

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Positron emission tomography (PET) using fluorine-18-401labeled fluoro-2-deoxy-D-glucose (FDG) has been widely accepted as a useful, noninvasive imaging modality for evaluating a variety of neoplastic and brain diseases (1).
The brain and liver are useful organs for evaluating FDG uptake because they are relatively large in human bodies and can be shown with certainty on FDG-PET images. In general, the brain demonstrates the highest physiologic FDG uptake in the human body because of its high glucose metabolism, and this high FDG uptake complicates differentiating lesions from normal tissue in clinical situations. FDG uptake by the brain is sometimes abnormally low, even in the absence of brain disease. The most well known cause of reduced brain FDG uptake is a hyperglycemic state at the time of the FDG PET/CT study (2). In addition, a number of studies have revealed other factors associated with reduced brain FDG uptake (3456789). In contrast, the liver generally shows low FDG uptake that is only slightly higher than that of the mediastinal blood pool. Because the liver can show increased uptake even in the absence of malignant disease, true hepatic lesions with mildly increased uptake can be overlooked. It has been reported that liver FDG uptake is also affected by various clinical factors (101112131415).
Concurrent low brain and high liver uptake are sometimes observed on FDG PET; however, no studies have yet investigated the clinical significance of this pattern. We intended to investigate potential associations between degree of brain FDG uptake, degree of liver FDG uptake, and various physical and hematological factors, with the ultimate aim of defining determinants of low brain uptake and high liver uptake on FDG PET. Because we included all components of metabolic syndrome (MS) in the present study, we also investigated the potential clinical significance of concurrent low brain and high liver FDG uptake related to MS.
MATERIALS AND METHODS
Subjects
The Institutional Review Board approved our study design and all informed consent exemptions, and we retrospectively reviewed data from 264 consecutive males who had undergone general health check-ups, including FDG PET/CT scans to screen for malignancies. None of the enrolled subjects had a known malignant disease, hepatitis B or C, cardiac symptoms, previous coronary artery disease, neurodegenerative disorders, psychiatric diseases, or previous cerebral vascular accidents, nor did they use neuropsychological medications. We measured their height, weight, and waist circumference and calculated body mass index (BMI, kg/m2) as an index of obesity. After at least five minutes of rest, we measured systolic and diastolic blood pressures (SBP and DBP, mm Hg). After an overnight fast, we drew peripheral blood and measured the levels of fasting blood glucose (FBG, mg/dL), glycated hemoglobin (HbA1c, %), total cholesterol (mg/dL), high-density lipoprotein cholesterol (HDLc, mg/dL), low-density lipoprotein cholesterol (LDLc, mg/dL), triglyceride (TG, mg/dL), aspartate aminotransferase (AST, IU/L), alanine aminotransferase (ALT, IU/L), γ-glutamyl transpeptidase (γ-orgGT, IU/L), alkaline phosphatase (IU/L), total bilirubin (mg/dL), total protein (g/dL), blood urea nitrogen (mg/dL), creatinine (mg/dL), erythrocyte sedimentation rate (mm/hr), high-sensitivity C-reactive protein (mg/L), insulin (µIU/mL), and thyroid-stimulating hormone (TSH, µIU/mL).
A radiologist determined the presence of fatty liver using abdominal ultrasonography interpretation, and we obtained the Framingham Risk Score (FRS) from the medical records. We estimated insulin resistance using the homeostasis model assessment of insulin resistance (HOMA-IR) equation from the FBG and insulin concentrations as follows: HOMA-IR = (FBG × insulin) / 405. We conducted all measurements on the same day as the FDG PET/CT scan. We defined diabetes mellitus (DM) as serum FBG level ≥ 126 mg/dL or the use of any hypoglycemic drug and hypertension (HTN) as SBP ≥ 140 or DBP ≥ 90 mm Hg or the use of any anti-hypertensive drug.
Patients were diagnosed with MS based on criteria established by the American Heart Association and National Heart, Lung, and Blood Institute using waist circumferences adjusted for Asians, specifically, when three or more of the following criteria were met: 1) waist circumference ≥ 90.0 cm; 2) fasting TG ≥ 150 mg/dL; 3) HDLc < 40 mg/dL; 4) SBP ≥ 130 mm Hg, DBP ≥ 85 mm Hg, or use of HTN medication; and 5) FBG ≥ 100 mg/dL or use of DM medication (16).
FDG PET/CT Protocol
All subjects were examined using a dedicated PET/CT scanner (Discovery 710; GE Healthcare, Waukesha, WI, USA). FDG PET/CT imaging was performed 60 min after injection of FDG at a dose of 3.7 MBq/kg (0.1 mCi/kg) body weight. Before FDG administration, subjects were asked to fast for at least 6 hours. Blood glucose level at the time of FDG injection was less than 180 mg/dL in all subjects. No additional glucose control drugs were used in subjects with high blood glucose levels (17). Sixty minutes after the administration of FDG, low-dose CT covering the area from the vertex of the skull to the proximal thigh was performed for attenuation correction and precise anatomical localization. Thereafter, an emission scan was conducted in the three-dimensional mode. Emission scan time per bed position was 1.5 minutes, and nine or 10 bed positions were acquired. PET data were obtained using a high-resolution whole-body scanner with an axial view field of 15.7 cm. The average axial resolution varied between 5.6 mm (full width at half maximum) at 1 cm and 6.3 mm at 10 cm. The average total PET/CT examination time was 15 minutes. The CT scan was obtained with tube voltage of 120 kVp and tube current of 30–180 mAs. The PET data were iteratively reconstructed with attenuation correction and then reoriented in axial, sagittal, and coronal slices.
Image Analysis
We reviewed the images using an Advantage Workstation 4.6 (GE Healthcare), using round regions of interest (ROIs) to measure the standardized uptake values (SUVs) of the brain and liver of each subject. We calculated SUV as the tissue activity of the ROI (MBq/g)/(injected dose [MBq]/body weight [g]) on PET images and measured the maximum SUVs (SUVmax) of the brain and liver from ROIs (2 cm and 5 cm diameters, respectively) manually placed over the frontal cortex at the level of the centrum semiovale (318) and the right lobe of the liver parenchyma, respectively. Because SUVmax is most conveniently measured by the surrounding target region and is less observer-dependent and more reproducible than SUVmean in spite of its vulnerability to image noise (19), we used SUVmax as a representative value for glucose metabolism in the brain and liver.
We classified all subjects whose brain SUVmax was below the 25th percentile of the entire study population as having low brain uptake and all subjects whose liver SUVmax was above the 75th percentile as having high liver uptake. According to the combination of brain and liver FDG uptake, we classified all subjects into one of three patterns as follows: pattern 1, concurrent low brain and high liver uptake; pattern 2, either (A) low brain uptake alone or (B) high liver uptake alone; pattern 3, neither (Fig. 1).
Statistical Analysis
Values are expressed as the mean ± standard deviation or number (%). To compare between-group differences, we used the Student's t test or the Mann-Whitney U test, as appropriate, for the continuous variables. We also used the chi-square test or Fisher's exact test for the categorical variables. We compared the three patterns classified by the combination of brain and liver FDG uptake using one-way ANOVA analysis followed by post hoc testing with the Student-Newman-Keuls comparison test, and we used multiple logistic stepwise regression analysis to identify predictive factors for low brain uptake and high liver uptake. We evaluated the correlations between variables using Spearman rho rank correlation analysis. We performed all statistical analyses using MedCalc (ver. 14.12.0, MedCalc Software bvba, Ostend, Belgium) and defined statistical significance as p < 0.05 (two-tailed test).
RESULTS
Subject Characteristics According to the Intensity of FDG Uptake in the Brain and Liver
We classified a total of 264 male subjects (mean 46.1 years; range 38–65 years) according to their brain and liver FDG uptake; the subjects' clinical characteristics are compared in Table 1. The mean SUVmax values for the brain and liver in all subjects were 13.47 ± 2.16 and 3.80 ± 0.50, respectively. Of the 264 subjects, 50 (18.2%) had MS. Compared with subjects without MS, the subjects with MS had lower brain FDG uptake (12.30 ± 2.44 vs. 13.75 ± 2.00, p < 0.001) and higher liver FDG uptake (4.14 ± 0.49 vs. 3.72 ± 0.47, p < 0.001).
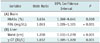
Age (p = 0.003), FBG (p < 0.001), AST (p = 0.037), HbA1c (p < 0.001), the number of MS components (p < 0.001), FRS (p = 0.017), and fatty liver (p = 0.037) were associated with brain FDG uptake. SBP (p < 0.001), DBP (p = 0.003), waist circumference (p < 0.001), FBG (p = 0.018), TG (p = 0.001), total cholesterol (p = 0.003), LDLc (p = 0.002), AST (p = 0.007), ALT (p < 0.001), γ-GT (p < 0.001), HOMA-IR (p < 0.001), insulin (p < 0.001), BMI (p < 0.001), HbA1c (p = 0.012), the number of MS components (p < 0.001), and fatty liver (p < 0.001) were associated with liver FDG uptake. We conducted multiple logistic stepwise regression analysis including these factors, and the results revealed that FBG and HbA1c were the strongest predictive factors for low brain FDG uptake and waist circumference and γ-GT were the strongest predictors for high liver FDG uptake (Table 2).
Comparison of MS Components According to FDG Uptake by the Brain and Liver in Subjects with and without MS
Regardless of the presence of MS, subjects with low brain FDG uptake had significantly higher FBG levels than did those with high FDG uptake (with MS; 122.7 ± 23.6 mg/dL vs. 96.9 ± 9.5 mg/dL, p < 0.001, without MS; 98.2 ± 11.9 mg/dL vs. 90.5 ± 9.0 mg/dL, p < 0.001). Moreover, subjects with high liver FDG uptake had significantly larger waist circumferences than those of the men with low FDG uptake (with MS; 95.2 ± 5.9 cm vs. 89.1 ± 7.1 cm, p = 0.002, without MS; 90.0 ± 7.3 cm vs. 82.2 ± 6.1 cm, p < 0.001) (Table 3).
Comparison of Clinical Variables among Three Patterns Classified by Combination of Brain and Liver FDG Uptake
Eleven subjects (4.2%) showed concurrent low brain and high liver FDG uptake, and all but one of these subjects (90.9%) had MS. Of the 142 subjects with pattern 3, 132 (93.0%) did not have MS (Fig. 2), and the proportion of MS in subjects with pattern 2 was 27.0% (30/111). Subjects with pattern 1 had higher values for SBP, waist circumference, FBG, TG, ALT, HOMA-IR, insulin, HbA1c, and BMI than did those with patterns 2 or 3 (Table 4). Subjects with pattern 2 had higher values for SBP, DBP, waist circumference, FBG, TG, total cholesterol, LDL, AST, ALT, γ-GT, HOMA-IR, HbA1c, BMI, and FRS than did those with pattern 3. FRS was correlated with brain (r = -0.183, p = 0.003) and liver (r = 0.122, p = 0.047) FDG uptake.
DISCUSSION
The present study demonstrated that various clinical and hematological factors are associated with metabolic activity in the brain and liver, as measured by FDG PET, and subjects with concurrent low brain and high liver FDG uptake had a higher prevalence of MS. MS is a potent predictor of future cardiovascular disease and its prevalence (2021). Thus, we evaluated the relationship between this FDG uptake pattern and cardiovascular risk. The results revealed that subjects with this FDG uptake pattern had higher values for the various factors that are closely associated with cardiovascular risk than subjects without this pattern.
In this study, FBG and HbA1c were the strongest determinants of brain FDG uptake; brain SUVmax was significantly lower in subjects with high FBG, regardless of the presence of MS. Glucose is a major substrate for brain energy metabolism, and in the hyperglycemic state, excess unlabeled glucose and the action of insulin can alter FDG accumulation in the body as follows. First, glucose transporters (GLUTs) become saturated in the presence of excess unlabeled glucose (2223). Second, plasma insulin levels increase, resulting in translocation of GLUT-4 from an intracellular pool to the plasma membrane (2425). Whereas saturation with unlabeled glucose is likely to reduce FDG uptake in insulin-insensitive organs such as the brain, insulin is likely to increase FDG uptake in insulin-sensitive tissues such as the myocardium and muscles. This implies that the saturation effect of unlabeled serum glucose is more evident in tissues with high glucose metabolism than in organs with lower glucose demands. One study also demonstrated that blood glucose only exerts a significant impact on FDG uptake in the brain, where there is a high level of glucose metabolism, whereas a nonsignificant effect was observed in organs that consume less glucose such as the liver and spleen (2). Because HbA1c reflects average plasma glucose over the previous eight to 12 weeks (26), this finding implies that chronically uncontrolled hyperglycemia also has a significant influence on brain FDG uptake as well as acute hyperglycemia. However, serum glucose levels (< 180 mg/dL) were sufficiently low in the present study that they may not have saturated the GLUTs, and therefore, other mechanisms should be considered. Insulin resistance, which is broadly defined as reduced tissue responsiveness to the action of insulin, is one possible explanation. Insulin increase and subsequent GLUT activation is a normal response to hyperglycemia, whereas it appears that dysglycemia is the main cause of low FDG uptake in the brain; in dysglycemia, high serum glucose is not the cause but the result of peripheral insulin resistance. Peripheral insulin resistance strongly corresponds to brain insulin resistance owing to reduced insulin transport into the brain or potentially similar changes in receptor sensitivity and activation (2728), and insulin resistance leads to decreased GLUT1 and GLUT3 expression and consequent glucose uptake in the brain (29). This may be why our enrolled subjects showed different brain FDG uptake despite exhibiting similar insulin levels (p = 0.922).
In contrast to brain FDG uptake, FBG did not influence liver FDG uptake. Moreover, we observed no differences in the serum FBG levels of subjects with high versus normal liver uptake regardless of the presence of MS. The strongest determinants of liver FDG uptake were waist circumference and γ-GT, which supports the findings of a previous study that found that BMI was the strongest determinant (13). Both waist circumference and BMI are regarded as obesity-related factors, and obesity is associated with increased plasma levels of inflammatory cytokines such as tumor necrosis factor-α (TNF-α) and interleukin-6 (IL-6). Altered long-term expression of liver metabolic enzymes mediated by TNF-α and IL-6 may be critical in the transition to a chronic inflammatory state (30). Because the sites of FDG accumulation in infectious lesions are located in migratory inflammatory cells such as macrophages (31), high liver uptake may be induced by the inflammatory state of the liver in obese subjects. One previous study reported that inflammation is a primary cause of hyperlipidemia (32). Liver inflammation and fibrosis have both been associated with the presence and severity of MS (33), and therefore, high FDG uptake by the liver indicates more severe MS. Elevated serum γ-GT has been suggested to be a marker of excess fat deposition in the liver. Serum γ-GT is closely related to obesity and visceral fat deposition, and is involved in inflammatory response (343536). However, considering that the chronic, low-active, systemic inflammation related to obesity has been observed primarily in adipose tissue, the speculation that increased liver uptake is caused by inflammation needs to be supported by evidence that inflammation is more active in the liver than in adipose or other tissues in the body. An even distribution of inflammatory activity does not lead to observed differences in regional uptake. In addition, FDG uptake in fat is very low (37). The FDG uptake of non-fatty tissues may be influenced by the distribution and volume of fatty tissue in obese subjects. Given the zero-sum nature of FDG uptake in the body (38), increased non-FDG-avid fatty tissue may result in increased liver FDG uptake, and this may explain the significant correlations between liver FDG uptake and obesity.
Interestingly, waist circumference exhibited a positive, albeit weak, association with brain FDG uptake (Spearman rho rank correlation coefficient = 0.199, p = 0.001) and was also greater in subjects who exhibited normal uptake than in those who had low uptake in the brain regardless of the presence of MS. These results differ from our expectations that the brain would show lower FDG uptake in obese than in non-obese subjects due to insulin resistance; a previous study of 28 obese patients (2) did not detect any differences in brain FDG uptake between obese and non-obese patients (12.6 ± 4.5 vs. 11.6 ± 3.9, p = 0.308). Taken together, it is unlikely that increased waist circumference leads to decreased brain activity, although the extent of correlation between these two factors remains unclear. More studies are needed to clarify this relationship.
In the current study, subjects with pattern 1 had higher values for SBP, waist circumference, FBG, TG, ALT, HbA1c, insulin, HOMA-IR, and BMI, which are all closely associated with cardiovascular risk. Subjects with pattern 1 had high FRS compared with those with pattern 3, although there was no significant difference compared with the values in the pattern 2 subjects. In addition, FRS was negatively correlated with brain (r = -0.183, p = 0.003) FDG uptake and positively correlated with liver (r = 0.122, p = 0.047) FDG uptake. In addition, because subjects with pattern 2 had higher values for various cardiovascular risk factors compared with those with pattern 3, subjects with either low brain or high liver uptake should also be evaluated for cardiovascular disease.
This study had some limitations. First, the study was cross-sectional and retrospective in design and thus could not clarify the causal relationships between brain uptake, liver uptake, and cardiovascular risk factors. Second, only males were included in the study because very few females had undergone general health check-ups at our institution. In addition, the number of subjects 55 years or older (n = 19, 7.2%) was relatively small, which may weaken the findings of this study. Studies with females and more subjects older than 55 years are needed to validate the findings of the present study. Third, the present study only included clinical and laboratory data that were available from general health check-ups at our institution; thus, other factors that could affect glucose metabolism in the brain or liver could have been missed. Despite these limitations, the present study is the first to demonstrate that incidentally concurrent low brain and high liver FDG uptake are associated with various cardiovascular risk factors.
In conclusion, concurrent low brain and high liver FDG uptake were closely associated with MS, and therefore, when this pattern is incidentally found on FDG PET, subjects should be further evaluated for MS. Moreover, subjects with this pattern had higher values for various cardiovascular risk factors compared with those without it, and a longitudinal study is needed to verify whether this FDG uptake pattern is directly related to cardiovascular events.





 XML Download
XML Download