

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
It is desirable to minimize motion artifacts from cardiac pulsation and respiration on lung CT in free-breathing children. To achieve this, faster gantry rotation time (1), partial reconstruction (2), electrocardiography (ECG) triggering (134), respiratory triggering (5678), controlled ventilation (91011), and general anesthesia with intubation (12) have been used. The use of faster gantry rotation time and partial reconstruction is insufficient to suppress all motion artifacts on free-breathing lung CT (13). The respiratory-controlled techniques require intense patient cooperation or handling by skilled experts; hence, they are difficult to apply in free-breathing children (5789101112). In contrast, transthoracic impedance plethysmography-based respiratory triggering used in a study (6) may be applicable in free-breathing children. Retrospective respiratory gating has been used for radiotherapy (14), positron emission tomography (PET)/CT (15), and animal lung CT (1617). However, a high radiation dose of retrospective respiratory-gated lung CT hinders its clinical use in children.
Combined ECG and respiratory triggering or gating is used to suppress motion artifacts during free breathing in lung MRI (18), or cardiac PET (19). For free-breathing lung CT, a combined ECG and respiratory triggering system may also be used to minimize respiratory misregistration artifacts between adjacent imaging slabs, which is frequently seen with ECG-triggering alone; however, to our best knowledge, its technical feasibility has not been evaluated previously. Prospective ECG-triggered sequential scanning is already widely available in clinical CT scanners (2021) and additional prospective respiratory triggering, hence, needs to be incorporated for a combined triggering system. Therefore, the aim of this study was to describe our initial experience with combined ECG and respiratory triggering to reduce respiratory misregistration artifacts on lung CT in free-breathing children.
Go to : 
MATERIALS AND METHODS
Study Population
Our Institutional Review Board approved the retrospective study; and all CT examinations were clinically indicated. In our institution, prospectively ECG-triggered sequential scanning is used for unenhanced lung CT in free-breathing sedated children to eliminate cardiac motion artifacts and reduce respiratory motion artifacts on axial images. However, respiratory misregistration artifacts persist on coronal and sagittal reformatted images between adjacent sequential imaging slabs. In addition to axial images, coronal and sagittal reformatted images are included in routine image interpretation; hence, there is a need to reduce the motion artifacts on reformatted images. In our institution, lung CT protocol was gradually changed from prospectively ECG-triggered sequential scanning to combined prospectively ECG- and respiratory-triggered sequential scanning to reduce the respiratory misregistration artifacts on reformatted images. Combined prospectively ECG- and respiratory-triggered scan mode was installed in our institution in December 2008. Depending on the patients' condition and examination schedule, prospectively ECG-triggered sequential or spiral scan was used for unenhanced chest CT until March 2011. After March 2011, combined prospectively ECG- and respiratory-triggered scan was used as the primary scan mode for unenhanced chest CT in free-breathing children. In this study, we included pediatric patients who consecutively underwent free-breathing unenhanced lung CT using these two different CT scan protocols. Patients older than 15 years of age were excluded.
In 15 children (median age 19 months, range 6 months–8 years; 7 boys), prospectively ECG-triggered sequential lung CT using a first-generation dual-source scanner (SOMATOM Definition, Siemens Healthcare, Forchheim, Germany) was obtained during free breathing with and without additional respiratory triggering on two different days (median interval 3 months, range 12 days–1 year) between December 2008 and March 2011. Lung CT with ECG triggering was performed first in 10 patients and later in five patients. Disease categories of the patient population comprised congenital pulmonary airway malformation (n = 7), pneumonia (n = 2), Wilms tumor (n = 2), interstitial pneumonitis (n = 1), Langerhans cell histiocytosis (n = 1), repaired total anomalous pulmonary venous connection (n = 1), and pectus excavatum (n = 1). All children were sedated with oral chloral hydrate and intravenous administration of midazolam and/or ketamine was added if necessary. All children were younger than 5 years of age except for an 8-year-old boy who needed sedation for lung CT due to altered mentality caused by hemorrhagic brain lesions. In all children, general anesthesia, intubation, or controlled ventilation was not used.
CT Imaging
Dual-source prospective ECG-triggered sequential CT scan was performed at a gantry rotation time of 0.33 second (temporal resolution of 83 ms), 2 × 32 × 0.6 mm detector collimation with a z-flying focal spot, 0.75-mm slice width, 0.4-mm reconstruction interval, and a cycle time of 1.36 seconds for one acquisition and the subsequent table feed resulting in data acquisitions every 2 or 3 R-R intervals depending on heart rates. Sequential scanning was acquired at the end-systole of the R-R interval by using an absolute trigger delay (ms). For combined ECG and respiratory triggering, a pressure-sensing belt of a respiratory gating system (AZ-733V, Anzai Medical Co., Tokyo, Japan) was placed, usually in the upper abdomen, to obtain the respiratory signal (Fig. 1). Then, respiratory triggering was produced at either inspiration (n = 5) or expiration peak (n = 10) of the respiratory cycle determined by a pediatric radiologist based on the shape of respiratory curve in each child. Sequential scanning was acquired only when ECG triggering was synchronous with respiratory triggering through a prototype box that was not commercially available (Fig. 1). Average sequential scan rates per minute during free-breathing lung CT were recorded and compared between the two scan modes. Body size-adapted volume CT dose index derived from 16 cm-sized phantom of lung CT was determined individually by the cross-sectional area and the mean body density of each patient (22). To reduce image noise of unenhanced lung CT images, high tube voltage was used, e.g., 100 kVp in 14 patients, 120 kVp in one patient. Multiple sequential scans were obtained to cover the whole lung. The number of sequential scan slabs per lung CT was compared between ECG-triggered lung CT and combined ECG- and respiratory-triggered lung CT. CT dose estimates were calculated from dose length products derived from 16 cm-sized CT dose index phantom and age-, sex-, and tube voltage-specific conversion factors (23). The calculated effective dose was compared between ECG-triggered lung CT and combined ECG- and respiratory-triggered lung CT. For image interpretation, 3- to 5-mm thick axial, coronal, and sagittal CT images were reconstructed depending on scan length.
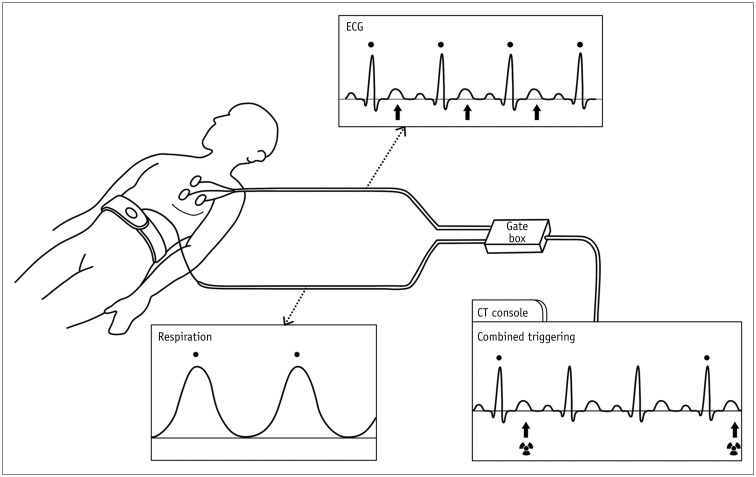 | Fig. 1Schematic drawing of combined ECG and respiratory triggering.From ECG leads, R wave (dot) is detected and end-systolic phase (arrows) is determined by trigger delay. Pressure-sensing belt is placed in upper abdomen to continuously monitor respiratory signal; in this case, respiratory triggering (dot) is produced at inspiration peak. When they occur concurrently, these two triggering signals can be passed through gate box to CT system. Combined ECG and respiratory triggering at R wave on ECG (dot) is displayed on CT console. From combined ECG and respiratory triggering, end-systolic sequential scanning is acquired every three R waves in this case. ECG = electrocardiography
|
Image Evaluation
The degree of respiratory misregistration artifacts in the entire thorax including the chest wall, the lung outline, and the diaphragm was measured by using calipers on coronal and sagittal lung CT images (Fig. 2) and subsequently, semi-quantitatively graded on a 4-point scale (grade 1, maximal distance of misalignment between adjacent imaging slabs due to respiratory misregistration < 2 mm; grade 2, 2–5 mm; grade 3, 5–10 mm; and grade 4, > 10 mm).
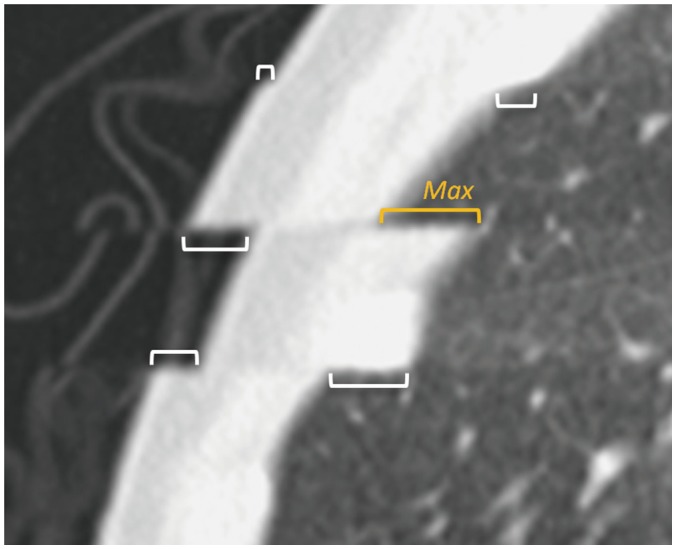 | Fig. 2Measurement of respiratory misregistration artifacts between imaging slabs on sagittal formatted lung CT image.Respiration misregistration occurred at three levels and degree of misregistration was measured in length (brackets) at six locations. Among them, maximal length (Max, orange yellow bracket) was used for semi-quantitative grading (grade 1, < 2 mm; grade 2, 2–5 mm; grade 3, 5–10 mm; and grade 4, > 10 mm).
|
Statistical Analysis
For statistical analysis, statistical software (SPSS version 20.0, IBM, Chicago, IL, USA) was used. Variables were expressed as the mean with standard deviation. Respiratory misregistration artifact grades were compared between ECG-triggered lung CT studies with and without respiratory triggering by using the Wilcoxon signed rank test. Continuous variables were compared between the two lung CT studies by using the paired t test. A p value < 0.05 was considered as statistically significant.
Go to :
RESULTS
Combined triggering was successfully applied to all children without technical failures. The results of comparisons between ECG-triggered lung CT studies with and without respiratory triggering are described in Table 1. Respiratory misregistration artifact grades on lung CT were significantly less with combined ECG and respiratory triggering (1.1 ± 0.4) than with ECG-triggering only (2.2 ± 1.0, p = 0.003) (Figs. 3,4). Average sequential scan rates per minute were significantly higher for ECG-triggered scan than for combined ECG- and respiratory-triggered scan (50.2 ± 6.8 vs. 35.3 ± 18.9, p = 0.01). The number of sequential scan slabs per lung CT was not significantly different between ECG triggering only (8.3 ± 1.9) and combined ECG and respiratory triggering (8.1 ± 1.8). The effective CT dose values showed no significant differences between ECG-triggered lung CT studies with and without respiratory triggering (1.0 ± 0.3 mSv vs. 1.1 ± 0.3 mSv, p = 0.2).

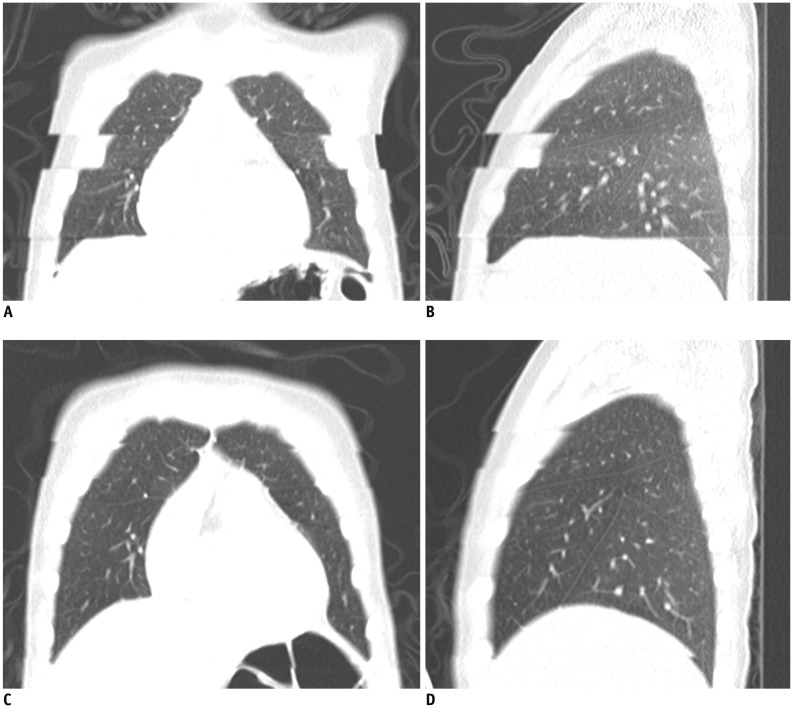 | Fig. 35-year-old boy with Langerhans cell histiocytosis.
A, B. Free-breathing coronal (A) and sagittal (B) ECG-triggered lung CT images acquired at end-systole show grade 4 respiratory misregistration artifacts. C, D. Respiratory misregistration artifacts grade was grade 1 on free-breathing coronal (C) and sagittal (D) lung CT images with combined ECG and respiratory triggering at end-systole and inspiration peak.
|
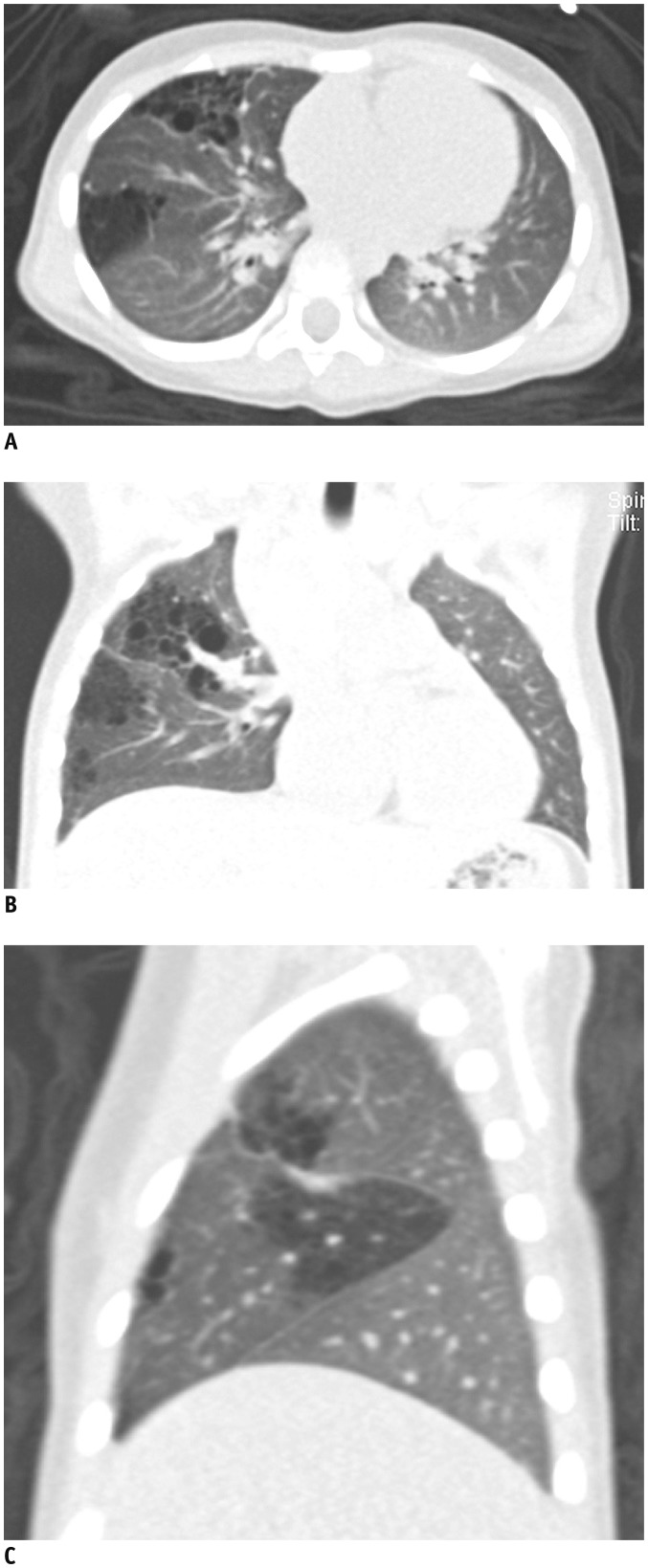 | Fig. 42-year-old girl with multifocal congenital pulmonary airway malformation.Free-breathing axial (A), coronal (B), and sagittal (C) lung CT images with combined ECG and respiratory triggering at end-systole and expiration peak demonstrate excellent normal anatomic and pathologic details without any motion artifacts.
|
Table 1
Comparisons of Variables between ECG-Triggered Lung CT with and without Respiratory Triggering
![]()
Go to :
DISCUSSION
Image quality of lung CT in free-breathing children has improved mainly due to more rapid acquisition of CT data. However, residual motion-related artifacts need to be reduced to achieve comparable image quality on free-breathing lung CT as that on breath-hold lung CT. ECG-triggered sequential scanning is often used to reduce cardiac pulsation artifacts on lung CT, but respiratory misregistration artifacts are particularly pronounced along the z-axis in free-breathing children. In this study, we demonstrated the technical feasibility of combined ECG- and respiratory-triggered lung CT to minimize not only cardiac pulsation artifacts, but also respiratory misregistration artifacts in free-breathing children without any interventions to patients' airways, such as general anesthesia with intubation and controlled ventilation. In the 1990s, the first respiratory-triggered lung CT using a spirometer was reported in adult patients (57). However, it has not been widely used since the spirometer is not patient-friendly. Recently, Lell et al. (24) reported that free-breathing respiratory-triggered high-pitch dual-source chest spiral CT, using the same respiratory gating system as in this study, could minimize motion artifacts in adult patients, as compared with conventional inspiratory breath-hold spiral chest CT. However, the sole effect of respiratory triggering on reduction of motion artifacts could not be determined, because high-pitch dual-source spiral scan itself can considerably reduce motion artifacts due to its very fast scan time. To our best knowledge, combined ECG- and respiratory-triggered lung CT has not been previously evaluated in free-breathing patients.
In the combined ECG- and respiratory-triggered lung CT, sequential scan rates were approximately 1.4-times slower than those in ECG-triggered lung CT, which prolonged the total scan time of combined-triggered scan. However, this prolongation may not affect the image quality of lung CT without intravenous contrast agent. In contrast, a modified intravenous contrast injection protocol to lengthen peak enhancement period is necessary for contrast-enhanced chest or cardiac CT with combined ECG and respiratory triggering in free-breathing patients. This can be achieved by using multiphase decremental injection rates of contrast agent (2526).
In addition to improved anatomic details, the combined ECG and respiratory triggering used in this study has potential for functional and quantitative lung evaluations, such as air trapping evaluation and lung volumetry, in free-breathing children because motion-free lung CT image data can be obtained at both end-inspiration and end-expiration with three-dimensional non-rigid image registration (2728). The combined ECG and respiratory triggering can also be used for uncooperative, free-breathing adults with altered mental state or respiratory difficulty. The respiratory gating system used in this study has a technical limitation, since respiratory triggering is not possible when the respiratory rate is higher than 50/min or breathing is substantially irregular.
This study has several limitations. First, the study population was small. However, the results of paired comparisons to evaluate the technical feasibility in this retrospective study may not be different even by increasing the number of patients included. Second, underlying diseases of the study population were heterogeneous. However, this was a technical feasibility study focusing on motion artifacts rather than clinical diseases. Third, there was a median 3-months-time interval between the two lung CT studies in the same patient. This was also attributed to the retrospective nature using the clinically indicated CT studies.
In conclusion, combined ECG and respiratory triggering can minimize respiratory misregistration artifacts between imaging slabs on lung CT in free-breathing children. This new CT imaging technique may eliminate the need for more invasive procedures, such as general anesthesia with intubation and controlled ventilation, to produce a motion-free effect on free-breathing lung CT.
Go to :
 XML Download
XML Download