

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Several organizations have published guidelines for imaging diagnosis of hepatocellular carcinoma (HCC), including the American Association for the Study of Liver Diseases (AASLD), European Association for the Study of the Liver–European Organization for Research and Treatment of Cancer (EASL-EORTC), Asian-Pacific Association for the Study of the Liver (APASL), Korean Liver Cancer Study Group-National Cancer Center (KLCSG-NCC), Japan Society of Hepatology (JSH), and American College of Radiology Liver Imaging Reporting and Data Systems (LI-RADS) (12345). Because the diagnostic criteria of HCC are mainly based on its hemodynamic hallmarks, which include hyperenhancement and washout in the hepatic arterial and venous phases, respectively, these guidelines were established based on the assumption of dynamic computed tomography (CT) or magnetic resonance imaging (MRI) with extracellular contrast media (ECCM) being the first-line modality.
Since its initial approval in 2004, gadoxetic acid (gadolinium ethoxybenzyl diethylenetriamine pentaacetic acid or gadoxetate disodium) has been increasingly used as a contrast agent, especially in Asia and Europe. A survey in 2016 revealed 177 of 195 (90.7%) members of the Korean Society of Abdominal Radiology (KSAR) as using gadoxetic acid for MRI in patients with suspected HCC. Several studies have demonstrated the clinical efficacy of gadoxetic acid in early detection of HCC by providing functional information as a hepatocyte-specific contrast agent as well as hemodynamic information. Although ECCMs and gadoxetic acid are both gadolinium-based contrast agents, they differ in terms of pharmacokinetic characteristics, dosage, and mechanism of action.
The regional heterogeneity of HCC in demographic characteristics, prevalence, surveillance, and socioeconomic status necessitates different treatment approaches, leading to variations in survival outcomes, which affects the diagnostic strategy. Korea has a few unique situations which have steered clinicians towards application of gadoxetic acid-enhanced MRI for early diagnosis of HCC; the highest prevalence of HCC, hepatitis B-related chronic liver disease as the most common underlying etiology, variable curative treatment options–especially hepatic resection or radiofrequency ablation–for early HCC, and affordable treatment because of the national health insurance system. However, diagnosis of HCC by gadoxetic acid-enhanced liver MRI poses certain challenges beyond the scope of current guidelines. Therefore, the KSAR organized meetings to reach a consensus on guidelines for diagnosis of HCC by gadoxetic acid-enhanced MRI with updated perspectives and in consideration of current medical practices in Korea.
MATERIALS AND METHODS
Five organizing members (M. S. P., J. Y. C., S. Y. K., J. M. L., and Y. K. K.) performed literature review in consensus to collect data regarding diagnosis of HCC by gadoxetic acid-enhanced MRI. The PubMed and MEDLINE databases were searched for relevant original articles, systematic reviews/meta-analyses, and consensus statement/guidelines in English. These data were used to extract relevant topics to be addressed in a questionnaire. Debatable issues that were deemed essential for diagnosis of HCC by gadoxetic acid-enhanced MRI were catalogued. Four panels comprising twenty-one panelists–all members of the KSAR and leading abdominal radiologists with expertise in the field of liver MRI–were each assigned one or two issues of debate. An internist (D. Y. K.), a pathologist (E. S. Y.), and two additional abdominal radiologists (M. J. K. and W. J. L.) were invited as advising members. These panels consolidated relevant evidences regarding their assigned issues and prepared a draft of a specific questionnaire, along with a summary of the clinical and scientific rationale behind their suggestions. The questionnaire was drafted at a face-to-face meeting and refined by online discussion.
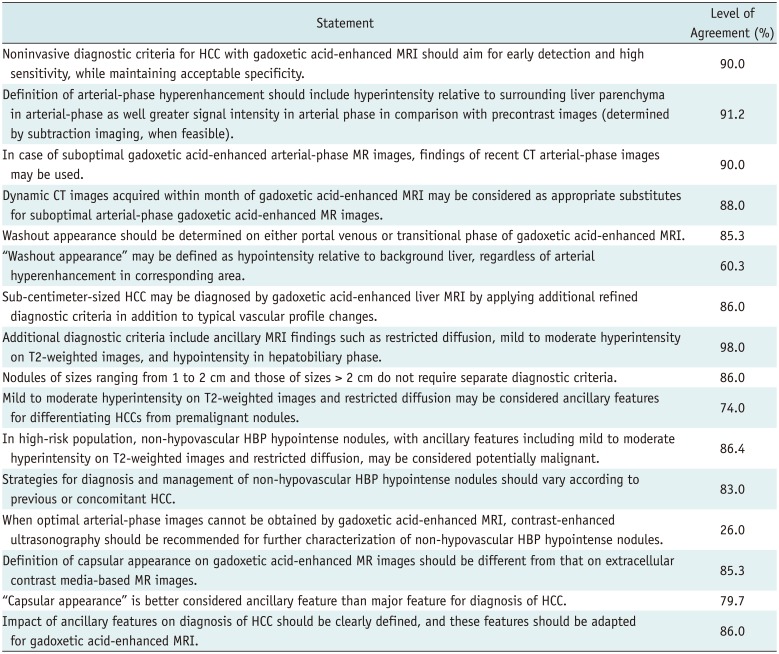
The initial 34 questions were presented to members of the KSAR at a one-day symposium (5th Liver Imaging Day; KSAR-Consensus on Diagnosis of HCC with Gadoxetic Acid-enhanced MRI) on April 16, 2016, which involved didactic lectures and a thorough discussion on the issues of debate. A total of 195 board-certified radiologists specializing in abdominal radiology attended this symposium, where the questionnaire was put through first-round voting. The proposed consensus statement was developed using a modified Delphi method based on a six-point scale: strongly agree, agree with minor reservation, agree with major reservation, disagree with minor reservation, disagree with major reservation, and strongly disagree. Consensus was predefined at ≥ 80% of the sum of votes indicating strong agreement or agreement with minor reservation. Of the 34 questionnaire items, 16 achieved consensus. Following the first-round vote, the questionnaire was refined by the panelists by online discussion and put through second-round voting at a half-day satellite conference, attended by 128 board-certified radiologists specializing in abdominal radiology, during the 39th Scientific Assembly and Annual Meeting of the KSAR, May 14, 2016. Finally, 12 of 16 statements reached the 80% consensus threshold (Table 1). All votes were recorded by secret ballot.
Strategy for Diagnosis of HCC
Hepatocellular carcinoma can be diagnosed by histopathology or non-invasive imaging (6). In fact, HCC is the only malignancy for which pathologic confirmation is not mandatory for diagnosis. With advances in imaging techniques, reliable assessment can be made based on contrast-enhanced CT or MRI findings.
However, extensive geographical differences in tumor biology and regional tendencies make it challenging to establish universal guidelines for diagnosis of HCC. Moreover, guidelines are influenced by the clinical environment and resources available for treatment. The prevalence of HCC in Korea is higher compared to that in Western countries (7). Patients with positive imaging findings in high-prevalence populations are more likely to have HCC than those in low-prevalence populations. Therefore, differences in disease prevalence might affect the likelihood of diagnosis. Choice of therapy is also influenced by regional and institutional tendencies (8). Because liver transplantation eliminates cancer as well as cirrhotic liver tissue, it is considered as the only curative treatment in many Western countries. While deceased donor-liver transplantation (DDLT) constitutes over 90% of liver transplantation cases in Western countries, most such cases in Korea involve living donor-liver transplantation (910). Since organ shortage remains a major limitation for DDLT, Western guidelines for imaging diagnosis focus on achieving high specificity, comparable to that of histopathologic diagnosis, in order to maximize organ utilization. The United States Organ Procurement and Transplantation Network (OPTN) diagnostic criteria for HCC were specifically designed to improve specificity. In Korea, other treatment approaches, such as surgical resection, radiofrequency ablation, transcatheter arterial therapy, and systemic chemotherapy, are widely used for HCC. Given the vast differences in clinical environment between Western countries and Korea, diagnostic strategies for HCC also differ.
Despite controversies regarding its specificity, accumulating evidence shows that gadoxetic acid-enhanced MRI provides improved sensitivity for detecting HCC (11). In Asian countries where gadoxetic acid-enhanced MRI is widely used, diagnostic criteria for HCC are relaxed to increase sensitivity at the expense of specificity (1213). Corresponding with the emphasis on early detection, Asian guidelines have been developed to address early treatment. Because HCC frequently invades vessels and metastasizes to other parts of the liver and body, aggressive treatment of early-stage HCC improves long-term survival (14). A remaining issue is whether diagnostic sensitivity for HCC can be improved while maintaining acceptable specificity. Further studies are required to refine the current diagnostic criteria for HCC.
In the 2016 KSAR consensus meeting on diagnosis of HCC with gadoxetic acid-enhanced MRI, the consensus level for the following statement was 90%.
Definition of Arterial-Phase Hyperenhancement
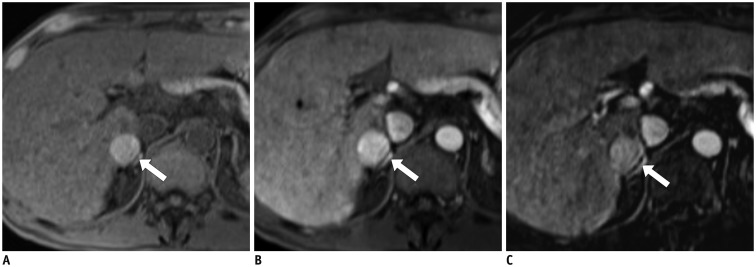
Arterial-phase hyperenhancement, a key imaging feature of HCC (215), is observed in 76–82.7% of small HCCs and only 3.2–9.7% of benign nodules (16). It exhibits high positive predictive value (96.5–98.9%) and specificity (90.3–96.8%) but a low negative predictive value (54.6–62.5%) and moderate sensitivity (76–79.8%) (16). Therefore, acquisition of optimal late arterial-phase images is critical for noninvasive imaging diagnosis of HCC. Arterial-phase hyperenhancement on dynamic contrast-enhanced MR images is generally defined as hyperintensity relative to the surrounding liver parenchyma in the arterial phase (1617). However, diagnosis based on this definition often leads to false-positive results in hepatic lesions that already exhibit hyperintensity on unenhanced T1-weighted images because of accumulation of fat, hemosiderin, glycoproteins, or copper (1819). Comparison of unenhanced and arterial-phase images is necessary to avoid this misinterpretation and detect arterial enhancement (20). However, in some instances, it is challenging to detect or determine arterial hyperenhancement by visually comparing two image sets. Additionally, because of the weak enhancement associated with small volumes of contrast media, low gadolinium concentrations (21), and acute transient dyspnea (11), suboptimal arterial enhancement is more frequent with gadoxetic acid-enhanced MRI than with ECCM-MRI. In such cases, subtraction images of unenhanced T1-weighted and arterial-phase images are helpful in detecting arterial-phase hyperenhancement (Fig. 1) (16222324). However, in subtraction imaging, image quality cannot be assured in case of misregistration due to patient-related or technical factors. Nevertheless, subtraction imaging has shown greater diagnostic accuracy than arterial-phase imaging and visual comparison of precontrast and arterial-phase images (16). Therefore, when available, subtraction imaging is recommended for assessment of arterial-phase enhancement.
In the 2016 KSAR consensus meeting, the consensus level for the following statement was 91.2%.
Consensus Statement
Definition of arterial-phase hyperenhancement should include hyperintensity relative to the surrounding liver parenchyma in the arterial-phase as well greater signal intensity in the arterial phase in comparison with precontrast images (determined by subtraction imaging, when feasible).
Diagnosis Based on Recent CT Arterial-Phase Findings in Case of Suboptimal Gadoxetic Acid-Enhanced MR Images
Because of its higher relaxivity (25), the standard dosage of gadoxetic acid (0.025 or 0.1 mL/kg) (2126) is half in volume and a quarter in gadolinium concentration of the general dosages of ECCMs. The lower dosage of gadoxetic acid in comparison with those of ECCMs results in a shorter bolus transit time and, thereby, a shorter late arterial-phase window, which necessitates particular attention to the arterial-phase acquisition protocol. Additionally, intravenous gadoxetic acid administration is frequently associated with acute transient dyspnea, which results in severe motion artifacts in 12.9–18% of arterial-phase gadoxetic acid-enhanced MR images (112728). These problems have been partially overcome by modification of contrast injection and imaging protocols, including a slower injection rate (1 mL/s rather than 2 mL/s) (2930), detection of arterial phase by test or fluoroscopic bolus monitoring rather than by fixed-scan delay (3132), and multiple short arterial-phase imaging (123334). However, acquisition of optimal arterial-phase gadoxetic acid-enhanced MR images is still challenging in clinical practice. As a practical solution for this issue, the LI-RADS (v2014) allows substitution of arterial-phase findings on suboptimal gadoxetic acid-enhanced MR images with those on recent CT images (35).
In the 2016 KSAR consensus meeting, the consensus levels for the following two statements were 90% and 88%, respectively.
Consensus statements
1. In case of suboptimal gadoxetic acid-enhanced arterial-phase MR images, the findings of recent CT arterial-phase images may be used instead for diagnosis of HCC.
2. Dynamic CT images acquired within a month of gadoxetic acid-enhanced MRI may be considered as appropriate substitutes for suboptimal arterial-phase gadoxetic acid-enhanced MR images.
Appropriate Phase for Determining Washout Appearance
On ECCM-enhanced CT or MR images, the portal venous (PVP) or delayed phases (DP) are used to determine the presence of washout appearance (36). However, there is controversy regarding the most appropriate phase(s) of gadoxetic acid-enhanced MRI for evaluation of washout appearance (3738). Several latest guidelines that incorporate gadoxetic acid-enhanced MRI in the diagnostic algorithm for HCC permit different phases for identifying the washout pattern. The LI-RADS v2014 permits identification of washout appearance only in the PVP in order to maintain high specificity (515). The KLCSG-NCC guidelines v2014 permit identification of washout appearance in the PVP or transitional phase (TP; usually obtained around 3 minutes after contrast administration) (13). The consensus-based algorithm proposed by the Liver Cancer Study Group of Japan (LCSGJ) v2014 includes gadoxetic acid-enhanced MRI as a first-line imaging modality and permits identification of hypointensity in the TP and hepatobiliary phase (HBP) as an alternative to washout appearance for diagnosis of HCC after exclusion of hemangioma using other sequences of MRI and/or other imaging modalities (39). These discrepancies among different guidelines arise from individual preferences for higher sensitivity or specificity (4041), as mentioned in the “Strategy for the diagnosis of HCC”.
Hypointensity in the HBP is a useful feature for diagnosis of small HCCs, which might have influenced the LCSGJ to include the HBP for evaluation of washout appearance (424344). However, most non-HCC malignancies and non-hepatocyte-containing benign lesions and a proportion of borderline nodules (e.g., dysplastic nodules) show hypointensity in the HBP (364546). Therefore, caution should be given in using hypointensity on the HBP as an alternative to washout appearance, since the former has been reported to result in substantially low specificity (< 50%) for detection of arterial-phase hyper-enhancing nodules of sizes ≥ 1 cm (47).
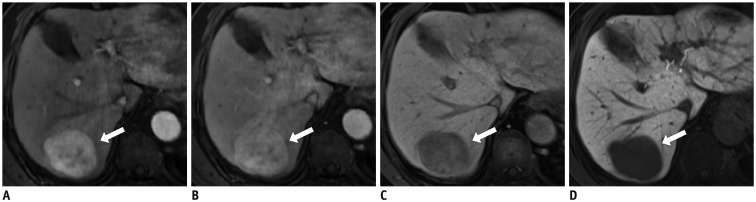
In comparison to multi-phasic CT, typical washout appearance of HCC on gadoxetic acid-enhanced MRI was less frequent if only PVP was used, while it was more frequent if PVP and/or TP was used (Fig. 2) (4748). However, the main concern regarding inclusion of the TP for determining washout appearance is that, the definition of hypointensity in the TP differs from that in the DP in ECCM-enhanced imaging. Since gadoxetic acid uptake by hepatocytes begins as early as the end of the PVP, hypointensity in the TP might be due to the combined effect of de-enhancement and lack of hepatocyte relative to the surrounding liver parenchyma (3549). This “pseudo-washout” can be observed in high-flow hemangiomas (50) and other non-hepatocyte-containing lesions, which decreases the specificity of diagnosis of HCCs, including hypervascular intrahepatic cholangiocarcinomas (ICC) (475152).
In the 2016 KSAR consensus meeting, in responses to the question “Which phase(s) would be appropriate for determining washout appearance?”, “PVP or TP” gained 85.3% votes, while “PVP only” gained 14.7% votes. The reasons for this choice include: 1) inclusion of the TP would increase the diagnostic sensitivity for HCC, but it would not substantially decrease the positive predictive value,which might be a more suitable parameter in Korea, considering the high prevalence of HCC and low availability of DDLT as a treatment option (4); 2) in most cases, high-flow hemangiomas, which mimic HCCs on dynamic phase images (i.e., arterial hyperenhancement and pseudo-washout in the TP), can be ruled out using other MRI sequences (e.g., T2-weighted [T2W] or diffusion-weighted [DW] imaging with an apparent diffusion coefficient map) (505354); and 3) in patients with hypervascular ICCs, which mimic HCCs on gadoxetic acid-enhanced MR images, prognosis following treatment by the same method as that for equivalent-stage HCC has not been well established (5556). To sum up, the appropriate phase for detection of washout appearance on gadoxetic acid-enhanced MR images should be determined considering the inevitable trade-off between sensitivity and specificity in HCC diagnosis. Additionally, the role of ancillary features and effects on clinical outcomes should also be considered.
Sub-Centimeter-Sized HCC
The AASLD and EASL-EORTC guidelines do not allow imaging diagnosis of sub-centimeter-sized HCC. Instead of instantaneous diagnosis of sub-centimeter-sized lesions, these guidelines recommend augmented follow-up at short intervals of 3–4 months, as opposed to regular surveillance, typically at 6-month intervals. This recommendation is based on the belief that a majority of nodules of sizes < 1 cm are unlikely to be HCCs (57). Although there are some contrary evidence (585960), over 90% of arterial-enhancing lesions of sizes < 20 mm were found to be non-neoplastic both in patients with and without history of HCC (6162). In addition, the diagnostic performance of imaging studies for smaller HCCs is low. According to a recent meta-analysis, per-lesion sensitivity for diagnosis of HCCs of sizes < 1 cm was significantly lower compared to that for HCCs of sizes ≥ 1 cm (CT, 31% vs. 82%, p < 0.001; MRI, 48% vs. 88%, p = 0.02) (4263). Even when sub-centimeter-sized lesions are diagnosed on CT or MR images, it would be tricky to co-localize them for intervention or surgery (6465).
In comparison with other imaging modalities, gadoxetic acid-enhanced MRI provides a greater opportunity for detection of small or early HCCs (13), which is supported by evidence that gadoxetic acid-enhanced MRI outperforms CT and ECCM-MRI in diagnosis of lesions of sizes < 1–2 cm (66676869). Moreover, a significant proportion of sub-centimeter-sized lesions detected by gadoxetic acid-enhanced MRI are likely to be or turn into HCC within a short time period (7071). In accordance with these new findings, several recent guidelines, including those of the KLCSG-NCC, JSH, APASL, and LI-RADS v2014, allow imaging diagnosis of sub-centimeter-sized HCC. Given that the mainstay treatment for HCC in Korea is locoregional treatment rather than liver transplantation, detection of smaller lesions susceptible to locoregional v2014, allow imaging diagnosis appears meaningful (72737475). Additionally, new diagnostic techniques, such as fusion of real-time ultrasonography (US) images with CT/MR or contrast-enhanced US images, have made it possible to accurately localize small lesions for local treatment (76), thus bridging the distance between gadoxetic acid-enhanced liver MRI and optimal treatment.
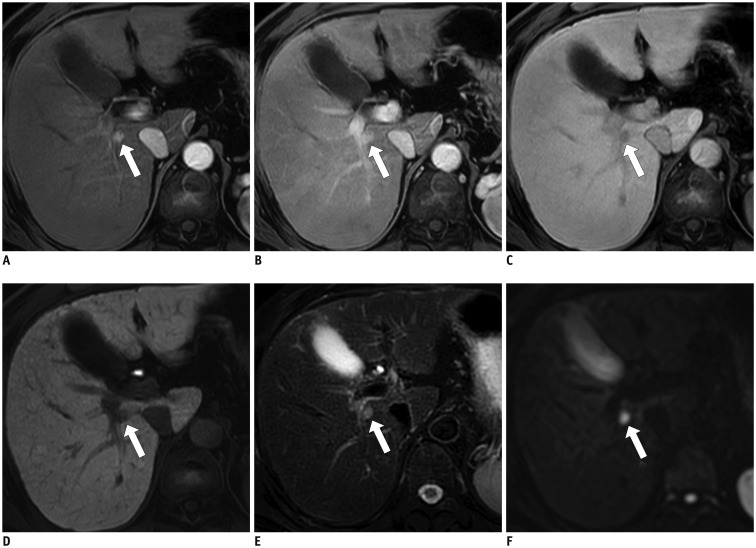
Despite the greater efficacy of gadoxetic acid-enhanced MRI in comparison with those of conventional imaging modalities for diagnosis of sub-centimeter-sized HCC, the diagnostic performance of gadoxetic acid-enhanced liver MRI alone is still unsatisfactory (6377). Recent studies have reported that inclusion of ancillary imaging features, including moderate hyperintensity on T2W imaging (T2WI), restricted diffusion, and hypointensity in the HBP, along with the typical vascular profile changes of HCC improves the diagnostic performance of gadoxetic acid-enhanced liver MRI in small HCCs (Fig. 3) (637177787980). Therefore, typical vascular profile changes should not be relied on as the sole criteria for diagnosis of sub-centimeter-sized HCC.
Besides, the clinical benefits of treatment of sub-centimeter-sized lesions are yet to be proven. Although lesion size of 2 cm has been suggested as being indicative of aggressiveness and invasiveness in HCC (748182), it is not clear whether the same may be extrapolated to sub-centimeter-sized lesions. Therefore, caution should be exercised in diagnosis of sub-centimeter-sized HCC, because the additional cost and possibility of false-positive diagnosis could offset its potential clinical benefits.
In the 2016 KSAR consensus meeting, the consensus levels for the following two statements were 86% and 98%, respectively.
Consensus Statements
1. Sub-centimeter-sized HCC may be diagnosed by gadoxetic acid-enhanced liver MRI by applying additional refined diagnostic criteria in addition to the typical vascular profile changes.
2. Additional diagnostic criteria include ancillary MRI findings such as moderate hyperintensity on T2WI, restricted diffusion, and hypointensity in the HBP.
Nodules of Sizes Ranging from 1 to 2 cm
While some guidelines, including those of the EASL-EORTC and LI-RADS v2014, have provided different diagnostic criteria for nodules of sizes ranging from 1 to 2 cm and for those with sizes > 2 cm, other guidelines, including those of the AASLD, KLCSG-NCC, JSH, and APASL, have not. Because of the concern that nodules of sizes < 2 cm are more likely to be benign lesions than HCC (6162), guidelines such as those of the EASL-EORTC and LI-RADS v2014 have implemented stricter criteria for such lesions in order to maintain high diagnostic specificity. The previous version of the AASLD guidelines required coincidental positivity on two imaging modalities for lesions < 2 cm in size. However, since sequential use of a single imaging modality exhibits similar specificity as simultaneous imaging, with substantially reduced resource expenditure, this policy was discarded in the latest version of the AASLD guidelines (8384). Furthermore, the findings of recent meta-analyses revealed gadoxetic acid-enhanced MRI as exhibiting excellent diagnostic performance for lesions < 2 cm in size (sensitivity, 79–95%; specificity, 89–92%) (6985). Thus, in the era of gadoxetic acid-enhanced MRI, the necessity of the 2-cm cut-off appears to be diminishing.
In the 2016 KSAR consensus meeting, the following statement received 86% votes.
Non-Hypervascular Hypointense Nodules in the HPB
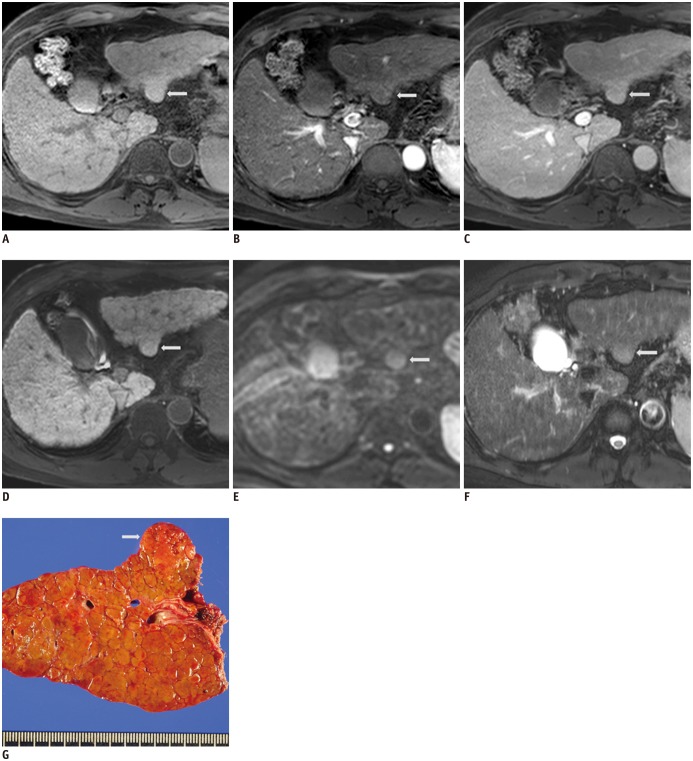
Non-hypervascular hypointense nodules in the HPB is an important issue with gadoxetic acid-enhanced MRI. Several studies have suggested that expression of organic anion transporting polypeptide 1B1/3 (OATP 1B1/3) decreases with tumor progression, which can be assessed using hepatocyte-specific MR contrast agents (364886). Given that OATP 1B1/3 expression decreases prior to angiogenesis, hypointense HBP nodules appear prior to HCCs with typical hemodynamic hallmarks, which proves the feasibility of gadoxetic acid-enhanced MRI in detecting early HCC (41488788). Although the clinical impact of these non-hypervascular HBP hypointense nodules in cirrhotic patients is not yet clearly defined, several papers reported that a substantial proportion of nonhypervascular HBP hypointense nodules (≥ 1 cm) were pathologically diagnosed as early HCCs followed by high-grade dysplastic nodules (HGDNs) (8990), up to 30% of nodules were found to have transformed to typical hypervascular HCCs on follow-up imaging within 3 years (899192939495); additionally, patients with non-hypervascular HBP hypointense nodules exhibited shorter recurrence-free survival after radiofrequency ablation and lower overall survival after liver resection than those without (9697).
However, most guidelines, except JSH or APASL, do not recommend noninvasive imaging diagnosis of non-hypervascular HBP hypointense nodules (23) because of the considerable overlap in features between early HCCs and HGDNs as well as the very low specificity (4148899899100101). Several ancillary features, including restricted diffusion, mild to moderate T2 hyperintensity, diameter > 1.5 cm, and presence of fat, are useful for cross-sectional or longitudinal characterization of non-hypervascular HBP hypointense nodules (899092102103104105106107).
At present, management for patients with non-hypervascular HBP hypointense nodules is controversial and includes several options, such as biopsy, intense follow-up, and additional studies such as contrast-enhanced US (199). Although non-hypervascular HBP hypointense nodules have a probability of transforming into malignant or premalignant nodules, they do not have to be treated as urgently as hypervascular HCCs (99108). A recent study demonstrated simultaneous resection of concomitant non-hypervascular HBP nodules with typical hypervascular HCCs could provide significant benefit for recurrence-free survival (109). However, another study reported only marginal survival benefit from resection of early HCCs (110). Therefore, further studies on management of non-hypervascular HBP hypointensenodule are required.
In the 2016 KSAR consensus meeting, the following statements received 86% and 83% votes, respectively.
Consensus Statements
1. Non-hypervascular HBP hypointense nodules with mild to moderate T2 hyperintensity and/or restricted diffusion should be considered potentially malignant.
2. Strategies for diagnosis and management of non-hypervascular HBP hypointense nodules should vary according to previous or concomitant HCC.
Capsular Appearance
Capsular appearance is defined by the LI-RADS guidelines v2014 as a “peripheral rim of smooth hyper-enhancement in the PVP or DP that unequivocally is thicker or more conspicuous than the rims surrounding background nodule” (5). Capsular appearance is more difficult to recognize with gadoxetic acid-enhanced MRI than with ECCM-enhanced MRI, because early gadoxetic acid uptake by hepatocytes leads to early appearance of strong liver parenchyma enhancement in the PVP and/or TP, which, in turn, obscures any capsular rim enhancement (35). Because of this difference in pharmacodynamics characteristics, capsular appearance should be defined differently on gadoxetic acid-enhanced and ECCM-enhanced MR images. In a recent pathologic correlation study, presence of a smooth dark rim in the HBP was found to exhibit greater correlation with presence of histologic capsule than with conventional capsular appearance on the PVP or TP (76.1% vs. 59.4%; p < 0.001) (Fig. 4) (111). This capsular appearance in the HBP corresponds to HBP hypointense rim, a new, but not major, ancillary feature favoring malignancy described in the LI-RADS v2014 lexicon (35). Capsular appearance has been presented as one of the major features of HCC in the LI-RADS and OPTN guidelines. However, most other current imaging-based diagnostic guidelines do not include capsular appearance as a major feature for HCC diagnosis mainly because of its lack of additional diagnostic value (18). Additionally, interobserver agreement on capsular appearance has been reported as being merely moderate (19).
In the 2016 KSAR consensus meeting, the statement that “capsular appearance is better considered an ancillary feature than a major feature for diagnosis of HCC” received 79.7% votes, while the following statement received 85.3% votes.
Ancillary Features
In view of the limitations of the current HCC diagnostic criteria, which rely on enhancement patterns, addition of a variety of ancillary features would be reasonable method for improving diagnostic accuracy for HCC. Because HCC on gadoxetic acid-enhanced MR images might exhibit different enhancement patterns from that on ECCM-enhanced MR images, other features apart from enhancement patterns could be important for diagnosis of HCC.
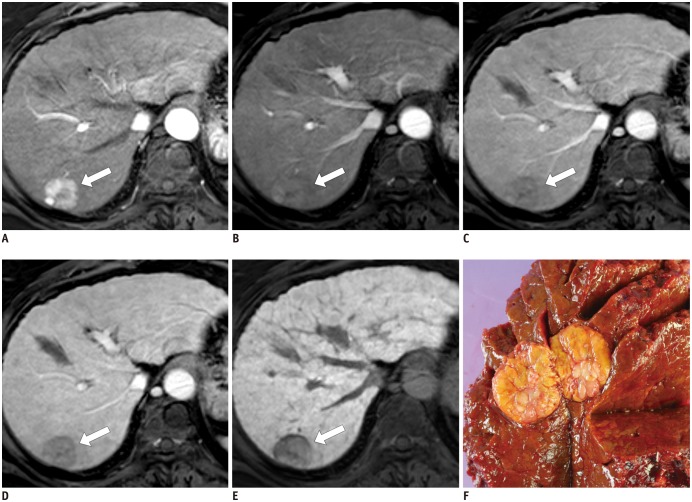
Although they are not specific for HCC, restricted diffusion and mild to moderate T2 hyperintensity are important ancillary features for differentiating between malignant and benign lesions (Fig. 5). However, the sensitivities of these features are not high because several well-differentiated HCCs and some small moderately-differentiated HCCs exhibit iso or hypointensity on T2W and DW images (36). Moreover, DW imaging for diagnosis of HCC presents additional issues. First, background fibrotic parenchyma frequently exhibit lower diffusivity than normal liver, thereby, reducing the lesion–liver contrast on DW images. Second, DW images are prone to spatial distortion and motion artifacts, which make reliable evaluation of hepatic lesions challenging, especially in the left lateral hepatic section, where artifacts due to cardiac motion are inevitable. Third, small HCCs and hemangiomas might exhibit overlapping DW signal intensities (112). For these reasons, the KSAR members could not reach consensus (74%) on the additional role of restricted diffusion and mild-moderate T2 hyperintensity as ancillary features for differentiating HCCs from premalignant nodules under typical circumstances; however, this criterion achieved consensus under special preconditions, including sub-centimeter-sized nodules with typical vascular profile changes (98%) and non-hypervascular HBP hypointense nodules (86.4%) in high-risk populations.
The LI-RADS guidelines are the only ones to incorporate a variety of ancillary features that might favor HCC or benign nodules by a more detailed evaluation of imaging findings (9). The LI-RADS v2014 ancillary features that might favor malignancy include HBP and TP hypointensity, mild to moderate T2 hyperintensity, restricted diffusion, distinctive rim, corona enhancement, mosaic and nodule-in-nodule architecture, intra-lesional fat, lesional iron and fat sparing, blood products, and diameter increase less than the threshold (5). Of these features, distinctive rim, coronal enhancement, mosaic and nodule-in-nodule architecture, and intra-lesional fat are considered as specifically favoring HCC over malignancies (5). These ancillary features in the LI-RADS guidelines are intended to modify the likelihood of diagnosis of HCC but not to upgrade HCC category to LR5 (definitely HCC) without any weighted value on individual features. However, since these ancillary features vary in frequency and importance and are challenging to detect by gadoxetic acid-enhanced MRI, the KSAR members reached an 86% consensus for the following statement.
CONCLUSION
Despite its better diagnostic performance for HCC in comparison with other imaging modalities, most current guidelines have neither accepted gadoxetic acid-enhanced MRI as a mainstream diagnostic algorithm nor defined standard criteria for diagnosis of HCC by this method. The 2016 KSAR meeting reached consensus on several issues of debate from the radiologists' point of view, based on routine clinical practices. Although several challenges remain in terms of optimization and standardization, these consensus recommendations might serve as useful tools to ensure more standardized diagnosis of HCC by gadoxetic acid-enhanced MRI.
 XML Download
XML Download