

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Focal epilepsy accounts for more than 50% of childhood-onset epilepsy cases (1). Identification of potential structural lesions of focal epilepsy is crucial prior to consideration of surgery (2). The superiority of surgical over medical therapy in patients with intractable epilepsy has been verified (34).
The role of neuroimaging in localizing epileptogenic foci is well-established, and children with focal epilepsy should undergo brain magnetic resonance imaging (MRI), excepting those with benign idiopathic focal epilepsy (5). Approximately half of the imaging studies in children with new-onset focal epilepsy demonstrate abnormal results and 15–20% of the studies provide information useful for lateralizing focal epilepsy (56). Malformation of cortical development (MCD) and hippocampal sclerosis are the commonly encountered focal brain pathologies on surgical series in patients with MRI-negative epilepsy (2). Moreover, 40–80% of patients with MRI-negative epilepsy are likely to be seizure-free (78); whereas MRI-positive patients have a greater than two-fold surgical-success rate to achieve freedom from seizures, as compared to MRI-negative patients (9).
Several studies have proposed the significance of repeat MRI in patients with focal epilepsy (101112). The diagnostic yield of MRI in patients with epilepsy strongly depends on the expertise of the reader and various technical considerations. However, in children with focal epilepsy, the degree of myelination is an additional factor to be considered (1314151617). In the present study, we focused on the value of advanced imaging techniques and chronological changes according to myelination in children with focal epilepsy.
The purpose of our study was to evaluate the value of repeat brain MRI to identify potential epileptogenic lesions in children with initial MRI-negative focal epilepsy.
Go to : 
MATERIALS AND METHODS
Study Population
Our Institutional Review Board approved this retrospective study, and the requirement for informed consent was waived. The patients' information was anonymized and de-identified prior to analysis.
We searched the records of children with seizures who had undergone at least two sets of brain MRI (initial and at least one follow-up MRI) between January 1997 and March 2012. The search yielded 890 patients who were under the age of 18 years at the time of the initial MRI. The inclusion criterion for the study was children with focal epilepsy as a reason for the initial brain MRI that showed negative findings (either normal or absence of focal abnormality). One of the authors who had 12 years of experience in pediatric neurology made the diagnosis of focal epilepsy based on seizure semiology and electroencephalogram (EEG) criteria. The classification of epilepsy was based on the Commission of the International League Against Epilepsy (2010) guideline (18). The exclusion criteria were: 1) children with initial MRI reports as positive (either minor or major abnormalities, regardless to the association of seizure; n = 500), 2) children with generalized epilepsy (n = 114), 3) children with non-epileptic events such as psychogenic seizure (n = 10), 4) children with epilepsy wherein focal or generalized seizure was ruled out (n = 6), and 5) children with situation-related seizures (e.g., febrile convulsions or seizures due to an acute metabolic or toxic event; n = 3). Finally, a total of 257 patients were included for analyses. Their mean age at the time of initial MR examination was 6.6 years (range, 1 month–18 years). Of the 257 patients, 148 were boys (mean age, 6.6 years; range, 1 month–18 years) and 109 were girls (mean age, 6.7 years; range, 1 month–16 years). The case accrual process is summarized in Figure 1.

The reasons for repeat MRI included intractable epilepsy (> 1 month duration or > 2 antiepileptic drugs administered) in 43% (110/257) of the patients, changed seizure semiology in 7% (19/257), recently developed recurrent seizure in 9% (22/257), persistent seizure lasting more than 2 years in 23% (61/257), other causes such as headache or developmental delay in 2% (5/257), and uncertain causes in 16% (40/257).
MRI Technique
In our hospital, MRI was performed using a 1.5T (Signa Advantage Horizon, GE Medical Systems, Milwaukee, WI, USA) with quadrature head coils from 1997 to 2010 and 3T (Achieva, Philips Healthcare, Best, the Netherlands) from 2006 to 2012 with eight-channel phased-array head coils. This study also included MRI examinations conducted by outside hospitals using 0.3T to 3T systems from various vendors (Table 1).
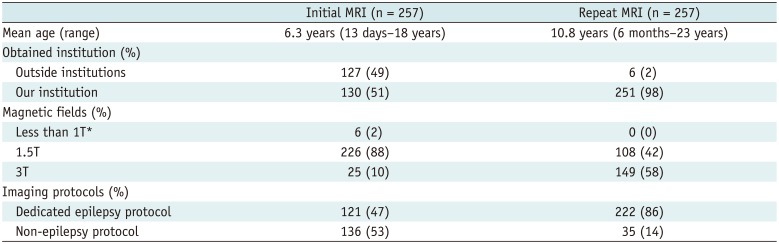
Table 1
Characteristics of Initial and Repeat MR Examinations
![]()
The imaging protocols were classified into dedicated epilepsy protocol and non-epilepsy protocol. Dedicated epilepsy protocol comprised at least one coronal acquisition for T2-weighted images and/or fluid-attenuated inversion recovery (FLAIR) and a high resolution, 3-dimensional (3D) T1-weighted gradient echo volume acquisition. Non-epilepsy protocol included at least three axial or coronal acquisitions of T2-weighted, T1-weighted, and FLAIR images. Our institutional epilepsy protocol consisted of T1-weighted magnetization-prepared rapid acquisition with gradient echo imaging (repetition time/echo time = 9–25/4–5 ms, section thickness = 1–1.6 mm, field of view = 220–240 mm, matrix = 240–304 × 240–304), axial and oblique coronal T2-weighted fast inversion recovery for myelin suppression sequences (4405–6701/20–100 ms, 3–4 mm, 180–200 mm, 336 × 252–256), axial and oblique coronal FLAIR (11000/120–125 ms, 3–5 mm, 180–220 mm, 256–372 × 253–279), and axial gradient echo T2-weighted images (622–626/11 ms, 5 mm, 180–210 mm, 256 × 241) for the 3T MR system; and 3D T1-weighted spoiled gradient-recalled acquisition (14–33/3–7 ms, 1.5–1.6 mm, 200–220 mm, 256 × 192), axial and oblique coronal FLAIR (10002–13000/20–133 ms, 4–5 mm, 180–240 mm, 256 × 192–224), axial and oblique coronal fast spin echo T2-weighted images (3000–5800/76–105 ms, 3–5 mm, 180–240 mm, 320–256 × 192–256), and axial gradient echo T2-weighted images (283–450/15–20 ms, 5 mm, 210–240 mm, 256 × 224–256) for the 1.5T MR system. Gadolinium contrast was used if there were concerns about tumor, vascular malformation, infection, and inflammation.
Image Analysis
Two pediatric radiologists (with 21 years and 6 years of experience in pediatric neuroimaging, respectively) independently reviewed the initial as well as repeat MRI images and consensually resolved all disagreements. Readers were informed of the seizure semiology and EEG results to facilitate MRI localization but were blinded to other clinical data.
At the first reading session, the readers reassessed all the repeat MR images and classified them as either negative or positive based on the presence of abnormalities. Positive results of repeat MRI were assessed for the presence of potential epileptogenic lesions including MCD and hippocampal sclerosis. Features not generally considered as epileptogenic were regarded as other abnormalities (19). At the second reading session, the readers re-evaluated the initial MRI to assess whether newly diagnosed lesions at repeat MRI were retrospectively detectable on the initial MRI. Initial MRI with negative reports were categorized as either initial true-negative or initial false-negative. In cases of newly diagnosed potential epileptogenic lesions, the contributing factors for new diagnoses were analyzed for lesions that had been overlooked initially; and the factors were classified as imaging factors or lesion factors. Imaging factors were technical differences between the scans, including MRI systems with different magnetic field and/or imaging protocols. Lesion factors were considered when there were changes in size, extent, or signal intensity of the lesion itself.
Malformation of cortical development included a wide disease spectrum based on a prior classification (20); wherein, focal cortical dysplasia was determined when at least one of the cardinal MRI findings was present: 1) cortical thickening or thinning, 2) abnormal gyration, 3) blurring of gray and white matter junction, 4) cortical and/or subcortical signal changes, and 5) transmantle sign (defined as a subcortical white matter signal change, tapering toward the ventricle). Imaging diagnosis of hippocampal sclerosis was made in cases with concomitant hippocampal volume loss and increased T2 and FLAIR signal intensity (21). Increased T2 and FLAIR signal intensity alone without volume loss of the hippocampus was regarded as other abnormality.
Go to :
RESULTS
Initial and Repeat MRI Examinations
A total of 257 patients underwent 594 brain MRI examinations as both initial work-up and subsequent follow-up for focal epilepsy. The mean number of MRI acquisitions per patient was 2.3 (range, 2–7). The information of both initial and repeat MRI is summarized in Table 1. The mean interval between scans was 4 years (range, 2 days–14 years). Of the total cohort, 16% of patients (41/257) underwent initial MRI at under 2 years of age.
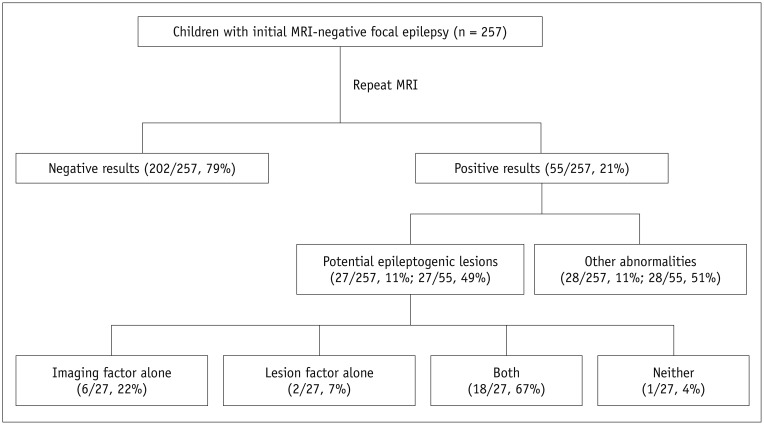
The results of repeat MRI are summarized in Figure 2. Of repeat MR images from 257 children with initial MRI-negative focal epilepsy, positive results at repeat MRI were 21% (55/257), whereas negative results were 79% (202/257). Re-evaluation of initial MR images indicated that the incidence of true-negative initial MRI was 91% (233/257), whereas the incidence of false-negative initial MRI was 9% (24/257). Of the 233 patients with true-negative initial MRI, 31 patients (mean age, 5.3 years; range, 1 month–14 years) showed positive results at repeat MRI (potential epileptogenic lesions in 6 and other abnormalities in 25). Of the 24 patients with false negative initial MRI (mean age, 4.6 years; range, 1 month–13 years), 21 showed potential epileptogenic lesions and three showed other abnormalities.
Potential Epileptogenic Lesions
Potential epileptogenic lesions were detected in 11% of all patients (27/257), which comprised 49% (27/55) of the patients with subsequent positive MRI. Among these 27, 17 (63%) were diagnosed with MCD, and 10 (37%) exhibited hippocampal sclerosis.
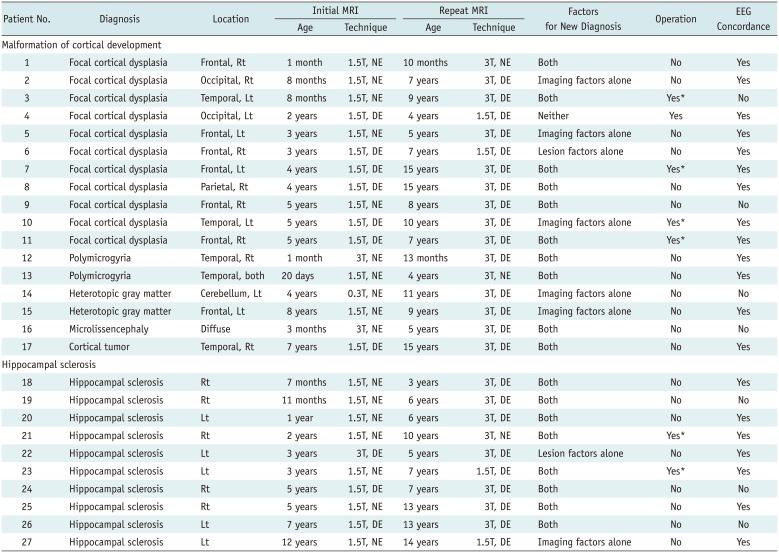
Newly diagnosed MCD included focal cortical dysplasia (n = 11), polymicrogyria (n = 2), heterotopic gray matter (n = 2), microlissencephaly (n = 1), and cortical tumor (n = 1) (Table 2). Focal cortical dysplasia was localized to the frontal (n = 6), temporal (n = 2), occipital (n = 2), and parietal lobe (n = 1); involving the right (n = 6) or left (n = 5) hemispheres. Among the 17 patients diagnosed with MCD, only four patients had true-negative initial MRI on re-evaluation; whereas, the remaining 13 patients were retrospectively read as possible MCD at initial MRI that was supported by repeat MRI. Contributing factors for newly diagnosed MCD were imaging factors alone in five patients (Fig. 3), lesion factors alone in one patient (Fig. 4), both factors in 10 patients (Figs. 5, 6), and neither in one patient. Imaging factors included either higher magnetic field strength (n = 13) or dedicated epilepsy protocols (n = 8). Lesion factors included more apparent cortical thickening (n = 6, cases 1, 3, 8, 12, 13, and 16), apparent abnormal gyration (n = 3, cases 1, 3, and 16), alterations in the signal intensity of subcortical white matter (n = 5, cases 3, 6, 7, 9, and 11), apparent blurring of gray and white matter junction (n = 4, cases 1, 3, 7, and 8), and/or increased extent of the lesion with enhancement (n = 1, case 17). Of the 17 patients with newly diagnosed MCD, six had initial MRI performed at less than 1-year of age (mean 3.6 months, range 20 days–8 months) and all except one had lesion factors (Fig. 5). In addition, 11 patients had received their initial MRI at more than 2-years of age (mean 4.5 years, range 2–7 years), and showed either imaging factors (n = 9) or lesion factors (n = 6) (Fig. 6). The mean interval between initial and repeat MRI was 5 years (range 1–11 years; median 4 years). The epileptogenic activity in the EEG was concordant with the location of the newly diagnosed MCD on repeat MRI in 13 of 17 patients (76%).
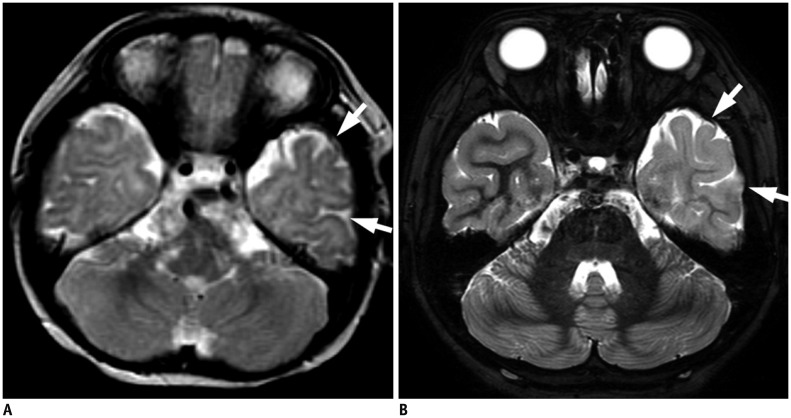
 | Fig. 3Imaging factors alone in case 14 with cerebellar heterotopia.
A. Axial proton density T2-weighted initial MR image (0.3T, non-epilepsy protocol) obtained at age of 4 years poorly demonstrates subtle iso-intense lesion (arrow) compared to cerebellar cortex in left cerebellum. B. Axial T2-weighted fast inversion recovery for myelin suppression repeat MR image (3T, dedicated epilepsy protocol) obtained at age of 11 years clearly shows small nodule (arrow), matching with area indicated in (A), with same signal intensity of cerebellar cortex (iso-intense on T1-weighted MR images, image not shown). This lesion is unchanged on second follow-up MRI obtained 15 months later (image not shown).
|
 | Fig. 4Lesion factors alone in case 6 with focal cortical dysplasia.
A. Axial T2-weighted initial MR image (1.5T, dedicated epilepsy protocol) obtained at age of 3 years reveals focal abnormal gyration in right frontal lobe (arrow). B. Axial T2-weighted repeat MR image (1.5T, dedicated epilepsy protocol) obtained at age of 7 years shows hyperintense cortical thickening and subcortical white matter hyperintensity in right frontal lobe (arrow).
|
 | Fig. 5Both imaging and lesion factors in case 3 with focal cortical dysplasia.
A. Axial T2-weighted initial MR image (1.5T, non-epilepsy protocol) obtained at age of 8 months shows normal cortical thickness in left temporal lobe (arrows). B. Axial FIRMS repeat MR image (3T, dedicated epilepsy protocol) obtained at age of 9 years demonstrates cortical thickening (arrows), matching with area indicated in (A). Patient underwent temporal lobe resection and pathologic reports revealed focal cortical dysplasia type Ia. FIRMS = fast inversion recovery for myelin suppression
|
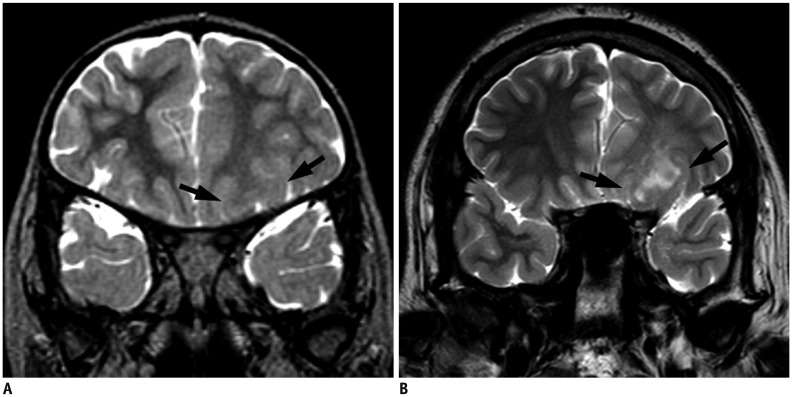 | Fig. 6Both imaging and lesion factors in case 7 with focal cortical dysplasia.
A. Oblique coronal T2-weighted initial MR image (1.5T, dedicated epilepsy protocol) obtained at age of 4 years after completion of brain myelination shows blurring of gray and white matter junction, thick cortex, and subtle increased underlying white matter signal intensity in left frontal lobe (arrows). B. Oblique coronal T2-weighted repeat MR image (3T, dedicated epilepsy protocol) obtained at age of 15 years demonstrates discernable subcortical white matter hyperintensity in same area (arrows). Patient underwent surgical resection and pathologic reports revealed focal cortical dysplasia type IIb.
|
Table 2
Potential Epileptogenic Lesions at Repeat MRI in Children with Initial MRI-Negative Focal Epilepsy
![]()
Ten patients were diagnosed with hippocampal sclerosis at repeat MRI. Mean age at initial MRI was 3.8 years (range, 7 months–12 years) and at repeat MRI, 8.4 years (range, 3–14 years). The mean interval between the initial and repeat MRI was 4 years (range, 2–8 years; median 3.5 years). All patients had unilateral hippocampal sclerosis with a right-to-left ratio of 5:5. Two patients had true-negative initial MRI and eight had false-negative initial MRI including four each with increased hippocampal signal intensity, and both increased signal intensity and volume loss of the hippocampus at initial MRI. Contributing factors for newly diagnosed hippocampal sclerosis were considered as imaging factors alone (n = 1), lesion factors alone (n = 1), and both factors (n = 8). Imaging factors included either higher magnetic field strength (n = 7) or dedicated epilepsy protocols (n = 6). Lesion factors included either progressive hippocampal volume loss (n = 9, cases 18–26) or alteration of hippocampal signal change (n = 6, cases 18–23).
Based on the new relevant diagnoses of potential epileptogenic lesions, the patients' management included surgical resection (5 cases of focal cortical dysplasia and 2 cases of hippocampal sclerosis) in seven of 55 patients (13%), representing 3% of the total patients; and all except one (86%, 6/7) achieved seizure-free status following surgery.
Other Abnormalities
Other abnormalities were detected in 28 patients (11% of all patients; 51% of 55 patients with positive repeat MRI), including diffuse cortical atrophy in 18% (5/28), white matter abnormality in 46% (13/28), ventricle abnormality (ventriculomegaly) in 7% (2/28), basal ganglia abnormality (T1 hyperintensity in the bilateral globus pallidus and right caudate nucleus) in 4% (1/28), hippocampal abnormality (signal alterations without volume loss) in 11% (3/28), and gliosis and/or encephalomalacia in 14% (4/28). White matter abnormality consisted of punctate hyperintense foci (n = 9) and small patchy hyperintense areas (n = 4) on T2-weighted images. Of the 28 patients with other abnormalities, 25 showed true-negative initial MRI and three had false-negative initial MRI. In cases with false-negative initial MRI, repeat MRI revealed increased signal intensity in the peritrigonal area in one case, and increased hippocampal signal intensity in the remaining cases; contributing factors included imaging factor in one patient and both imaging and lesion factors in two patients.
Go to :
DISCUSSION
Repeat MRI in children with initial MRI-negative focal epilepsy revealed positive results in 21% of cases (55/257), which led to identification of new potential epileptogenic lesions in 11% of cases (27/257). These data exceeded the result of Winston et al. (10), who found new diagnoses in 12% (97/804) and new potential epileptogenic lesions in 5% (37/804) of 3T MRI in focal epilepsy among all ages. In the present study, new relevant diagnoses affected patients' management in 3% (7/257) of total patients, resulting in seizure-free status following surgery in 86% (6/7) of patients with new epileptogenic lesions. Focal cortical dysplasia and hippocampal sclerosis, in order, were the most common new potential epileptogenic lesions.
The reclassification of a patient with focal epilepsy from negative MRI to positive MRI may depend on the quality of the applied MRI. In our study, 93% of new relevant diagnoses were detected by imaging factors including a higher magnetic field MRI system with phased array coils and/or dedicated epilepsy protocols. Similarly, increased field strength of 3T MRI detected new lesions in 12–65% of patients with a previously negative 1.5T MRI (1012). A 3T MRI with phased array coils can result in an eight-fold increase in the signal-to-noise ratio (SNR) than that of 1.5T MRI with quadrature head coils. Improved SNR allows increased spatial resolution and improved contrast-to-noise ratio (1222). In addition, dedicated epilepsy protocols revealed relevant pathologies in 85–94% of patients undergoing evaluation for epilepsy surgery who had shown normal results on standard brain MRI (2324).
While imaging factor may account for improved lesion visibility, imaging factor alone was not sufficient to explain the variability of lesion conspicuity on repeat MRI. Our results revealed that 11 cases of MCD had lesion factors, indicative of possible changes in the appearance of MCD on MRI over time despite the congenital nature of MCD. These chronological changes in MCD on MRI can include changes in the appearance and even disappearance of lesions (1314151617). Several studies of histopathologically confirmed focal cortical dysplasia have documented newly appeared (n = 6) or more apparent (n = 1) lesions in seven patients who had follow-up MRI at older ages (131416). All except one had undergone initial MRI at less than 1-year of age. Conversely, disappearance of focal cortical dysplasia on repeat MRI has also been reported (17). In terms of polymicrogyria, longitudinal cortical change has been reported in a 3-month-old patient (15). Follow-up MRI at 2-years of age indicated that the cortical features had changed from small and fine with normal thickness to bumpy with abnormal thickness. Such changes in the appearance of MCD on MRI may be strongly influenced by myelination of subcortical and intracortical fibers (1314151617). Axonal myelination causes T1 and T2 shortening, which occurs at various rates and times, and is essentially completed by 2-years of age (25). T2 shortening is possibly associated with chemical maturation of the myelin, which leads to decreasing axonal or extracellular water. In myelin, the interaction of cholesterol and glycolipids with water correlates with T1 shortening in the developing white matter (25). During this period, the variability of MRI contrast between gray and white matter can cause changes in the appearance of MCD on MRI. Therefore, our study supported that in cases with normal findings on initial MRI performed before 2-years of age and persistent focal epilepsy, MRI should be repeated at a stage when myelination is expected to have advanced.
Our study included six patients who had MCD with lesion factors, wherein initial MRI was conducted at over 2-years of age, when myelination was complete; among them, one patient showed no technical difference between the MRI scans. Other authors have reported the case of a boy with negative MRI findings for focal cortical dysplasia at the age of 2.5 years, which became discernible at the age of 6 years (13); in addition, the MRI changes were possibly due to cortical changes, such as disorganized cortical lamination and dysplastic neurons, based on the histopathologic findings. Besides these cortical changes, subcortical white matter changes, including gliosis, hypomyelination, or disorganized heterotopic white matter neurons, may progress over time, as supported by our findings of changed signal intensity in subcortical white matter after complete myelination in four patients with focal cortical dysplasia. Although the exact mechanism is uncertain, it is important to recognize that the appearance of MCD on MRI may change with increasing age, even after myelination is complete. Thus, repeat imaging may be necessary to lateralizing focal epilepsy in older children.
Hippocampal sclerosis appears to be a progressive disorder. Hippocampal volume ipsilateral to the seizure focus correlates with the duration of epilepsy and/or earlier age of onset, and may be related to progressive neuronal damage over time (2627). Although the pathogenesis of hippocampal sclerosis remains unclear, febrile status epilepticus, genetics, and viral infection may be associated with hippocampal injury (4). More than 80% cases of hippocampal sclerosis manifest before the age of 16 years, but cases have been reported in infancy (28).
Our study has the following limitations. First, uniformity of MRI techniques could not be maintained due to the retrospective nature of data collection over a 15-year period; therefore, we could not separate each effect of the 3T MRI system, phased array coil, and dedicated epilepsy protocol. Second, histopathologic diagnosis was unclear for most of the potential epileptogenic lesions. Third, the unblinded review of seizure semiology may have resulted in increased rates of false negatives or false positives, because lesions remote from the area of EEG-based epileptogenic activity may have been overlooked, and lesions in the lobe of epileptogenic activity may have been over-interpreted. Fourth, our results did not address the optimal timing of repeat MRI, particularly in children over 2 years of age. Fifth, we did not evaluate the relationship between potential epileptogenic lesions on repeat MRI and seizure semiology including frequency or duration. Further studies are needed to address these issues.
In conclusion, repeat MRI with enhanced techniques identified initially overlooked epileptogenic lesions in children with focal epilepsy. In addition, changes in appearance of potential epileptogenic lesions on MRI emphasized the importance of repeat MRI in children with negative initial MRI. If the initial MRI performed before the age of 2 years is negative, MRI should be repeated after completion of 2-years of age, when brain myelination is complete. Furthermore, in children over 2-years of age, repeat MRI is necessary in cases of persistent focal epilepsy with negative initial MRI.
Go to :
 XML Download
XML Download