

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Reports indicate that the incidence of incidentally detected cystic pancreatic lesions (CPLs) on CT and MR images ranges between 2% and 38%, and increases with age (12345). Pancreatic cysts found in asymptomatic patients are comprised of a wide range of disease entities from benign to potentially malignant lesions (678910). Among these lesions, pseudocysts were previously considered to be the most frequently encountered cystic lesions, especially when the lesions were unilocular in morphology (811). However, recent studies have shown that neoplastic cysts account for the majority of CPLs in patients without a clinical history or evidence of pancreatitis (51213). Fernández-del Castillo et al. (12) reported that a pseudocyst was diagnosed in only 4% of asymptomatic patients with incidental CPLs. Thus, the increase in the frequency of CPL detection has paralleled a rise in concerns regarding its management (1011).
Previous studies pertaining to incidentally detected unilocular CPLs of diameter less than 3 cm suggest that the lesions may be safely monitored with serial imaging instead of further workup (911). However, it is highly plausible that a considerable amount of neoplastic, mucin-producing cystic lesions actually present as small (< 3 cm), unilocular CPLs (131415161718). Small unilocular CPLs may have occult malignancy in fewer than 5% of cases (9). It is well known that even benign-looking CPLs can increase in size as time goes on (561019). Furthermore, in cases of CPLs ≥ 3 cm in diameter, the risk of malignant foci was reported to be greater than four times that of cysts < 3 cm (20). To our knowledge, very few explicit studies have hitherto examined patient cohorts with only incidental, small CPLs showing unilocular morphology with respect to features associated with a size increase and development of features suggestive of a potential malignant nature (6919).
Therefore, in this study, we sought to retrospectively investigate features of incidentally detected unilocular CPLs measuring less than 3 cm in diameter that could predict a size increase and development of potential malignant features during subsequent follow-up.
Go to : 
MATERIALS AND METHODS
Patient Population
The patient cohort was recruited by searching our radiology database, which contained all radiological imaging reports prepared between November 2003 and December 2014. The key words used for data collection were ‘pancreas,’ ‘pancreatic,’ ‘cyst,’ ‘cystic lesion,’ ‘cystic tumor,’ ‘cystic neoplasm,’ ‘intraductal papillary mucinous neoplasm and intraductal papillary mucinous tumor,’ ‘IPMN and IPMT,’ ‘serous,’ ‘mucinous,’ ‘cystadenoma,’ ‘mucinous cystic neoplasm’ and ‘MCN.’ These search terms retrieved 1514 patients who had CPLs that were detected on CT or MR images. Among them, only those who met all the following criteria at the time of initial detection of the lesion were enrolled for the final analysis: 1) pancreatic lesions incidentally detected during evaluation for other medical issues and no symptoms attributable to the pancreatic lesions; 2) available serial CT or MR images with an interval of more than six months between initial and final imaging; 3) unilocular CPLs, irrespective of the lesion contour (round or oval); 4) CPLs with the largest diameter of less than 3 cm; 5) no radiological features suggestive of malignancy; and 6) no history of pancreatitis. Symptoms considered indicative of pancreatic dysfunction included upper abdominal pain, abdominal pain that radiates to the back, tenderness or palpable mass on epigastrium, weight loss, jaundice, and steatorrhea (921). CPLs with a wall thickness < 2 mm and without discernible enhancing septum traversing the cyst lumen were defined as ‘unilocular.’ Radiological features suggestive of a possible malignant nature included thickened/enhancing cyst walls (septa); mural nodules; and enhancing solid component within the CPLs.
Imaging Protocols
CT
During the follow-up period, CT examinations were performed using various multidetector-row CT (MDCT) equipment (LightSpeed QX/i, LightSpeed16, LightSpeed VCT, Discovery CT750 HD; GE Healthcare, Milwaukee, WI, USA; Sensation Cardiac 64, Somatom Definition Flash; Siemens Healthineers, Erlangen, Germany). The routine abdominal CT protocol consisted of both unenhanced and contrast-enhanced scanning. An unenhanced CT was initially performed from the hepatic dome to the right hepatic angle. Then, portal venous-phase imaging was performed after intravenous injection of 100–150 mL of iodinated contrast material at the rate of 2.5–4 mL/sec through the antecubital vein. In patients suspected to have a hepatic lesion and undergoing follow-up imaging due to known CPLs, triple-phase (the arterial, portal venous, and delayed phase) and dual-phase (the arterial and portal venous phase) contrast-enhanced CT were performed, respectively. After initiating the injection of the contrast material, a scan delay of 25–40, 70–80, and 150–180 seconds was applied for the arterial, portal venous, and delayed phases, respectively. The parameters of MDCT were 3–4 mm section thickness, 0.8–1 beam pitch, and 3–4 mm reconstruction interval. The raw data were routinely reformatted in the coronal plane with a section thickness of 2–3 mm and an interval of 2–3 mm.
MR Imaging
MR examinations were conducted using either a 1.5T (Signa HDxt; GE healthcare, Milwaukee, WI, USA) or a 3T MR scanner (Magnetom TrioTim; Siemens Medical System, Forchheim, Germany) with a phased-array body coil. T1-weighted images were obtained using the liver acquisition with volume acquisition (LAVA) and the volumetric interpolated breath-hold examination (VIBE) techniques. T2-weighted images were obtained using the single-shot fast spin echo and the half-Fourier acquisition single-shot turbo-spin echo techniques. Dynamic contrast-enhanced images were obtained using the LAVA and VIBE techniques. MR cholangiopancreatography images were obtained using the three dimensional (3D) fast-recovery fast-spin echo and 3D sampling perfection with application of optimized contrasts using different flip-angle evolution sequence with fat saturation on both 1.5T and 3T MRI systems. Contrast-enhanced MR imaging was performed after intravenous bolus injection of 0.1 mmol/kg (0.2 mL/kg) of Gadoterate meglumine (Dotarem; Guerbet, Villepinte, France) or 0.025 mmol/kg (0.1 mL/kg) of Gadoxetic acid (Primovist; Bayer Healthcare, Berlin, Germany) with an MRI-compatible injector (Sonic Shot; Nemoto Kyorindo, Japan) at a flow rate of 1–1.5 mL/sec. The extension tube was immediately flushed with 20–25 mL of 0.9% saline solution administered at the same injection rate as that used for the contrast agent. Axial images were obtained at 30, 60, and 180 seconds after injection of the contrast agent. Contrast-enhanced coronal images were additionally acquired at 5 minutes. The imaging parameters of each MR imaging protocol are summarized in Table 1.
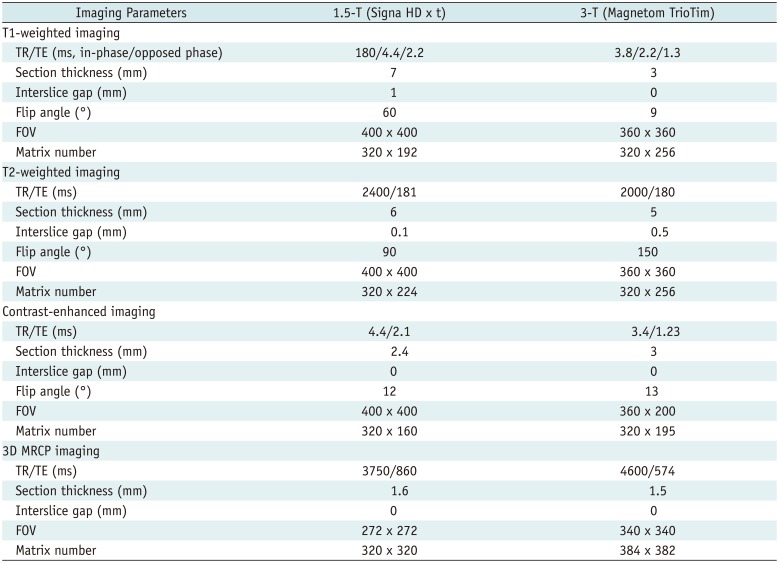
Table 1
Imaging Parameters of Various MR Imaging Protocols
![]()
Image Analysis
All the initial and subsequent follow-up CT and MR images were retrospectively reviewed in consensus by two abdominal radiologists who were blinded to the clinical history and pathologic analyses, but aware of the aim of this study. All CT and MR images were reviewed on a picture-archiving and communication system workstation (PACS; Marotech 5.4, Seoul, Korea). The reviewers were allowed to adjust the window width and level on the PACS monitor. They recorded the number, size, and location of CPLs on the initial and serial CT and MR images. The lesion size was measured in the plane that showed the largest diameter using an electronic caliper. Interval increase or decrease in the lesion size was defined as at least a 2 mm change in the maximal lesion diameter. The location of the lesions was classified into the head, neck, body, and tail of the pancreas. In addition, dilatation of the main pancreatic duct (MPD), the presence or absence of worrisome features (thickened/enhancing cyst walls [septa], main duct size 5–9 mm, mural nodule), and high-risk stigmata of malignancy (enhancing solid component within cyst, MPD ≥ 10 mm in size) according to the International Association of Pancreatology (IAP) guidelines (22) were also evaluated on follow-up images. MPD dilatation was recorded when its diameter was > 3 mm (23). All CPLs were classified into two groups, increase and no-increase groups, based on the interval change in lesion size. Subjects in the increase group were further classified into two subgroups, < 3 cm and ≥ 3 cm according to the lesion size at the last follow-up measurement. Lesions that showed no change, interval decrease in lesion size, or complete resolution during follow-up were classified into the no-increase group. All the CPLs were evaluated individually at follow-up examinations. To perform a patient-based analysis, we chose to consider the most advanced-looking dominant lesion (showing a potential malignant nature, interval increase, and the largest one at last imaging in descending order) in patients who had more than one CPL.
Statistical Analysis
The increase and no-increase groups, as well as the two subgroups in the increase group (CPL diameter at the last follow-up of < 3 cm vs. ≥ 3 cm) were compared using the Student's t test and the chi-square test, according to the data types. The association of various variables such as age, sex, follow-up duration, initial cyst size, lesion location, and lesion number (single vs. multiple), MPD dilatation at initial imaging with the lesion size increase and the development of worrisome features or high-risk stigmata of malignancy during the subsequent imaging surveillance were explored using multiple logistic regression analysis. In the increase group, we explored an optimal cut-off for the initial cyst size to predict later lesion growth to and beyond 3 cm in diameter using the receiver operating characteristics (ROC) curve analysis and the Youden index. All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 23.0 (IBM Corp., Armonk, NY, USA). A p value less than 0.05 was considered significant.
Go to :
RESULTS
Study Population
After reviewing the imaging findings and clinical records, 553 patients (282 men and 271 women; age range: 31–83 years; mean age: 62.2 ± 19.8 years) with 641 CPLs were included in this study (Fig. 1). Patients were monitored with follow-up CT only (n = 412), MR imaging only (n = 26), or both CT and MR imaging alternatively (n = 115). The follow-up period ranged from six to 129 months (mean: 34.5 ± 26.8 months), and the interval between follow-up examinations ranged between one and 126 months (mean: 12 ± 15.1 months). The baseline features of patients and CPLs are summarized in Table 2.
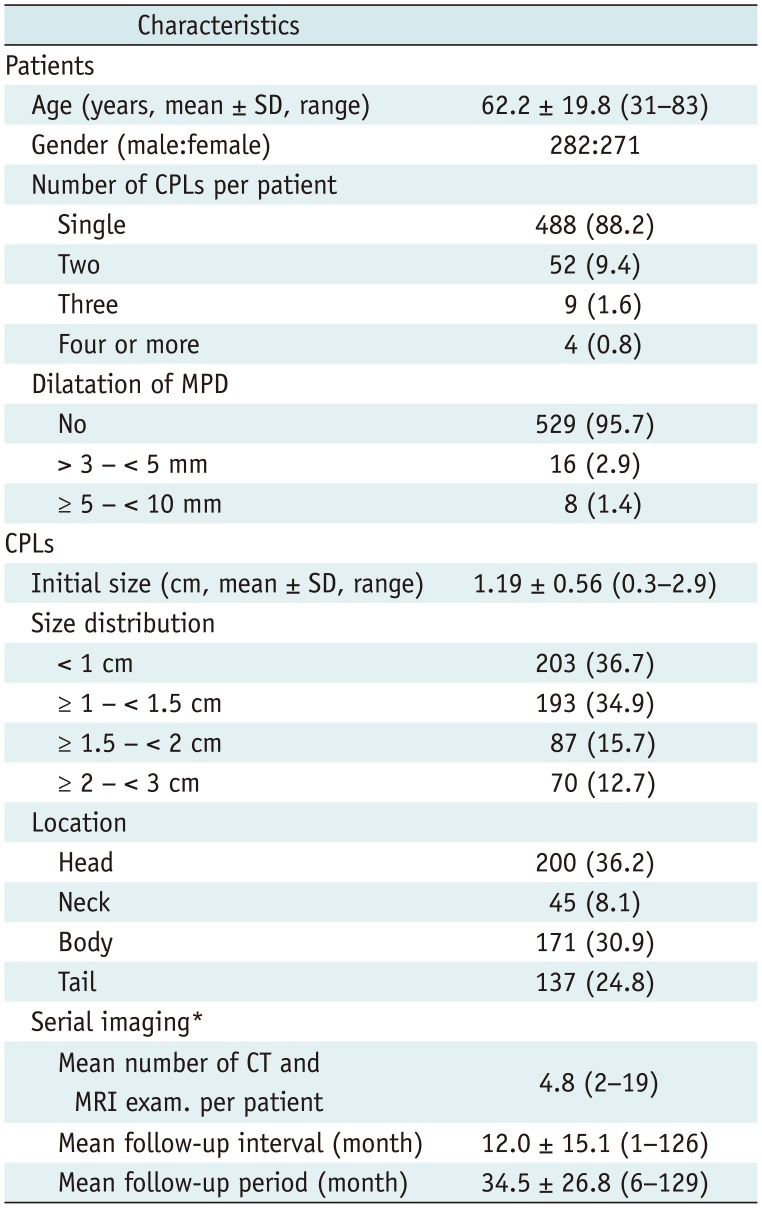
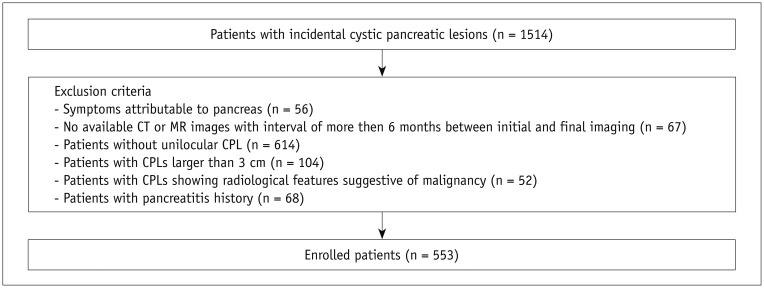
Table 2
Baseline Characteristics of Study Patients and Lesions
![]()
During the follow-up, nine patients underwent surgical resection for the following reasons: 1) increased cyst size (n = 3); 2) development of thick enhancing wall (n = 2); 3) dilatation of the MPD (n = 2); and 4) patient's request (n = 2). In addition, a pathologic diagnosis was made through endoscopic, ultrasound-guided, fine needle aspiration (n = 6) and percutaneous ultrasound-guided biopsy (n = 1) due to patient's request to make a pathological diagnosis (n = 3), dilatation of the MPD (n = 2), an increase in the size of CPLs during follow-up (n = 1), and occurrence of enhancing solid component (n = 1). Pathological examinations confirmed that 13 CPLs were benign cysts, four were pseudocysts, three were mucinous cystadenomas with low-grade dysplasia (Fig. 2), two were IPMNs with low-grade dysplasia (Fig. 3), two were lymphoepithelial cysts, one was a serous cystadenoma, and one was a simple serous cyst. Three CPLs were diagnosed as ductal adenocarcinoma (Fig. 4), mucinous cystadenocarcinoma, and intraductal papillary mucinous carcinoma.
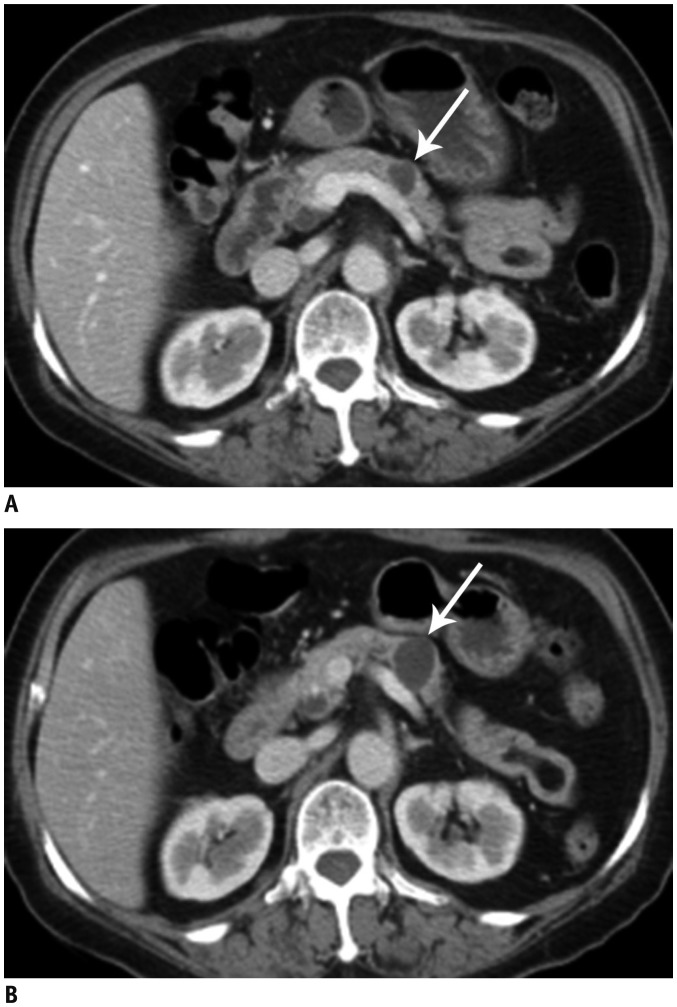 | Fig. 268-year-old female with pathologically confirmed MCN with low-grade dysplasia.
A. Initial CT image shows 1.4 cm incidental unilocular CPL (arrow) in body of pancreas. B. Lesion (arrow) shows interval increase in size up to 2.2 cm on follow-up CT image obtained 11 months later. MCN = mucinous cystic neoplasm
|
 | Fig. 371-year-old male with pathologically confirmed IPMN with low-grade dysplasia.
A. Initial CT image shows 1.6 cm unilocular CPL (arrow), which was incidentally detected. B. Follow-up CT image obtained 6 months later demonstrates no interval change of pancreatic cyst (arrow). C. Follow-up CT image obtained 12 months later reveals interval increase in size of CPL up to 3.2 cm (arrow). CPL = cystic pancreatic lesion, IPMN = intraductal papillary mucinous neoplasm
|
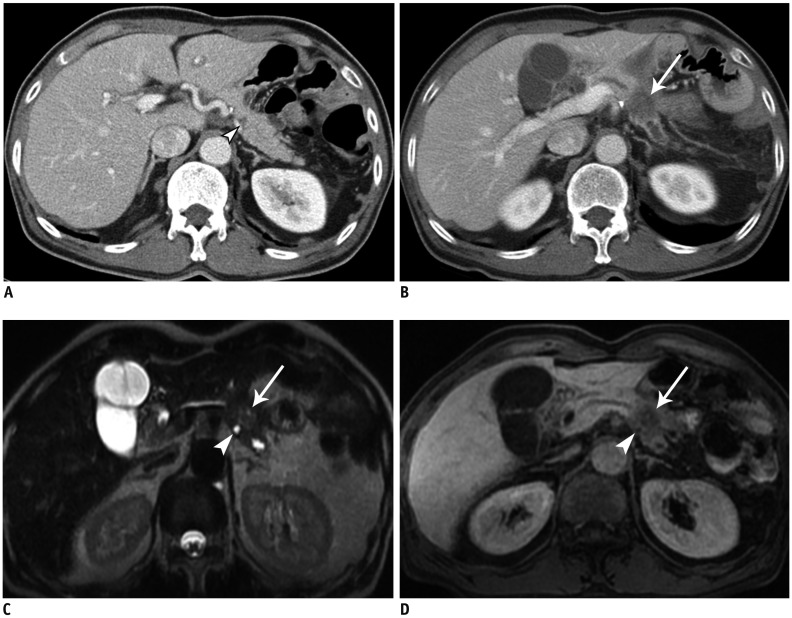 | Fig. 470-year-old male with pathologically confirmed ductal adenocarcinoma.
A. Initial CT image shows 0.4 cm unilocular cyst (arrowhead) in tail of pancreas. B. Follow-up CT image obtained 3 years later reveals newly developed, ill-defined low attenuated mass (arrow) in location of original cyst. C, D. MR images demonstrate no interval change of original cyst (arrowhead). Note that cyst (arrowhead) is located in vicinity of solid pancreatic mass (arrow).
|
Interval Change of CPLs
On a per-patient-based analysis, and of the 553 CPLs, 421 (76.1%) CPLs showed no increase, while 132 (23.9%) lesions showed an increase in size (Table 3). While the cyst size in the increase group at the last follow-up (mean: 1.90 ± 0.92 cm) was significantly greater than that in the no-increase group (mean: 1.08 ± 0.57 cm) (p < 0.001), the initial cyst size in the two groups did not differ significantly (mean: 1.22 ± 0.57 cm in the increase group and 1.18 ± 0.55 cm in the no-increase group, p = 0.535). The duration of follow-up was significantly longer in the increase group (p < 0.001). However, there were no significant differences between the two groups with respect to age, sex, the location and multiplicity of CPLs, and presence of dilatation of MPD at initial imaging (Table 3). At the last imaging, four (3.0%) of 132 CPLs in the increase group and one (0.2%) of 421 CPLs in the no-increase group were accompanied by dilatation of the MPD ≥ 5 mm that was not seen at the initial imaging. Further, two (1.5%) of 132 CPLs in the increase group and one (0.2%) of 421 CPLs in the no-increase group showed a thick enhancing wall and an enhancing solid component, respectively. There was a significant difference in the development of worrisome features and high risk stigmata between the two groups (p = 0.013).
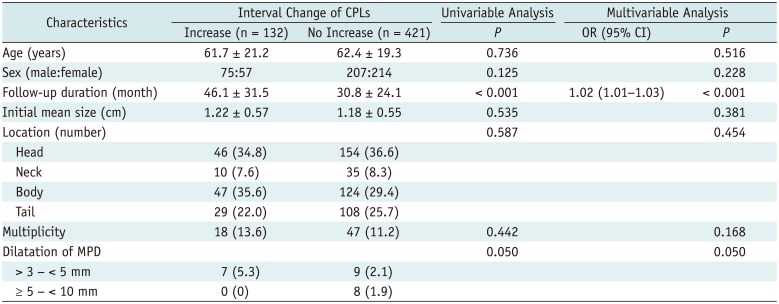
Table 3
Comparison between Increase and No Increase Groups
![]()
The no-increase group included CPLs that showed no change (n = 362), interval decrease (n = 46), and complete resolution (n = 13). Among the 421 CPLs in the no-increase group, nine were pathologically confirmed as benign lesions; four as pseudocysts, two as lymphoepithelial cysts, one as IPMN with low-grade dysplasia, one as a serous cystadenoma, and one as a simple serous cyst. In one case of 421 CPLs, a ductal adenocarcinoma was developed in the location of the original cyst. Of the 132 CPLs that showed an interval increase in cyst size, 120 (90.9%) lesions still had diameters less than 3 cm at the final follow-up studies. However, 12 (9.1%) CPLs increased to show diameters ≥ 3 cm (Table 4). There was a significant difference in the initial cyst size (mean: 1.13 ± 0.49 cm in < 3 cm group and 2.05 ± 0.73 cm in ≥ 3 cm group, p = 0.001) and growth rate (mean: 0.21 ± 0.27 mm/month in < 3 cm group and 0.67 ± 0.48 mm/month in ≥ 3 cm group, p < 0.001) between the two groups. While all 120 CPLs showing an interval increase to diameters < 3 cm were pathologically (n = 3) and radiologically (n = 117) regarded as benign, two (16.7%) of 12 CPLs with diameters ≥ 3 cm were pathologically confirmed to be malignant (mucinous cystadenocarcinoma and intraductal papillary mucinous carcinoma). One (8.3%) CPL was pathologically diagnosed as IPMN with low-grade dysplasia and the remaining nine (75%) of 12 CPLs were radiologically considered as benign. There were significant differences in the development of main duct size 5–9 mm (p = 0.013) and thickened enhancing cyst wall (p < 0.001) at final follow-up between the two groups.
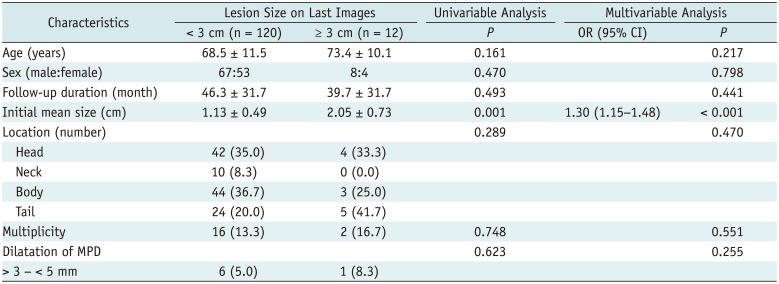
Table 4
Comparison between Two Subgroups (CPLs Size of < 3 cm vs. ≥ 3 cm at Last Follow-Up) in Increase Group
![]()
Among the various factors including age, sex, follow-up duration, initial size, lesion location, multiplicity of CPLs per patient, and dilatation of MPD at initial imaging, follow-up duration was a significant factor for an interval increase in size of CPLs on both univariable and multivariable analysis (odds ratio = 1.02; 95% confidence interval, 1.01–1.03; p < 0.001). In addition, multivariable logistic regression analysis revealed that initial cyst size was a significant independent factor of interval increase in size to diameters ≥ 3 cm in the increase group (odds ratio = 1.31; 95% confidence interval, 1.15–1.48; p < 0.001). According to the results from the multivariable analysis, ROC curve analysis was further performed to determine an optimal cut-off value for the initial cyst size to predict later cyst growth to ≥ 3 cm in diameter in the increase group. ROC curve analysis showed that a cut-off initial diameter of 1.5 cm (i.e., ≥ 1.5 cm as the test-positive criterion) achieved balanced sensitivity and specificity of 83% and 72%, respectively, for the prediction (area under the ROC curve, 0.82 [95% confidence interval, 0.79–0.85]). However, there were no significant predictors affecting the development of worrisome features and high-risk stigmata of malignancy during imaging surveillance.
Go to :
DISCUSSION
Cases of asymptomatic small CPLs would be less challenging to manage if a specific diagnosis of incidental CPLs could be clearly made. In a recent study, Lennon et al. (24) suggested a management strategy on the basis of the biology and malignant potential of each type of CPL via a multidisciplinary approach. However, despite advances in imaging techniques, small cystic lesions in the pancreas are still difficult to specifically characterize on CT or MR images due to similarities in appearance (25). Indeed, in cases of small unilocular CPLs, it often seems impossible or impractical to make a specific diagnosis because the lesions do not show any typical morphologic characteristics (1618). Previous studies have shown that the rate of correct histologic diagnosis of CPLs based on imaging findings was disappointing, with the accuracy being only about 50% (2627). Therefore, often, clinicians cannot confidently identify those requiring surgery among asymptomatic patients with incidental CPLs. One study revealed that the rate of recommending imaging for focal CPLs ranged from 10.5% to 79.6% among 22 radiologists (21). Further, even if imaging surveillance is deemed necessary for pancreatic cysts, several issues have yet to be clarified, including the optimal follow-up interval, the follow-up modality, stratification of cysts by size, and the point of discontinuing surveillance (28).
Technically, the vast majority of incidental pancreatic cystic lesions are small, and sub-centimeter cysts in the pancreas may be even interpreted as a part of the aging process (17). It is generally believed that unilocular CPLs without concerning features, such as thick enhancing wall, enhancing solid component, and mural nodule, can be confidently regarded as benign lesions, and would, therefore, not require close surveillance (913). In our study, pancreatic malignancy was noted only in 0.5% of the patients with unilocular CPLs over a mean follow-up period of 34.5 months, a finding consistent with previous studies (9111319).
In the past, post-inflammatory pseudocysts were believed to represent most of the cysts in the pancreas, irrespective of an antecedent history of pancreatitis (513). However, recent studies have suggested that neoplastic cystic lesions constitute a much larger proportion of incidental pancreatic cysts, with IPMNs being, by far, the most common (5121317). Thus, given the uncertainty of the natural history of IPMNs, it may be understandable that even small unilocular CPLs without concerning features could undergo malignant transformation, unlike the case with incidental cysts of the liver and kidney (2930313233). Further, many previous studies have indicated that a strong correlation exists between the presence of incidental pancreatic cysts and the subsequent development of ductal adenocarcinoma in any location within the pancreas (34353637). In our study, one patient with a 0.4 cm incidental pancreatic cyst went on to develop pancreatic ductal carcinoma three years later. Indeed, this example further complicates the issue of incidental CPLs. However, although the incidence of metachronous ductal adenocarcinoma has been reported to be as high as 8% in patients with IPMNs (38), the overall risk of malignancy in cases of incidental CPLs is considered to be very low (less than 0.5%) (519373940). Thus, anxiety among both patients and clinicians regarding the possibility of pancreatic carcinoma in the future does not seem to justify unnecessary and redundant imaging follow-ups to avoid missing a lethal pancreatic carcinoma.
In our retrospective study, 23.9% of incidentally detected small unilocular CPLs showed an interval increase over an average follow-up period of 34.5 months. However, 90.9% of the lesions showing growth still had a maximum diameter less than 3 cm at the final follow-up images, and tested negative for malignancy. In fact, many previous studies reported that even benign-looking CPLs showed an interval growth in size (5610193740414243); the percentage of CPLs that increased in size has been reported to range between 4% and 41%.
Several features may predict lesion growth during follow-up, including initial cyst size, tubular shape, septation, and dilated pancreatic duct (1040424344). Recently, a study by Yoen et al. (44) found that no cysts less than 1.5 cm without pancreatic duct change demonstrated a significant interval change within three years. In a study by Nougaret et al. (10), no lesion less than 2 cm showed a significant increase during the initial year of follow-up. In addition, those CPLs were not accompanied by any incidence of pancreatic cancer during a follow-up of 45 months. These results support the cessation of further follow-up for cysts with diameter < 2 cm that remain stable over a year or five years, as recommended by the American College of Radiology and American Gastroenterological Association, respectively (3945). However, given that the interval increase of CPLs may correlate with the duration of follow-up, as evidenced in our study, it remains uncertain whether imaging surveillance for stable CPLs (< 2 cm) in one or five years should be discontinued (17223746).
An increase in the size of an incidental CPL may imply an underlying malignant change (5). As per the European consensus statement (47), rapidly increasing size (diameter, > 2 mm/year) is included under the relative resection criteria of incidental asymptomatic pancreatic cysts on the basis of the findings of a study by Kang et al. (48). In our study, there was a significant correlation between an interval increase in cyst size and the development of concerning features. However, an increase in size alone may not be sufficient evidence to warrant surgical resection (45). Nevertheless, it seems at least reasonable that an incidental pancreatic cyst with interval growth warrants a watchful approach, even though such a lesion may not have other concerning features.
According to the IAP guidelines (22), cysts ≥ 3 cm are considered worrisome. Indeed, the relative risk of malignancy in these larger CPLs was reported to be higher than smaller ones (20). It is anticipated that cyst growth rate tends to increase in proportion to initial cyst size (44). Our study showed that initial cyst size was a significant independent factor of interval growth to diameters ≥ 3 cm in the increase group. Further, in our study, the initial size of 1.5 cm was an optimal cut-off point that would predict an interval size increase to greater than 3 cm. Therefore, CPLs of an initial size larger than 1.5 cm that show interval growth merit more attentive management than their smaller counterparts.
There are various imaging modalities available in the follow-up of patients with incidental CPLs. Ultrasound, MDCT and MR imaging are considered to be acceptable for imaging surveillance of CPLs (1149). Further, possible discrepancy in size or morphology of CPLs among various imaging tools has not been a vexing issue in the follow-up of incidental CPLs (11182122). However, in younger patients with CPLs of less than 1 cm, MR imaging is preferred owing to superior contrast resolution and no radiation exposure (113949). In our study, both MDCT and MR imaging were alternatively used at different times without a consistent protocol because our study was retrospective in nature.
Our study has several limitations. First, there may be selection bias. It is possible that the presence of small CPLs may not have been recorded in imaging reports. Second, pathologic confirmation of the diagnosis was not obtained for most patients. Third, all the patients underwent serial imaging without a consistent policy regarding selection of the imaging modality and follow-up interval. Thus, there may be a discrepancy between CT and MR imaging modalities with respect to the size and morphology of CPLs. Fourth, intra- and interobserver variability were not evaluated for measuring the size of CPLs. However, we assumed that interobserver agreement would be excellent for determining an interval increase of CPLs based on a previous study (37).
In conclusion, follow-up duration was independently associated with an interval increase of CPLs. Initial cyst size was an independent predictor of later increase in cyst size to diameters ≥ 3 cm in the increase group, and an initial cyst size ≥ 1.5 cm predicted such a growth with a sensitivity and specificity of 83% and 72%, respectively.
Go to :
 XML Download
XML Download