

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Renal cell carcinoma (RCC) accounts for 85 to 90% of kidney malignancies (1), and the disease has a highly variable clinical course ranging from several months to decades. RCC recurrence can occur several years or even decades after curative nephrectomy, and more than 50% of patients who undergo primary tumor resection have a remote recurrence (2). Excision of recurrent and metastatic lesions leads to longer survival (345) while improvements in patient care and new treatment modalities, such as administering anti-angiogenic agents, may also improve the overall survival benefits by reducing pharmacological toxicity and improving quality of life (36). Although RCC can metastasize to any site in the body, clinically evident gastrointestinal (GI) involvement is extremely rare (78), likely leading to its underdiagnosis due to its low prevalence. In addition, such cases do not receive much clinical attention since they are frequently regarded as an aspect of generalized metastatic disease.
Most RCCs are hypervascular, with the clear cell type as the most common histologic type (9), and their metastatic lesions also tend to be hypervascular. If RCC metastasizes to the GI tract, the lesions may cause GI bleeding due to the abundant vascularity. In addition, unlike metastasis to solid organs, metastatic GI lesions can lead to serious bowel complications due to their mobility, including obstruction or intussusception. These possibilities reinforce the importance of meticulous examination for small metastatic lesions involving the GI tract in patients who have undergone curative RCC resection to ensure early diagnosis and appropriate treatment.
To date, few case reports have described patients with RCC metastasis to the GI tract (7101112131415161718192021), and to the best of our knowledge, the CT features of RCC that manifest in the GI tract have not been well analyzed. CT plays a pivotal role in diagnosing RCC and in oncologic imaging of the GI tract, so characterization of the CT findings is essential to evaluate GI involvement in patients with recurrent RCC. The purpose of present study was thus to retrospectively evaluate the CT features of GI-involved recurrent RCC and correlate these characteristics with the clinical and pathologic features of these patients.
Go to : 
MATERIALS AND METHODS
Study Group
This retrospective study was approved by the Institutional Review Board of our institution, and the requirement for informed consent was waived. Medical records were searched through a computerized search to identify patients with pathologically-proven GI involvement of RCC from January 1994 to December 2014. Of the 3637 patients diagnosed with RCC at our institution during this period, 26 patients with 30 GI lesions were identified. No patient had synchronous GI metastasis at the time of the RCC diagnosis, and eleven patients were excluded from the analysis. Six of 11 patients, each with a single GI lesion, were excluded because the primary RCC had directly invaded the GI tract; five patients, each with a single lesion, were excluded due to poor CT image quality. Thus, this study included 15 patients (11 men and 4 women; mean age, 61.1 years; range, 45–80 years) with 19 GI lesions. Specimens for pathologic diagnosis were obtained through a surgical resection of 15 GI lesions and an endoscopic biopsy of four GI lesions. The reasons for laparotomy were endoscopically uncontrollable GI bleeding (n = 9), intussusception (n = 4), GI obstruction (n = 1), and clinical necessity of excisional biopsy for diagnostic purposes (n = 1).
Review of Medical Records
One radiologist reviewed the electronic medical records and recorded medical information for each of the 15 patients. The data recorded included patient age, sex, clinical presentation, hemoglobin concentration, TNM stage with histologic type and grade of RCC, concomitant distant metastasis, interval between RCC diagnosis and detection of GI involvement, treatment after primary tumor resection, exact treatment modality, and patient outcomes.
CT Scanning
All included patients underwent contrast-enhanced CT scans. Several CT scanners were used during the 20-year follow-up period, including the Sensation 16, Somatom Definition, Somatom Definition flash, and Somatom Definition AS + scanners (Siemens Medical Systems, Erlangen, Germany) and the LightSpeed 16, LightSpeed Plus, and LightSpeed VCT scanners (GE Healthcare, Milwaukee, WI, USA). As a result of the long follow-up period, the CT protocols varied. For scans of the abdomen and pelvis CT (n = 12), intravenous contrast medium (120–150 mL of 300–370 mgI/mL non-ionic contrast [iopromide, Ultravist 300 or Ultravist 370; Bayer Healthcare, Berlin, Germany]) was administered at a rate of 2–3 mL/sec using an automatic power injector through an 18-gauge angiographic catheter into an antecubital vein. With the patient in the supine position, venous-phase images were obtained from the dome of the diaphragm to the pubic symphysis 70–80 seconds after a contrast medium injection.
The dynamic kidney CT (n = 2) images were obtained during unenhanced, corticomedullary, parenchymal, and early excretory phases. The time for the corticomedullary phase scan was determined using an automatic bolus triggering technique: scanning was started when the CT number of an region of interest in the upper abdominal aorta reached 100 Hounsfield unit (HU). The scan delays for the parenchymal and early excretory phases were 90 seconds and 180–240 seconds, respectively.
The dynamic pancreas CT (n = 1) images were obtained during the non-enhanced, arterial, and portal phases. The arterial phase images were obtained using a bolus tracking technique with a trigger enhancement threshold of 100 HU at the upper abdominal aorta. After the threshold was reached, a diagnostic delay time of 10 seconds was used for the arterial phase. The portal-phase images were obtained 72 seconds after contrast injection.
Beginning in 2008, coronal reformations of the venous phase were routinely performed for all CT scans at our hospital. Positive oral contrast medium consisting of a barium sulfate solution (1.5 Easy CT Solution; Taejoon Pharmaceutical, Seoul, Korea) was administered to cancer patients for opacification of the small intestine. The use of a positive oral contrast agent was prohibited if bowel obstruction, perforation, bleeding, inflammatory bowel disease, or biliary stone disease was suspected. Beginning in 2013, patients were instructed to drink water instead of barium sulfate as a neutral oral contrast.
The scan parameters included beam collimation at 16 × 0.75 mm, 32 × 0.6 mm, or 64 × 0.6 mm; beam pitch at 0.75–1.5; gantry rotation time of 0.5–0.8 second; field of view to fit; 120 kVp; automated dose reduction system (CARE Dose 4D; Siemens Medical Solutions, Erlangen, Germany) with tube current set to 170–250 mAs. The images were reconstructed in the axial and coronal planes, ranging from a 2.5-mm thickness at 2.5-mm intervals to a 5-mm thickness at 5-mm intervals.
CT Analysis
The CT scans were retrospectively reviewed by two radiologists using DICOM image viewing software, with a diagnosis reached by consensus. The involved bowel sites, lesion multiplicity, and type of involvement were assessed on the CT scans, along with the morphological appearance and contrast enhancement patterns of the lesions. The type of GI involvement was categorized as distant GI metastasis or direct GI invasion from adjacent metastatic lesions. The morphological appearance of the lesions was subjectively categorized as: 1) an intraluminal polypoid mass (Fig. 1); 2) an exophytic mass (Fig. 2); or 3) bowel wall thickening. The contrast enhancement for the GI lesions was compared to that of normal adjacent segments of the bowel wall and was categorized as 1) hypo, 2) iso, or 3) hyperenhanced.
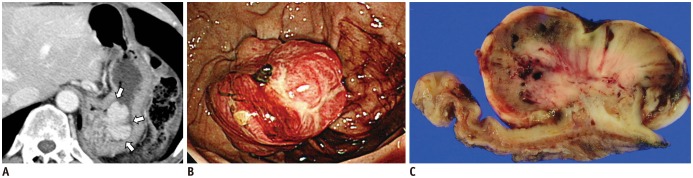 | Fig. 1Gastric metastasis from recurrent renal cell carcinoma in 47-year-old man.This patient had undergone left nephrectomy 5 years earlier.
A. Axial CT image showing strongly enhancing, homogeneous intraluminal polypoid mass arising from gastric fundus (arrows). B. Esophagogastroduodenoscopy revealing lobulated, protruding hyperemic mass with friable mucosa in gastric fundus. C. Gross specimen from stomach after wedge resection. Well-margined, lobulated soft tissue mass with multifocal hemorrhage was observed. Metastatic renal cell carcinoma was confirmed through histopathologic analysis, with mass found to involve submucosal layer of gastric wall.
|
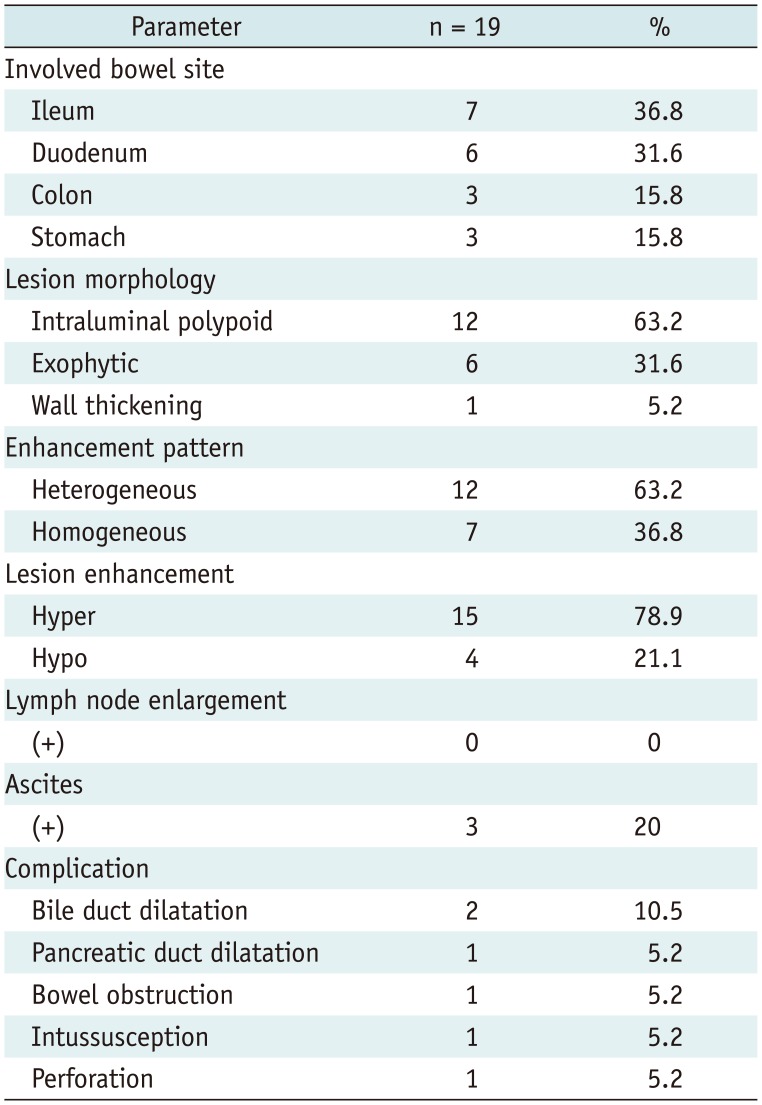
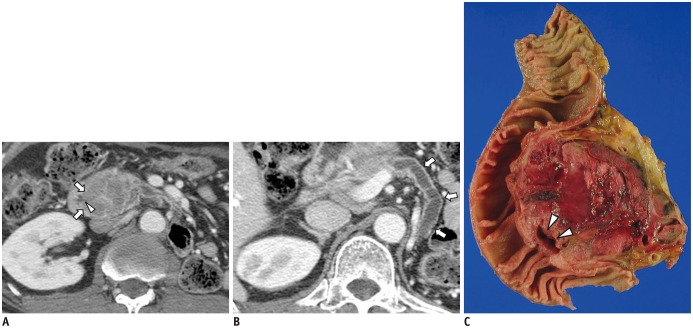 | Fig. 2Direct invasion of metastatic cancer from pancreatic head to duodenum in 63-year-old man.This patient had undergone radical left nephrectomy 9 years before.
A, B. CT scans showing lobulated, heterogeneous soft tissue mass arising from pancreatic head. Mass directly involved medial wall of duodenum, penetrating mural layer of duodenal wall (arrows, A) with suspected ulceration (arrowhead). Distal portion of the main pancreatic duct was diffusely dilated (arrows, B). C. Gross appearance of pancreatectomy specimen was consistent with CT findings of exophytic mass involving medial wall of duodenal second portion with ulceration (arrowheads). Pathologic diagnosis was metastatic renal cell carcinoma.
|
The parenchymal-phase images of the kidney CT scans and portal phase images of pancreas CT scans were evaluated. The enhancement patterns were characterized as homogeneous or heterogeneous, and the images were also evaluated for the presence of bowel complications, lymphadenopathy, ascites and metastasis to other intra-abdominal organs. The size criterion for lymphadenopathy was 10 mm in the shortest axis (22).
Statistical Analysis
Descriptive statistics were used to generate means and standard deviations for continuous and categorical data. The Kaplan-Meier method was used to estimate the overall patient survival following a diagnosis of the GI involvement. All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 21.0 (IBM Corp, Armonk, NY, USA).
Go to :
RESULTS
Clinical and Pathologic Findings
The clinical characteristics of the 15 included patients are summarized in Table 1. The most common clinical presentation was GI bleeding, 10 patients (66.7%), consisting of melena or hematochezia. Of the remaining five patients, two had abdominal pain, two patients had no symptoms, and one experienced weight loss. The mean hemoglobin concentration was 9.4 ± 2.6 g/dL (range, 3.7–13.3 g/dL). All patients had undergone curative nephrectomy, and adjuvant treatment modalities included chemotherapy alone (n = 9), radiotherapy alone (n = 1), and both chemotherapy and radiotherapy (n = 1). Four patients had not undergone adjuvant therapy. The mean time between the radical nephrectomy and detection of GI involvement was 30.4 ± 37.4 months (range, 0–113.4 months; median, 31.4 months).
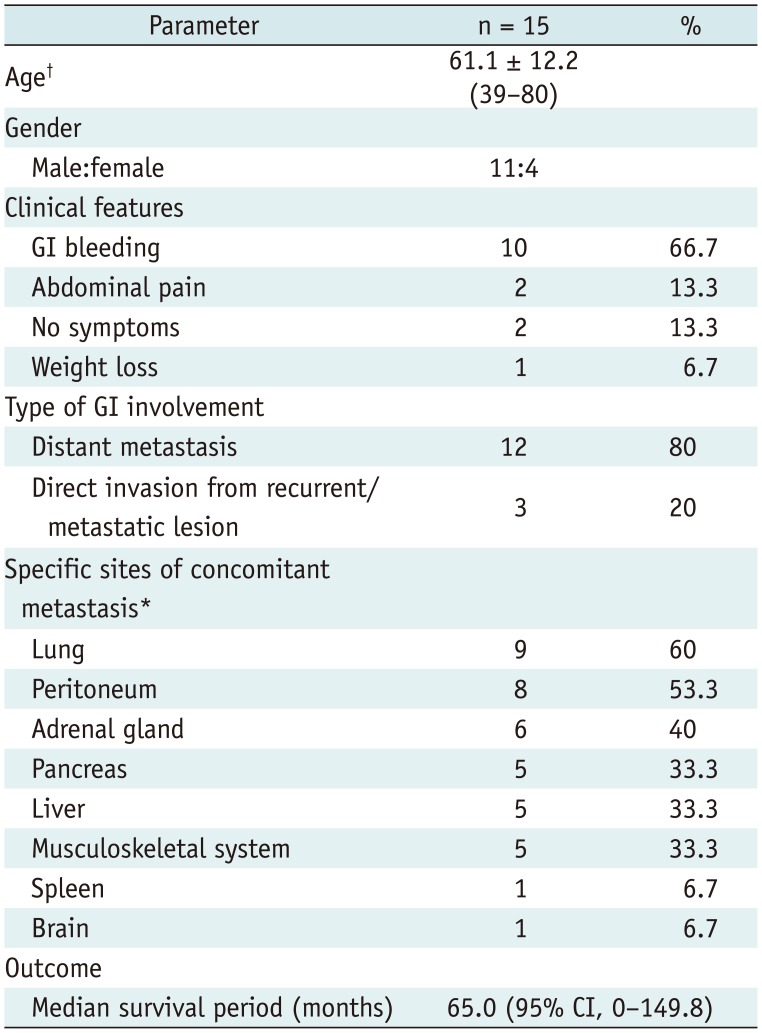
Table 1
Clinical Characteristics of Study Patients
![]()
Fourteen patients (93.3%) had concomitant metastases at the time of GI-involved RCC diagnosis. The mean number of concomitant metastatic sites per patient was 3.1 ± 1.5 (range, 0–6). The sites of simultaneous intra-abdominal metastases included the peritoneum, pancreas, liver, adrenal gland, contralateral kidney, spleen, and regional lymph nodes. The sites of simultaneous extra-abdominal metastases were the lung, brain, and musculoskeletal system. Simultaneous metastasis was most frequently detected in the lung (60%), followed by the peritoneum (53.3%).
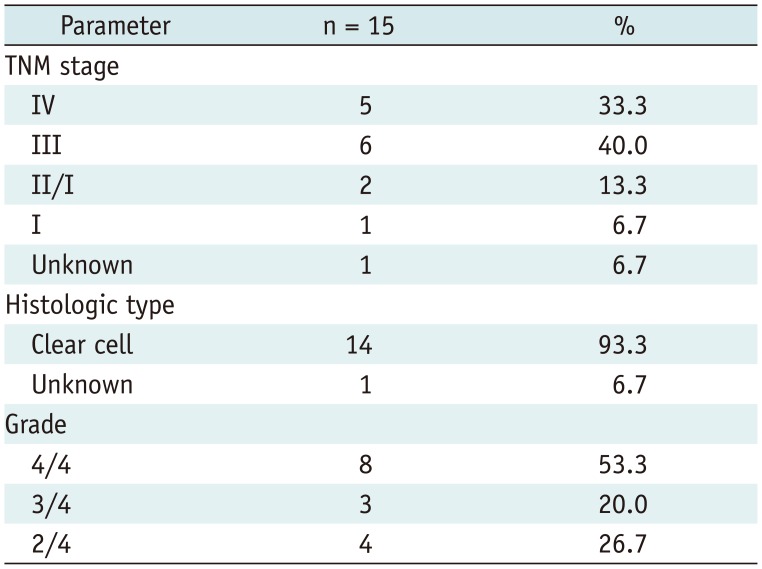
The RCC stage at initial presentation was stage IV in five patients, stage III in six, stage II in two, and stage I
in one. The staging information was not available in one
patient who underwent nephrectomy at another hospital.
The most common histologic type of primary RCC was clear cell carcinoma (n = 14, 93.3%). The histologic type of one lesion could not be determined because the nephrectomy was performed at another hospital. The most common Fuhrman histologic grade was 4/4 (n = 8, 53.3%), followed by 2/4 (n = 4, 26.7%), and 3/4 (n = 3, 20.0%). Histologically, one lesion was an unclassified adenocarcinoma of unknown histologic grade. The pathologic findings of the primary RCC are summarized in Table 2.
The average follow-up period after detection of GI involvement was 20.1 ± 23.5 months (range, 0–76.6 months). Four patients (26.7%) were lost to follow-up, and four (26.7%) died after a mean follow-up period of 18.0 ± 27.2 months (range, 0–65.0 months). Of these four patients, three died due to disseminated metastases with consequent multi-organ failure, and one died due to duodenal ulcer bleeding unrelated to metastasis. The overall median survival from the detection of GI involvement was 65.0 months (95% confidence interval [CI], 0–149.8 months).
CT Findings
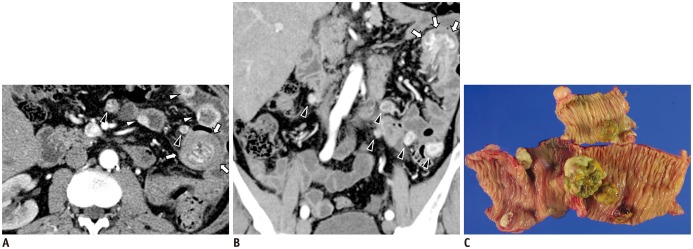
Nineteen lesions were detected in the CT scans of the 15 patients, including seven (36.8%) in the ileum, six (31.6%) in the duodenum, and three (15.8%) in the colon and stomach each. Two patients (13.3%) had multiple lesions (two and four lesions). In 12 patients (80%), the type of GI involvement was distant metastasis after curative nephrectomy, whereas the other three patients (20%) experienced direct GI invasion from an adjacent metastatic lesion. The morphology of the GI lesions varied in the CT scans, with 12 (63.2%) manifesting as intraluminal polypoid masses, six (36.8%) as exophytic masses, and one (5.3%) as wall thickening. In the two patients with more than one lesion, the individual lesions all had the same morphologic features. The average size of all lesions except wall thickening was 30.4 ± 37.4 mm, 36.5 ± 17.0 mm for exophytic lesions and 27.7 ± 8.7 mm for intraluminal polypoid lesions.
The lesions exhibited variable contrast enhancement, with 15 (78.9%) showing predominant hyperenhancement, 12 (63.2%) showing heterogeneous enhancement patterns (63.2%), and seven (36.8%) having homogeneous enhancement patterns.
The complications included bowel obstruction (n = 1) (Fig. 3), intussusception (n = 1) (Fig. 4), bile duct dilatation (n = 1), and combined bile duct/pancreatic duct dilatation (n = 1). Bile duct and pancreatic duct dilatation were associated with lesions at the duodenal second portion and the ampulla of Vater. Intussusception was associated with four lesions in one patient, all of which consisted of an intraluminal polypoid. None of the patients had regional lymphadenopathy. Ascites were found in three patients (20%), with two showing no evidence of malignancy. A summary of the CT findings is provided in Table 3.
 | Fig. 3Ileal metastatic lesion causing obstruction in 62-year-old man who had undergone right nephrectomy 7 years earlier.
A. Axial CT image showing lobulating intraluminal polypoid hypervascular mass in proximal ileum (arrows). Proximal small bowel loops were dilated with small bowel feces signs (arrowheads). B. Coronal reconstructed CT scan showing intraluminal mass (arrows) and diffuse dilatation of proximal bowel. Note small amount of perienteric fluid collection (arrowheads). C. Gross appearance of resected bowel. Firm, polypoid mass involving submucosal layer was confirmed as being metastatic renal cell carcinoma.
|
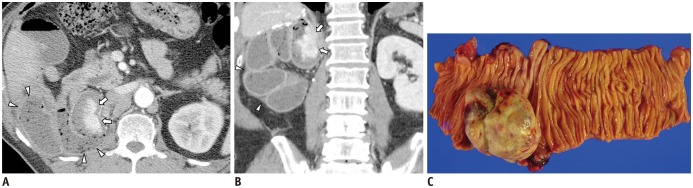
 | Fig. 4Intussusception caused by jejunal lesion from recurrent renal cell carcinoma in 53-year-old man who had undergone left nephrectomy 9 months earlier.
A. Axial CT image showing jejunal intussusception (arrows) with multiple intraluminal masses at other sites (white arrowheads) and peritoneal seeding lesions (black arrowheads). B. Coronal reconstruction image depicting lobulated, hypervascular mass (arrows) at tip of intussusceptum. Note seeding nodules (black arrowheads). C. Gross specimen from segmental jejunal resection, showing several intra-and extraluminal masses. Lesions were pathologically diagnosed as metastatic renal cell carcinoma.
|
Table 3
Summary of CT Findings of GI Involvement from Recurrent RCC in Study Population
![]()
Go to :
DISCUSSION
This analysis showed that GI involvement from recurrent RCC most often manifested as an intraluminal polypoid mass on CT, and a heterogeneous hyperenhancement was also the most common finding. The most frequently involved site was the small intestine, specifically the ileum and duodenum. This distribution of GI metastasis corresponded well with that of a previous study (23), which reported that RCC bowel metastasis was generally in the small bowel.
In our current study, a simultaneous metastasis was most frequently found in the lung, followed by the peritoneum. RCC primarily metastasizes either by hematogenous or lymphatic dissemination (24). The tumor cells can spread into the inferior vena cava, which extends into the right chamber of the heart (25), or can invade regional lymph nodes and traverse the thoracic duct. Thus, the lung tends to be organ that is primarily involved (2426). This finding is consistent with the results presented here, suggesting that the lung is the most common organ of simultaneous metastasis.
The lung is considered a key site for disease spread, with lung tumors metastasizing systematically to other organs. Of our 15 patients, nine (60%) had concomitant lung metastasis, all arising prior to GI involvement. The peritoneum was the second most common site of concomitant metastasis. Peritoneal seeding of RCC, which arises in the retroperitoneal space, may result from either hematogenous spread or direct tumor cell implantation.
Peritoneal metastasis is thought to be uncommon, accounting for 7% of all RCC metastases (24). However, of our 26 patients, eight (53.3%) showed simultaneous peritoneal seeding. The incidence of GI metastasis is much lower than that of peritoneal metastasis and the GI tract is generally considered a late metastatic site, so it was not surprising that peritoneal seeding was accompanied by significant metastatic GI involvement. No patient was found to have regional lymph node metastasis, which stands in contrast with the result of previous studies that reported the lymphatics as the major routes for RCC spread (2627). Our findings suggest that RCC metastasized to the GI tract through hematogenous or peritoneal seeding and not lymphatic dissemination. This finding may explain the high rate of simultaneous lung and peritoneal metastases, together with a low rate of lymph node involvement.
As with primary tumors, metastatic RCC is frequently hypervascular (26), and this was the case in our results. Most of the lesions in our patient population showed heterogeneous hyperenhancement, and most endoscopic and operative findings confirmed their abundant vascularity. Thus, these metastatic lesions may have been the sources of GI bleeding and symptoms. GI bleeding is one of the non-specific signs of GI pathology, so CT may be the primary modality to detect and evaluate metastatic lesions, particularly in the small bowel (28).
Renal cell carcinoma metastasis to the GI can cause several types of intestinal complications. No perforation occurred, which is contrary to our expectations because previous studies suggested a relationship between chemotherapy-related necrosis and intestinal perforation (29). Bowel complications in patients with metastatic lung cancer have shown a greater relationship to the morphologic appearance of GI metastatic lesions than previous treatment modalities, with bowel perforation being significantly associated with wall-thickening lesions (30). Only one of our 15 patients showed bowel wall thickening. The bile duct or pancreatic duct was dilated in patients with duodenal metastasis, especially in the ampulla of Vater and the duodenal second portion.
The overall median survival period of our patients was 65.0 months (95% CI, 0–149.8 months). These results are consistent with the known long-term disease course for patients with metastatic RCC (2345).
The morphologic features and contrast enhancement patterns of GI metastasis varied among our patients, so the differential diagnosis from other GI tract tumors, such as lymphoma, GI stromal tumors, GI neuroendocrine tumors, and malignant melanoma, may be challenging (31). Lymphadenopathy has been reported to be much less prominent, the involved bowel segment shorter, and multi-focality less common in GI metastasis than in lymphoma (32). Although RCC GI metastases and GI stromal tumors can both be presented as heterogeneous masses with variable enhancement patterns, GI metastatic lesions from RCC are mostly intraluminal polypoid masses with hyper-vascularity while GI stromal tumors tend to be exo-luminal. A large percentage of GI neuroendocrine tumors involve regional lymph nodes (33), in contrast to GI metastasis from RCC. Metastatic melanoma, one of the most prevalent malignancies that spread to the GI tract, with a reported incidence of 38–58% (34), is difficult to distinguish from GI metastasis from RCC; both may show hypervascular intraluminal polypoid masses with small bowel predominance. Thus, recognizing a patient's previous medical history may help differentiate these diseases.
This study had several limitations. First, it included a small number of patients due to the rarity of GI metastasis from RCC. However, to the best of our knowledge, this is one of the largest studies to date reporting on the radiologic findings of GI metastasis from RCC. Second, this was a retrospective study for which it was difficult to obtain all relevant information, even with a thorough medical chart review. We only included patients with pathologically confirmed GI metastasis, so the exact incidence of GI metastasis and the diagnostic accuracy of CT in detecting these lesions could not be determined.
In conclusion, GI involvement of recurrent RCC should be considered in the differential diagnosis of patients treated for advanced RCC who present heterogeneous, hyperenhanced intraluminal polypoid masses in the small bowel, with a relative paucity of lymphadenopathy, in their CT scans.
Go to :
 XML Download
XML Download