

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Imaging diagnosis is performed during chemotherapy to evaluate treatment response, detect metastasis and recurrence, and restage the malignancy. For multidisciplinary teams involved in cancer care, the precise imaging validation of a newly detected hepatic nodule has become crucial to achieve optimal treatment during chemotherapy for malignancies. Based on radiologic assessments, the new hepatic nodule could change both the clinical cancer stage and the therapeutic plan. Therefore, if radiologists are aware of a history of underlying gastrointestinal malignancy, they generally consider the metastasis first when they encounter a new hepatic nodule on imaging modalities. However, radiologists should also consider both the effects of chemotherapy on the hepatic metastasis itself, as well as the chemo-induced focal and diffuse alteration of non-tumor bearing hepatic parenchyma, which is important to differentiate mimickers from hepatic metastasis and precaution against impaired hepatic function on non-tumor-bearing liver after hepatic resection.
In recent years, studies have shown that many new hepatic lesions in patients with underlying malignancy are not metastases (123456789101112). Several benign conditions frequently mimic metastasis in the patient during chemotherapy. In this review article, we classify benign hepatic lesions that may occur during chemotherapy as chemotherapy-induced lesions or tumor-associated lesions, with exceptions for infectious conditions such as compromised immunity-associated fungal abscess and incidentaloma. These conditions include chemotherapy-induced focal sinusoidal injury, focal steatosis, and tumor-associated eosinophilic hepatic abscess.
Recently, many studies have reported that chemotherapeutic agents play an important role in new hepatic nodule in patients with underlying gastrointestinal malignancy (13513). There are two reasons why chemotherapy-induced focal hepatopathy have created problems more frequently and more recently in patients with gastrointestinal malignancy than in patients with other malignancies. First, the incidence of metastasis is very high in patients with gastrointestinal malignancy, and therefore more patients with this disease undergo chemotherapy, relative to patients with other malignancies. O'Reilly and Poston (14) reported that hepatic metastasis occurs in 40–50% of patients with colorectal cancer within 3 years after primary tumor resection. Second, many effective new chemotherapeutic agents have been developed recently, which has led to increases in the indication of chemotherapy (1516). An unresectable metastatic lesion could be converted to a resectable lesion by neoadjuvant chemotherapy, and new and effective chemotherapeutic agents could provide a safer resection margin and a decreased recurrence rate for resectable metastasis (15). These new chemotherapeutic agents have increased survival rates, but the focally accentuated hepatopathy that is induced by chemotherapy leads to pseudometastases (36171819202122). Although there is no evidence that chemotherapy-induced focal hepatopathy increases morbidity or mortality (unlike diffusely involved hepatopathy), it is important to understand the imaging features of chemotherapy-induced pseudometastasis, which could otherwise result in a poor prognosis by shifting management plans in the wrong direction, and could also lead to unnecessary biopsies and hepatectomies (158).
Eosinophilic liver disease is a relatively common disease that can be associated with variable disorders such as parasitic infestations, internal malignancies, drug hypersensitivity, allergic conditions, and hypereosinophilc syndrome. A few studies have shown a relatively high rate of coexistence of malignant disease such as stomach cancer and eosinophilic liver disease, which makes it difficult to differentiate focal eosinophilic abscess from metastases on imaging study (2324252627).
In this review, we addressed the updated concept of chemotherapy-induced hepatopathy and tumor-associated eosinophilic abscess in cases of a new hepatic lesion in patients with underlying gastrointestinal malignancy. We discuss the definitions, causal mechanisms, and pathologies of these diseases. The spectrum of imaging finding and the points of differential diagnosis are also described in detail.
Go to : 
Chemotherapy-Induced Focal Hepatopathy
Chemotherapy for Gastrointestinal Malignancy
Curative surgery is the treatment of choice for gastrointestinal malignancies. However, patients with advanced stage disease require postoperative, preoperative, or palliative chemotherapy to achieve a better survival duration or for palliation. Various chemotherapeutic agents, including new targeted agents, are widely used for the treatment of gastrointestinal malignancies as monotherapy or in combination with each other. These chemotherapeutic agents include oxaliplatin, irinotecan, fluorouracil (5-FU), capecitabine, cisplatin, epirubicin, paclitaxel, or docetaxel. It is difficult for radiologists to know which chemotherapeutic agents were included in the combination regimen. Therefore, we briefly describe representative agents and their combination regimen for gastrointestinal malignancy.
Oxaliplatin
Oxaliplatin is frequently used in multidrug regimens in combination with 5-FU/leucovorin or capecitabine. It is widely used for the treatment of gastrointestinal malignancies, including colorectal, gastric, pancreatic, and hepatocellular cancers. The National Comprehensive Cancer Network (NCCN) has recommended oxaliplatin-based chemotherapy regimens (FOLFOX, CapeOx, and FLOX) (Table 1) as a preferred option for adjuvant treatment in colorectal cancer patients (28). Capecitabine and oxaliplatin combination chemotherapy is recommended as a postoperative chemotherapy for gastric cancer by NCCN (28). In patients with colorectal cancer with liver metastases, treatment with the neoadjuvant therapy of oxaliplatin in combination with 5-FU is associated with steatosis, hepatic sinusoidal injury, nodular regenerative hyperplasia, and sinusoidal obstructive disease (1729).
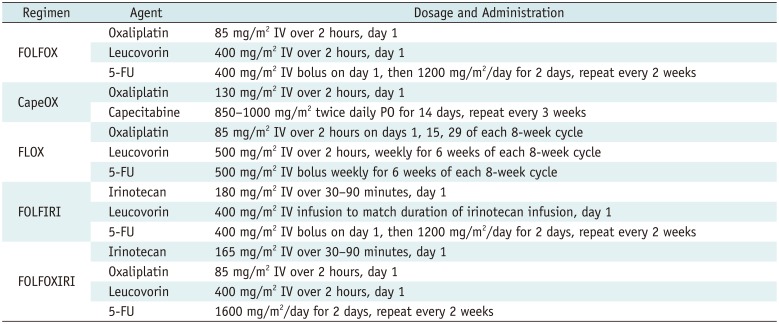
Table 1
Combination Chemotherapy Regimens Including Oxaliplatin or Irinotecan
![]()
Irinotecan
Irinotecan is commonly used to treat colorectal, gastric, cervical, and lung cancers. When provided as neoadjuvant therapy for colorectal cancer with liver metastases, regimens containing irinotecan and 5-FU in combination are associated with steatosis and hepatic sinusoidal injury (22). Irinotecan is mainly eliminated via hepatic metabolism and drug exposure is increased in the setting of hepatic dysfunction (30).
Fluorouracil and Capecitabine
Fluorouracil is one of the most effective and widely used single agents in patients with advanced gastrointestinal malignancies. It is included in all the current reference regimens. 5-FU is primarily metabolized in the liver by dihydropyrimidine dehydrogenase, and inhibition of this enzyme potentiates hepatotoxicity (31). Hepatic toxicity is reported with intravenous administration of the drug, particularly when used in combination with oxaliplatin or irinotecan as neoadjuvant therapy prior to resection of liver metastasis in colorectal cancer (32). Capecitabine is a prodrug that is converted in the intestine into the active metabolite 5-FU. Capecitabine can cause reversible hyperbilirubinemia that is attributed to hemolysis (33).
Chemotherapy-Induced Focal Sinusoidal Injury
Chemotherapy-induced sinusoidal injury can be defined as non-tumor bearing hepatic parenchymal damage initiated by chemotherapy-induced sinusoidal endothelial injury (3435). This is a comprehensive concept that includes several pathologic conditions such as sinusoidal dilatation, peliosis, and nodular regenerative hyperplasia. If these pathologic conditions involve the non-tumor bearing hepatic parenchyma diffusely, it is called sinusoidal obstructive disease. However, it is recently revealed that chemotherapy-induced sinusoidal injury sometimes shows focally accentuated manifestation on non-tumor bearing hepatic parenchyma, and this focal lesion is frequently misinterpreted as hepatic metastasis (135). In 1920, Willmot and Robertson (34) first reported hepatic veno-occlusive disease in a patient during lethal intoxication by pyrrolizidine alkaloids. The relationship between chemotherapy and hepatic veno-occlusive disease became known in the 1950s; and in 1999, DeLeve et al. (35) recognized that the disease process is initiated in the hepatic sinusoid and re-named the disease as sinusoidal obstructive syndrome. In 2004, Rubbia-Brandt et al. (17) reported that sinusoidal obstructive syndrome frequently developed in patients who underwent oxaliplatin-based chemotherapy. Of the patients who underwent oxaliplatin-based chemotherapy, 51–79% showed sinusoidal obstructive syndrome, as compared with only 21–30% of the patients who underwent other chemotherapy (173637). Additionally, in the EORTC Intergroup study of oxaliplatin-based neoadjuvant chemotherapy, sinusoidal lesions (grades 1–3) were observed in 14 of 29 specimens from the chemotherapy group, as compared with 3 of 28 specimens from the non-chemotherapy group. Furthermore, grade 2–3 sinusoidal damage was seen in 12 and 0 patients from the chemotherapy and non-chemotherapy groups, respectively (38). Another study revealed that the incidence of oxaliplatin-based chemotherapy-induced sinusoidal obstructive syndrome was significantly higher in patients who received more than 6 cycles of the chemotherapy, as compared with those who received less than 6 cycles (36). However, these results are confined to diffuse hepatic involvement of chemotherapy-induced sinusoidal injury (so-called sinusoidal obstructive syndrome); the incidence of focally accentuated chemotherapy-induced sinusoidal injury remains unknown.
Pathophysiology
The pathologic manifestation of chemotherapy-induced hepatic sinusoidal injury is variable, especially for oxaliplatin-based chemotherapy. On pathologic analysis, sinusoidal dilatation, peliosis, perisinusoidal fibrosis, and regenerative nodular hyperplasia are noted in sinusoidal obstructive syndrome; these pathologic findings are the serial disease spectrum that is initiated by injury of sinusoidal endothelial cells (Fig. 1) (39). Infused oxaliplatin through the intravenous route induces sinusoidal endothelial injury by depolymerization of the F-actin in sinusoidal endothelial cells, and activates matrix metallopeptidase (MMP)-9 and MMP-2 (Fig. 2A, B) (332404142). The sinusoidal wall integrity is then disrupted, and floating red blood cells are extravasated into the space of Disse through the opened gaps between sinusoidal endothelial cells. Additionally, collagens are deposited at the space of Disse, which is exposed to the sinusoid, and these pathologic conditions are called peliosis and perisinusoidal fibrosis (Fig. 2C-E), respectively. The outlet of the sinusoidal space becomes narrower in the event of extravasation of high numbers of red blood cells and the dilation of more space of Disse. In the same way, perisinusoidal fibrosis results in the sinusoidal outlet obstruction (Fig. 2F). In addition to these two factors, clogging of the damaged necrotic sinusoidal endothelial cells in the sinusoid is also responsible for obstruction and increased pressure in the sinusoid. Consequently, the dilatation of sinusoidal space, disruption of hepatic plates, and hyperplasia of hepatocytes occur by modification of the hepatic blood flow. The enlarged hepatocytes surrounded by atrophic hepatocytes are pathologically defined as nodular regenerative hyperplasia (Fig. 2G) (20). Oxaliplatin-based chemotherapy initiates disruption of the sinusoidal wall integrity and gives rise to serial pathologic conditions, such as peliosis, perisinusoidal fibrosis, sinusoidal dilatation, and nodular regenerative hyperplasia (Figs. 1, 2H).
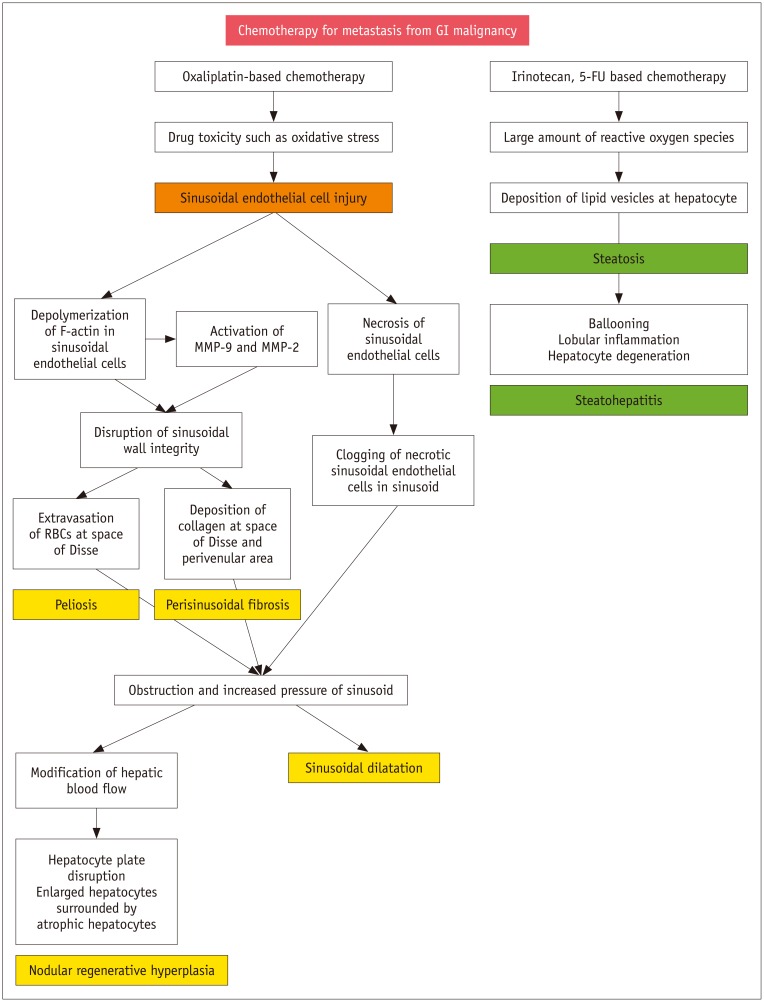 | Fig. 1Algorithm of pathophysiology of chemotherapy-induced hepatopathy.GI = gastrointestinal, MMP = matrix metalloproteinase, RBCs = red blood cells, 5-FU = fluorouracil
|
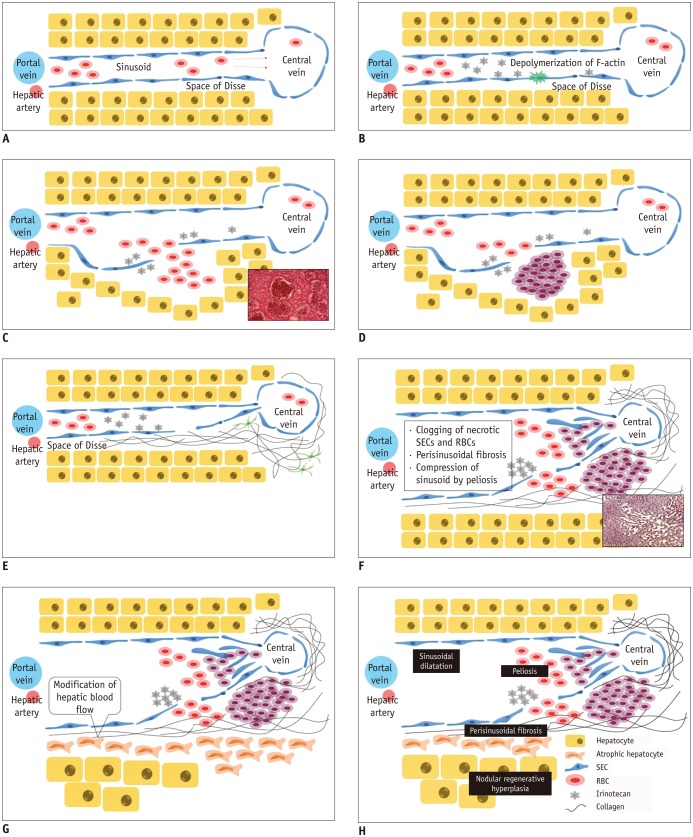 | Fig. 2Schematic illustration of pathophysiology of chemotherapy-induced sinusoidal injury.
A. Normal sinusoid. B. SEC injury and disruption of sinusoidal wall integrity. C. Peliosis with fresh blood. D. Peliosis with old blood. E. Perisinusoidal fibrosis. F. Sinusoidal dilatation. G. Nodular regenerative hyperplasia. H. Chemotherapy-induced sinusoidal injury. RBCs = red blood cells, SEC = sinusoidal endothelial cell
|
Clinical Issues
Most patients with diffuse chemotherapy-induced sinusoidal injury (so-called sinusoidal obstructive syndrome) have no symptoms, unlike patients with other general veno-occlusive disease derived via stem cell transplantation (19). Nonetheless, the situation is different for the patients scheduled to undergo hepatectomy. The risk of bleeding is increased in patients with chemotherapy-induced diffuse sinusoidal injury because the liver tends to become soft and brittle. In short, diffuse chemotherapy-induced sinusoidal injury causes no symptoms, but can lead to poor outcomes of hepatectomy.
On the other hand, focal chemotherapy-induced sinusoidal injury has another clinical significance: although it does not develop into a functional problem, it could mimic hepatic metastasis because it manifests as a newly developed focal hepatic lesion in patients with underlying malignancy.
Imaging Features
The imaging findings of sinusoidal obstructive syndrome are relatively well known through several studies. On abdominal ultrasound, non-specific hepatomegaly, splenomegaly, edematous wall thickening of the gallbladder, ascites, and decrease portal flow are noted in the sinusoidal obstructive syndrome induced by chemotherapy (43). On multidetector computed tomography (MDCT) scanning, the same findings are reported with periesophageal varices (44). Recently, Han et al. (28) also report that “post-oxaliplatin heterogeneity of liver parenchyma” presenting as diffuse and heterogeneous hypoattenuation of the hepatic parenchyma on contrast-enhanced CT is frequently observed in patients who underwent oxaliplatin-based chemotherapy (61.9%), and is predominantly located at the peripheral area (67.1%) and right hepatic lobe (62.4%) (Fig. 3). These imaging findings possibly result from the pathologic findings of sinusoidal obstruction syndrome, which shows irregular liver distribution and abnormal areas intermingled with intact lobules (17). The average time to attain maximal severity of hepatic parenchymal heterogeneity is approximately 4 months (average time, 119.9 ± 44.0 days; range, 33–246 days) after the date of the first session of oxaliplatin-based chemotherapy, and the average time to achieve radiologic remission is approximately 3 months (82.5 ± 68.8 days) after the date of the last session (28). In regard to the development of liver-specific contrast agents for magnetic resonance imaging (MRI), such as gadoxetate disodium (Eovist or Primovist; Bayer Healthcare, Berlin, Germany), a liver-specific MRI contrast agent with combined perfusion and hepatocyte-selective properties could be used to visualize early pathologic change. Heterogeneous reticular pattern are found in the non-tumor bearing parenchyma on hepatobiliary phase (HBP) MRI of the liver using gadoxetate disodium (Fig. 4) (45). The following action mechanisms are suggested: obstruction and high pressure in the sinusoid modify the hepatic blood flow and damage hepatocytes, which results in the low reticular signal intensity on HBP imaging due to disturbed uptake of gadoxetate disodium into the dysfunctional hepatocytes and modified portal flow (45).
 | Fig. 3Three types of hepatic distributions of post-oxaliplatin heterogeneity of liver parenchyma on contrast-enhanced portal phase computed tomography scans.
A. Peripheral distribution: liver shows heterogeneous hypoattenuation mainly in periphery of liver. B. Multifocal distribution: liver shows multifocal hypoattenuations (arrows) in liver. C. Diffuse distribution: liver shows diffuse heterogeneous hypoattenuation.
|
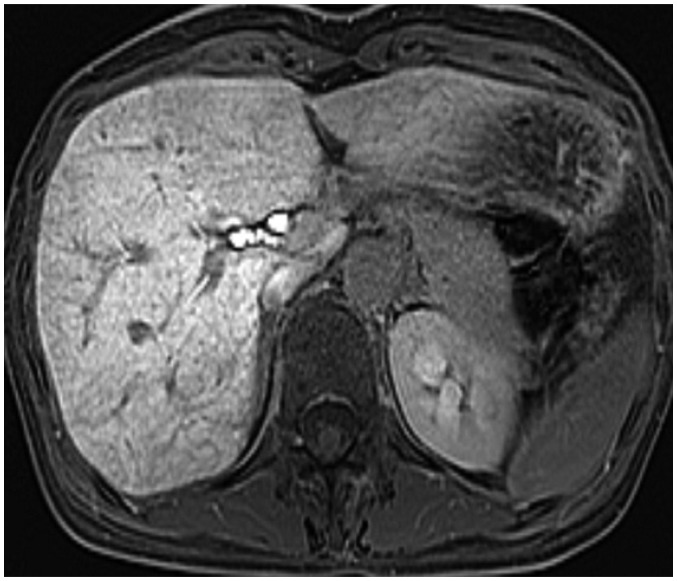 | Fig. 4Magnetic resonance images of 53-year-old woman with heterogeneous reticular pattern in non-tumor bearing parenchyma on hepatobiliary-phase imaging of liver.Pattern was detected 3 months after initiation of chemotherapy for colon cancer. After four cycles of chemotherapy with FOLFOX, variegated reticular parenchymal hypointensity on hepatobiliary phase image had newly developed in non-tumor bearing liver parenchyma.
|
The imaging findings of chemotherapy-induced focal sinusoidal injury mimicking metastasis are not fully elucidated, and is frequently mistaken as metastasis. Until now, few cases of chemotherapy-induced focal hepatopathies mimicking a metastatic tumor on imaging are reported (34647). B-mode ultrasound shows vaguely depicted lesions with variable internal echotexture. On contrast-enhanced MDCT, these lesions appear as hypodense masses that are mostly unenhanced during portal and delayed venous phase, but in some cases they show internal heterogeneous enhancement. Although CT is the primary imaging modality used to evaluate liver metastasis, these lesions are often categorized as indeterminate lesions by the interpreting radiologist, because of the nonspecific CT features of small low attenuation areas. Gadoxetic acid-enhanced MRI usually reveals ovoid shape and hypointensity on pre-contrast and portalphase T1-weighted imaging, without enhancement, slight hyperintensity on T2-weighted imaging, and hypointense nodule on diffusion-weighted imaging. All preoperative imaging findings are consistent with metastatic liver tumors except for negativity on diffusion-weighted images.
Recently, we reported a study that compared the imaging features of pathologically proven chemotherapy-induced focal sinusoidal injury with those of metastatic hepatic nodule using liver MRI (1). Focally accentuated form of chemotherapy-induced sinusoidal injury shows an ill-defined margin (its most valuable feature), non-spherical shape, and intermingled signal intensity pattern. These features are unlike those of a metastatic nodule, which shows a well-defined margin, spherical shape, and homogeneous signal intensity on HBP imaging. On dynamic study, 90% of the metastatic nodules present peripheral rim enhancement during the arterial and portal phases, but chemotherapy-induced sinusoidal injury does not show these enhancement patterns. Several other imaging features of a newly noted hepatic nodule favor chemotherapy-induced focal sinusoidal injury, rather than metastasis: iso-signal intensity on T1-weighted images (hypo-signal intensity in metastasis); iso- or equivocal hyper-signal intensity on T2-weighted images (hyper-signal intensity in metastasis); intermingled hypo- or hyper-signal intensity and less prominent contrast with normal parenchyma on HBP images (homogeneously hypo-signal intensity and clear contrast with normal parenchyma in metastasis); iso-signal intensity on high-b-value diffusion weighted images (high signal intensity in metastasis); and a low apparent diffusion coefficient (ADC) value, but significantly higher than is observed for metastasis on ADC images (a relatively lower ADC value in metastasis) (Fig. 5). Additionally, reticular heterogeneity of background liver tissue is present on HBP images in 69% cases with chemotherapy-induced focal sinusoidal injury that are histopathologically correlated with widespread and milder forms of sinusoidal obstructive syndrome and best depicted on HBP images. Radiologic findings specific to the main pathologic conditions such as sinusoidal dilatation, peliosis, and nodular regenerative hyperplasia in chemotherapy-induced focal sinusoidal injury are unknown, because the pathologic findings appear mixed. But lesions with both peliosis and sinusoidal dilatation are observed with a higher proportion of hyperintensity on T2-weighted images (91%) and well-defined margins (64%). However, this study has limitations of a small group of included patients with pathologically confirmed chemotherapy-induced sinusoidal injury and may not reflect the real numbers in population.
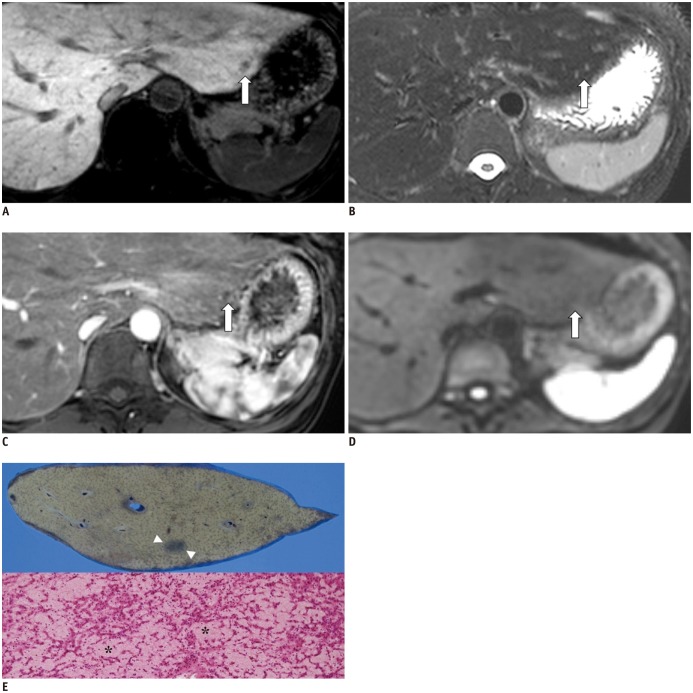 | Fig. 5Magnetic resonance images of 41-year-old man with 1-cm chemotherapy-induced focal sinusoidal injury detected 1 month after initiation of chemotherapy (FOLFOX) for colon cancer.
A. After four cycles of chemotherapy with FOLFOX, ill-defined ovoid lesion (arrow) had newly developed in segment 2 of liver. Lesion shows intermingled hypointensity with combined variegated reticular parenchymal hypointensity on hepatobiliary phase image. B. Iso-signal intensity (arrow) on fat-suppressed respiratory-triggered heavily T2-weighted image. C. No peripheral rim enhancement (arrow) is seen on arterial phase image. D. Iso-signal intensity on high b-value diffusion-weighted image (b = 800 s/mm2, arrow). E. (Upper half) cut surface of liver shows well-demarcated lesion with diffuse hemorrhage (arrowheads) in segment 2. (Lower half) microscopically, lesion shows diffuse sinusoidal dilatation with cystically dilated blood-filled spaces indicative of peliosis (*). Note degenerated red blood cells within dilated sinusoids (hematoxylin and eosin, × 200).
|
Positron emission tomography CT identifies no clear abnormal fluorodeoxyglucose uptake suggestive of malignancy in our experience and based on several other case studies (47).
Chemotherapy-Induced Focal Steatosis/Steatohepatitis
Hepatic steatosis is defined as a condition that is characterized by deposition of lipid vesicles in hepatocytes. Hepatic steatosis could be steatohepatitis, provided there is ballooning of hepatocytes, lobular inflammation, or degeneration of hepatocytes (21). It is difficult to distinguish between steatosis and steatohepatitis, except in terms of pathology. Several studies show that some chemotherapeutic agents, such as 5-FU and irinotecan, are closely related to chemotherapy-induced steatosis (132122). However, the frequency of this pathology is not yet determined (414849).
Clinical Issues
Like chemotherapy-induced sinusoidal injury, diffusely involved hepatic steatosis could affect the surgeon's ability to perform large liver resection, as well as the patient's postoperative morbidity and mortality (especially for steatohepatitis) (22). Recently, chemotherapy-induced steatosis/steatohepatitis is reported more frequently as neoadjuvant chemotherapy has become more common for hepatic metastasis from colorectal cancer. Because steatosis/steatohepatitis affects the outcomes of operations, surgeons would like to determine its existence and grade based on imaging findings. On the other hand, focally accentuated chemotherapy-induced steatosis/steatohepatitis does not cause functional problems, but could mimic a metastasis (8).
Pathophysiology
Distribution of fatty liver disease can vary from diffuse infiltration to focal steatosis. Chemotherapeutic agents, such as 5-FU and irinotecan, reportedly produce substantial quantities of reactive oxygen species, which is suggested as the causal mechanism for the deposition of lipid vesicles in hepatocytes during chemotherapy (374850). The oxygen species promote the deposition of lipid droplets into hepatocytes (Fig. 1).
Imaging Features
As compared with chemotherapy-induced sinusoidal injury, imaging diagnosis of steatosis/steatohepatitis is relatively easy. On ultrasound, hepatic steatosis/steatohepatitis appears as diffuse or focal increased echogenicity. On unenhanced CT, a reduced hepatic-to-splenic attenuation ratio confirms the presence of fat deposition, while an increased craniocaudal liver diameter and an increased caudate-to-right lobe ratio are findings of steatohepatitis (51). Diffusely involved steatosis is not difficult to diagnose using only ultrasound and CT, but focal steatosis could mimic metastasis on ultrasound and CT. However, MRI provides a confirmative diagnosis because steatosis shows signal loss on opposed-phase T1-weighted images, as compared with in-phase images (Fig. 6). In contrast, there is no signal drop on the opposed phase images of metastasis (8).
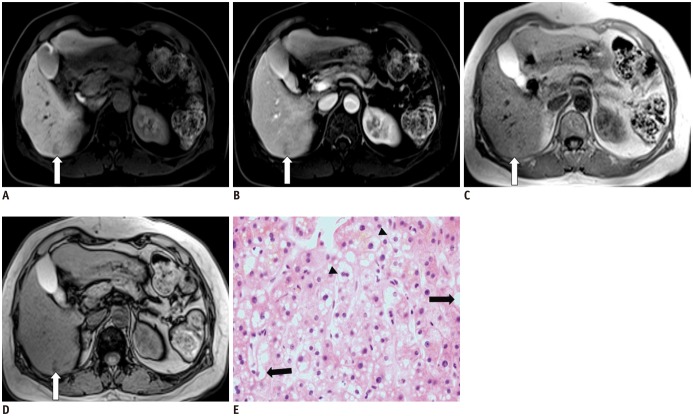 | Fig. 6Magnetic resonance images of 58-year-old woman with chemotherapy-induced focal steatosis mimicking metastasis, which was detected 12 month after initiation of chemotherapy (FOLFOX) for colon cancer.
A. After 12 cycles of chemotherapy, ill-defined ovoid lesion (arrow) had newly developed in segment 6 of liver. Lesion shows hypointensity without combined variegated reticular parenchymal hypointensity on hepatobiliary phase image. B. No peripheral rim enhancement (arrow) is seen on portal phase of dynamic enhancement. C, D. There is high signal nodular lesion (arrow) on in-phase and signal drop (arrow) on opposed-phase of chemical shift image, respectively. E. Microscopically, liver shows microvesicular and macrovesicular steatosis. Small fat droplets are assembled around centrally located nuclei (arrowheads) and large fat droplets replace nuclei to periphery of cell (arrows) (hematoxylin and eosin, × 200).
|
Go to :
Tumor-Associated Eosinophilic Abscess in the Liver
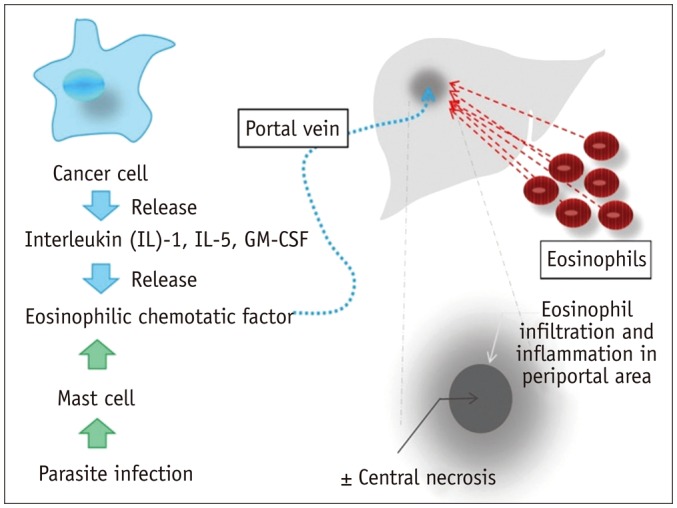
Focal eosinophilic liver disease was previously known as eosinophilic abscess, eosinophilic infiltration, or eosinophilic granuloma. It can be defined as localized eosinophilic infiltration with or without central necrosis in the liver, near the portal vein (2752). Usually, this lesion develops in patients with parasite infections. Currently, it is suggested that tumors themselves could cause eosinophilic abscesses that mimic hepatic metastases (10272930535455). The known mechanism for tumor-associated eosinophilic abscess in patients with underlying malignancy is as follows: eosinophils are aggregated in the liver by the eosinophilic chemotactic factor stimulated by interleukin (IL)-2, IL-5, and granulocyte macrophage colony-stimulating factor, which is derived from the primary cancer cells and is then transported into the liver through portal flow (Fig. 7) (2654). In fact, if chemotherapy-induced focal steatosis develops at the predilection site (e.g., adjacent to the falciform ligament or ligamentum venosum, in the porta hepatis, and in the gallbladder fossa), it is not difficult to diagnose. However, focal steatosis in unusual sites should be carefully distinguished from metastasis.
This lesion appears as low echoic nodules on ultrasound and as low attenuation in the portal phase on dynamic studies of CT scanning. It is not well defined on the arterial or delayed phase (29). Additionally, unlike metastasis, the infiltrative features of the lesion appear as a fuzzy/indistinct margin and irregular shape on CT and MRI. Furthermore, as compared with metastasis, the lesion itself shows a signal intensity that is reduced to a lesser extent on T1-weighted images, and is increased to a lesser extent on T2-weighted images (11). Recently, more specific image findings are revealed based on the pathologic characteristics of the disease (11). These findings can help differentiate this lesion from metastasis. Focal eosinophilic liver disease is consistent with eosinophilic infiltration and central necrosis, and these pathologic features result in size discrepancies on T1-weighted images and HBP images. On T1-weighted images, only the necrotic portion shows low signal intensity. However, on HBP images, the combined necrotic portion and non-necrotic eosinophilic infiltrative portion has low signal intensity. The maximum diameter of the lesion on the unenhanced T1-weighted image < 50% of that on the HBP image shows 100% positive predictive value for the diagnosis of focal eosinophilic liver disease (Fig. 8).
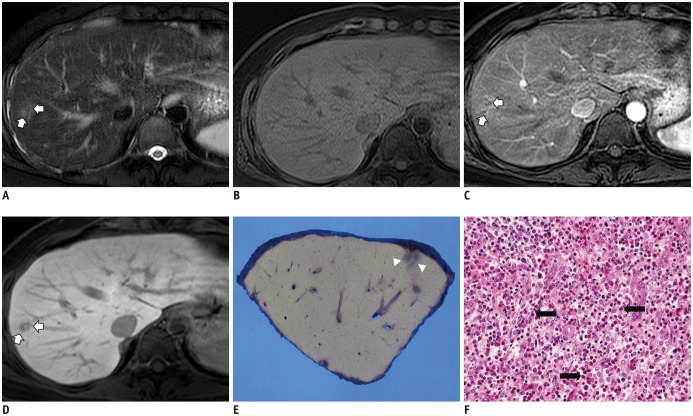 | Fig. 8Magnetic resonance images of 55-year-old man with colon cancer and surgically confirmed eosinophilic abscesses in liver.
A. Respiratory-triggered T2-weighted turbo spin-echo image shows single hyperintense nodular lesion (arrows) in right hepatic lobe. B. On T1-weighted gradient echo magnetic resonance imaging, lesion is almost isointense. C. On arterial phase, lesion appears as rim-enhancing nodule (arrows). D. On hepatobiliary phase image, lesion is clearly seen as relatively well-defined hypointense areas (arrows), and appears larger than that observed in (B).
E. Ill-demarcated grayish white lesion is noted at subcapsular area of liver (arrowheads). F. Microscopically, lesion (indicated by arrowheads in E) is composed of mixed inflammatory cell infiltrates, predominantly with eosinophils (arrows), replacing normal hepatocytes (hematoxylin and eosin, × 200).
|
Go to :
CONCLUSION
A focal hepatic lesion that is newly developed in a patient with underlying malignancy is not always a metastasis. Moreover, in patients who have undergone chemotherapy for gastrointestinal malignancy, a substantial proportion of newly noted hepatic nodules could be chemotherapy-induced focal hepatopathies, such as chemotherapy-induced focal sinusoidal injury, focal steatosis, and tumor-associated eosinophilic abscess. If the patient has received oxaliplatin-based chemotherapy, chemotherapy-induced focal sinusoidal injury should be considered in the differential diagnosis. To differentiate some types of pseudometastasis from liver metastasis during chemotherapy, various radiologic findings should be considered in liver dynamic CT and MRI. These typical radiologic findings include the margin, shape, signal intensity pattern, and enhancement pattern of the pseudometastasis, as well as characteristic changes to the background liver (Fig. 9). To achieve early and accurate diagnosis, provide appropriate treatments, and avoid unnecessary invasive treatments and salvage regimens, it is clinically important to 1) be familiar with the imaging characteristics of these mimickers, 2) understand their relationships with chemo-agents, and 3) understand the pathophysiologies of chemotherapy-induced focal sinusoidal injury, steatosis, and tumor-associated eosinophilic abscess.
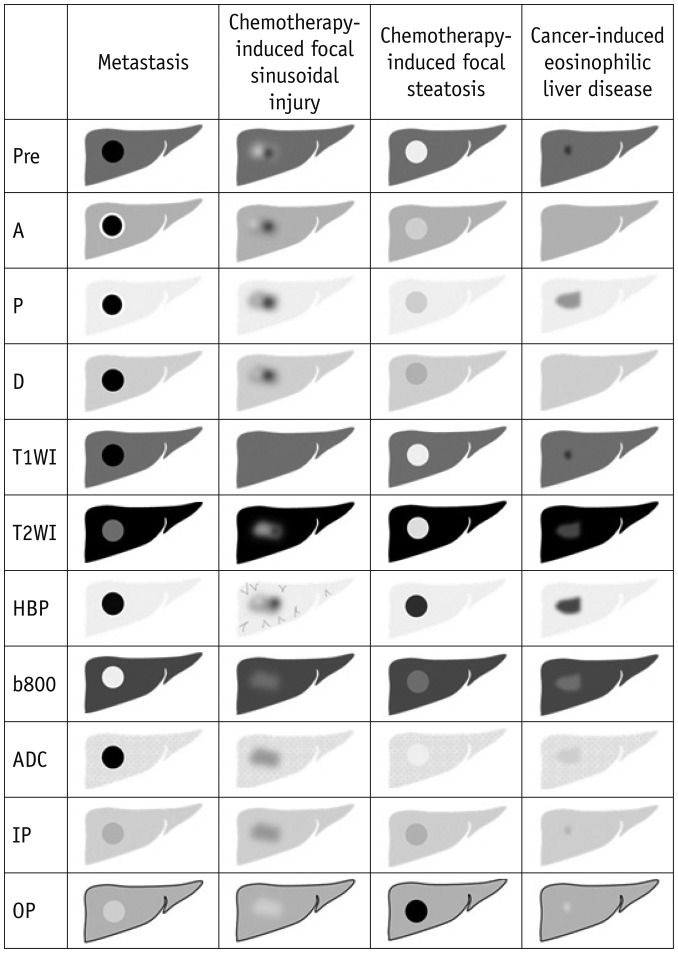 | Fig. 9Schematic representation of typical magnetic resonance imaging features of hepatic pseudometastasis during chemotherapy in patients with gastrointestinal malignancy.A = arterial phase image, ADC = apparent diffusion coefficient, b800 = diffusion weighted image (b value = 800 s/mm2), D = delayed-phase image, HBP = hepatobiliary phase, IP = in-phase magnetic resonance image, OP = opposed-phase magnetic resonance image, P = portal-phase image, Pre = precontrast T1-weighted image, T1WI = T1-weighted image, T2WI = T2-weighted image
|
Go to :
 XML Download
XML Download