LS measurements as well as a diagnostic performance comparable to VTQ for fibrosis staging, while proving high intra-and inter-observer reproducibility.





 XML Download
XML Download