

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Biopsy is a key step in the diagnosis and management of musculoskeletal soft-tissue lesions, even though not all lesions require a biopsy; biopsy is generally recommended for a lesion when its clinical and radiologic features do not suggest a typically benign entity or when it is detected in patients with a history of malignancy. Although surgical excisional biopsy is still considered the gold standard for the ultimate diagnosis, there is a general trend toward using minimally invasive procedures, and percutaneous core needle biopsy (CNB) is gaining favor over surgical excisional biopsy for the initial tissue diagnosis of musculoskeletal soft-tissue lesions (1). In particular, ultrasonography (US) is a guidance system that is most commonly used for obtaining biopsy materials from musculoskeletal soft-tissue lesions because it has many advantages: it is easy to handle; it is usually quicker than any other guidance modality; it provides real-time, multi-planar imaging; and it avoids subjecting the patient to radiation. Performing ultrasound-guided CNB (US-CNB) for musculoskeletal soft-tissue lesions is not much different than non-musculoskeletal lesions, but in some ways, it does require closer collaboration by a multidisciplinary team that consists of a surgical oncologist, medical oncologist, radiation oncologist, and musculoskeletal pathologist with a careful review of all relevant clinical and radiological information. To maximize diagnostic yield and minimize the morbidity of US-CNB, understanding the following considerations is critical: 1) selecting the proper biopsy target in order to yield the most useful specimen; 2) selecting the proper biopsy route in order to avoid damage to important structures and prevent unintended wide excision or local tumor recurrence; and 3) the principles and tips of biopsy techniques. In this article, we hope to provide useful guidelines for applying US-CNB to musculoskeletal soft-tissue lesions.
Selecting the Proper Biopsy Target
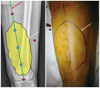
The first objective of biopsy is to obtain diagnostic material. Because musculoskeletal soft-tissue lesions often have heterogeneous imaging features, it is imperative to target the most diagnostic portion of the lesions. Various image modalities can provide important information that can guide the proper selection of the biopsy site, but in general, magnetic resonance imaging is the modality of choice for characterizing soft-tissue lesions. Intravenous gadolinium is useful for identifying solid or more vascular portions in lesions, and these portions are more likely to yield diagnostic specimens than are cystic or necrotic lesions (2). Positron emission tomography images can help guide biopsy in the target areas, which may result in a higher diagnostic yield by indicating the metabolic activity of a lesion. US is gaining wider acceptance as a suitable biopsy modality for soft-tissue lesions and is considered useful for differentiating solid portions from the cystic or necrotic portions of lesions (3). On US, the solid portion usually demonstrates iso- to hyper-echogenicity; however, in the case of a lesion with hemorrhage or a fatty component, the solid portion could show as a relatively hypoechoic area and thus could be confused with the cystic or necrotic portion. Therefore, it is critical to review all imaging studies and compare their results with the US findings (Figs. 1, 2).
Selecting a Proper Biopsy Route
The biopsy must be carefully planned with an understanding of the orthopedic surgeon's perspective, and the optimal biopsy tract should be chosen after considering the location, size, and morphological features of the lesion. It is better to use a shorter path to the lesion, although the shortest distance to the lesion is not necessarily the optimal route (4). The biopsy tract must be placed within the surgical resection margins because the en bloc resection of the tumor, as well as the biopsy tract, is needed to avoid possible tumor seeding along the tract. It is best if the point of needle entry is located along the planned surgery incision (Fig. 3). In addition, the biopsy route should be selected so that the needle does not violate unaffected compartments or neurovascular bundles in order to prevent unintended wide excision, local tumor recurrence, or functional deficits (Figs. 4, 5). Therefore, knowledge of the anatomic compartments and location of the main neurovascular bundle is very important for obtaining a biopsy of any soft-tissue lesions in the extremities.
There are three compartments in the upper leg. The anterior compartment includes the quadriceps muscle group, the iliopsoas, sartorius, and tensor fascia lata muscles, and the iliotibial band. The medial compartment includes the adductor muscle group and the gracilis muscle. The posterior compartment includes the hamstring muscle group (Fig. 6A). There are also three compartments in the lower leg. The anterior compartment includes the tibialis anterior, extensor hallucis longus, and extensor digitorum longus muscles. The lateral compartment includes the peroneus longus and brevis muscles. The posterior compartment can be separated into superficial and deep posterior compartments by the transverse intermuscular septum. The superficial posterior compartment contains the soleus, gastrocnemius, and plantaris muscles. The deep posterior compartment contains the flexor digitorum longus, tibialis posterior, flexor hallucis longus, and popliteus muscles (Fig. 6B). In the upper arm, there are two compartments. The anterior compartment includes the biceps, brachialis, and coracobrachialis muscles, and the posterior compartment includes the triceps muscle (Fig. 6C). The forearm can be described as containing two or three compartments. In the two-compartment description, the anterior or flexor compartment is separated from the posterior or extensor compartment by the radius, ulna, and intermuscular septum. In the three-compartment classification commonly used by surgeons, three muscles–the brachioradialis, extensor carpi radialis longus, and extensor carpi radialis brevis–are considered the lateral compartment (Fig. 6D) (256).
Principles and Tips for Biopsy
Which Type of CNB Should be Used?
The automated needle uses a two-stage spring-deployed action in which the inner stylet is initially propelled forward to expose the specimen notch, and this is followed by an outer cutting cannula (Fig. 7A). These two stages of the biopsy are powerful and fast, making it useful for obtaining biopsy materials from hard or movable soft-tissue lesions. In contrast, the inner stylet of the semiautomated needle is manually advanced (Fig. 7B). However, this movement lacks both force and speed, and only the movement of the cutting cannula over the inner stylet is automated. The manual advancement of the inner stylet allows for more delicate control, but there is a higher probability of distally displacing the lesion, and thus, the cannula may partially cut the lesion, leaving the remaining core tissue as the only adjacent normal tissue (Fig. 7C). Previously published studies compared the semiautomated and automated core needles for obtaining biopsy materials from breast lesions and reported a better diagnostic yield using automated needles. This is likely because breast lesions are usually mobile and more likely to be displaced distally by the force of the biopsy mechanism, especially when the lesion is small (27).
Should an Introducer Needle be Used?
The introducer–which is first inserted near or inside the edge of the lesion–serves as a sheath and enables the user to obtain multiple core samples. It can also minimize soft-tissue damage and contamination by tumor cells during multiple biopsies.
What Gauge of Needle is Suitable?
According to a previous study, there are no differences in diagnostic yield based on needle gauge (8). Generally, a thinner needle is safer and causes less pain, but it is difficult for a thin needle to penetrate a thick or hard-tissue lesion, and thin needles are difficult to control within the tissue. In the case of a calcified or ossified lesion, a larger needle can be more helpful. We suggest an 18-gauge core needle, which is sufficient for most biopsies of musculoskeletal soft-tissue lesions.
What Length of Specimen is Needed?
There are many kinds of biopsy gun systems, and each system has different lengths for the specimen notch. Wu et al. (8) reported a significant increase in diagnostic yield with longer specimens: only 42% of specimens that were < 5 mm in length were diagnostic, as opposed to 82% of specimens that were > 10 mm. On the basis of these results, attempts should be made to obtain longer specimens if possible.
How Many Specimens are Sufficient?
Wu et al. (8) reported that the cumulative diagnostic yield plateaued at four specimens for musculoskeletal soft-tissue lesions. Other analogous studies on breast lesion biopsies found that four samples were needed to obtain a diagnosis in 100% of biopsies (7). On the basis of these results, we suggest obtaining a minimum of four biopsy specimens for musculoskeletal soft-tissue lesions.
Tips for CNB Visualization
When US-guided biopsy is performed on a soft-tissue lesion, the lateral approach (i.e., the in-plane technique) is generally recommended, and the needle is aligned with the small side of the transducer. As a general rule, a finer needle is more difficult to visualize on US than a thicker needle, whereas a thicker needle is more clearly visible and often causes US reverberation or comet-tail artifacts behind the needle. If the needle gauge is the same, the needle is more visible as the incidence angle of the needle to the US beam increases, and the needle can be optimally visualized when the US beam is perpendicular to it (Fig. 8). The needle's incidence angle can be increased by pressing on the opposite side of the transducer rather than controlling the needle: this technique is called the "heel-and-toe" maneuver. For this technique, it is helpful to use a great deal of gel under one end of the transducer (9).
Tips for Obtaining Biopsy Materials from Small and Movable Lesions
Ultrasound-guided-core needle biopsy is now increasingly used on small soft-tissue lesions. This is due to technical advances in imaging that allow early detection of small lesions because of high sensitivity. In fact, obtaining biopsy materials from small lesions could be worrisome because targeting small lesions is technically difficult and the obtained specimens are likely to be inadequate, thus hindering accurate diagnosis. However, according to a previous study, performing US-CNB on musculoskeletal soft-tissue lesions is effective for diagnosis and decision-making even if the lesion is < 2 cm (1). Due to the technical aspects of biopsy, as previously mentioned, small, movable soft-tissue lesions are more likely to be displaced distally by the force of the biopsy mechanism. For successful penetration of a lesion with the needle, it is helpful to aim at the center of a lesion rather than the periphery (Figs. 9, 10). It is also important to embed the tip of the introducer needle into the lesion before deploying the inner stylet (7).
Keep in Mind!
1. For optimal visualization of the needle, increase the needle's incidence angle to the US beam.
2. Regarding the gauge of the core biopsy needle, an 18-gauge needle is sufficient in most cases.
3. Try to obtain longer specimens; diagnostic yield increases with longer specimens.
4. Try to obtain ≥ 4 specimens.
5. The heel-and-toe technique is helpful for clearly visualizing the entire needle.
6. Try to aim for the center of lesion if it is small and movable and do not hesitate to biopsy small lesions.
7. Embed the tip of the introducer needle into the lesion before deploying the inner stylet.
SUMMARY
Ultrasound-guided-core needle biopsy has become a key step in the diagnosis of musculoskeletal soft-tissue lesions. The goal of any biopsy is to obtain adequate tissue for accurate diagnosis while minimizing morbidity. Here, we have presented the principles and tips for diagnostic and safe US-CNB, and we hope these practical guidelines are helpful for performing successful biopsy.









 XML Download
XML Download