

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Calcification is occasionally observed in tumors, regardless of the organ or type of tumor. It is a notable radiologic feature and one that potentially has clinical significance, since the identification of intratumoral calcification facilitates detection of the tumor as well as its differential diagnosis (12). In the abdominopelvic cavity, various kinds of tumors such as, for instance, mucin-producing tumors, 335metastases, gastrointestinal tumors, solid pseudopapillary neoplasms (SPNs), and so on are frequently accompanied by intratumoral calcification (2345). Furthermore, the imaging features of intratumoral calcification also differ according to the type of tumor. However, to date, prior case reports and series regarding intratumoral calcification have each focused on a specific single case or one particular tumor, and no study has addressed this issue comprehensively.
Therefore, in this article, we classify the imaging patterns of intratumoral calcification according to number, location, and morphology of the calcification. In addition, we briefly review the abdominopelvic tumors that frequently exhibit typical patterns of intratumoral calcification. We also describe the imaging features with a focus on the differentiable characteristics of the tumors using the pattern of calcification, together with representative cases.
Intratumoral Calcification and Imaging Modalities
Intratumoral calcification is a type of pathologic calcification. Pathologic calcification is defined as an abnormal calcium deposition in soft tissues. It occurs via two mechanisms: metastatic and dystrophic. Metastatic calcification may be a result of systemic mineral imbalance, such as uremia or hyperparathyroidism; while dystrophic calcification may be a result of tissue injury, aging, disease, or malignancy (67). Thus, intratumoral calcification is usually considered to be dystrophic calcification caused by degenerative changes of the tissue, such as necrosis or hemorrhage, with the exception of a few bone-forming tumors.
Calcification, as it appears on radiographs and CT images, is easily visible as a hyper-dense or radiopaque lesion, because calcification attenuates X-rays (8). In clinical practice, CT is regarded as the gold standard for the identification of calcified lesions (910).
On US, calcification exhibits a hyperechoic appearance, as it contains high-intensity reflectors. Depending on the size and characteristics of the surface structure of calcification, posterior acoustic shadowing may or may not be evident (8). Occasionally, a color Doppler twinkling artifact (color comet tail artifact) is observed because this artifact is generated by a strongly reflecting medium with a rough interface and because most of the calcifications are small and have a rough surface (1112). Therefore, the color Doppler twinkling artifact is a helpful sign for identifying small calcifications and thus can improve diagnostic confidence (12).
On MR, calcification shows various nonspecific signal intensities on conventional spin echo T1- or T2-weighted images (913). Therefore, it difficult to definitively identify the intensities as calcium deposits, and thus small calcifications are easily missed on MR. However, dense calcification typically appears as a signal-void area because it has a very lower water content (8). In a gradient-echo sequence, calcification usually appears as being hypointense and cannot be differentiated from hemorrhage (9).
Imaging Patterns of Intratumoral Calcification
To date, a multitude of descriptive expressions have been used unsystematically to describe imaging patterns of calcification: fine, popcorn, granular, punctate, speculated, eggshell, miliary, and so on. We classify several patterns of intratumoral calcification according to the number, location, and morphology of the calcification (Fig. 1). In general, calcification in tumors can be single (solitary) or multiple, and can be located in the peripheral or the central portion of the tumor or at the internal septa. According to its morphology, intratumoral calcification is classified as having patterns which may be punctate (round), amorphous (irregularly shaped), curvilinear (curved line), or rim (eggshell, cyst-wall like appearance).
Then, based on the imaging pattern of intratumoral calcification, we categorize commonly-encountered abdominopelvic tumors which frequently show a typical calcification pattern as follows: mucinous adenocarcinoma, mucinous cystic neoplasm, metastasis, hemangioma, mature cystic teratoma, and miscellaneous tumors.
Mucinous Adenocarcinoma
Mucinous adenocarcinoma is a rare subtype (10–15%) of adenocarcinoma that usually occurs in the stomach and the colorectum. It is histologically defined as an extracellular mucin pool of > 50% of the tumor volume (214). Mucinous adenocarcinoma of the stomach shows typical CT findings with a thickening of the diffusely low-attenuating middle or outer layer (corresponding to the mucin pool) and a presence of associated multiple, punctate calcifications (9.5%) (Figs. 2, 3) (15). The presence of mucin is thought to act as an ion-exchange resin, and mucin may be an important factor both for calcium deposition within gastrointestinal carcinoma and in its metastasis (31617). Compared with non-mucinous carcinoma, mucinous adenocarcinoma in the colorectum shows more eccentric bowel wall thickening, heterogeneous enhancement, a greater area of low attenuation, and more frequent intratumoral calcification (21%) (2).
Mucinous Cystic Neoplasm
Mucinous cystic neoplasm is currently defined as a cyst-forming epithelial neoplasm composed of mucin-producing epithelium and associated with ovarian-type subepithelial stroma (1819).
Pancreas
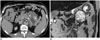
Mucinous cystic neoplasm of the pancreas is a relatively uncommon tumor with a predominance among females (> 95%) and a predilection for the pancreas body or tail (20). If mucinous cystic neoplasm is suspected from imaging, complete surgical excision is advocated–as the tumor has malignant potential. Mucinous cystic neoplasm from the pancreas shares common clinical and pathologic characteristics with mucinous cystic neoplasm that arises in the liver and ovary (21). On cross-sectional imaging, mucinous cystic neoplasm of the pancreas appears as a well-capsulated, unilocular, macrocystic lesion with or without septation or mural nodule (212223). Calcification is found in 10–25% of cases with a peripheral, curvilinear pattern or septal location (Figs. 4, 5) (123). Intratumoral calcification occasionally enables differentiation of mucinous cystic neoplasms from serous cystic neoplasms, which frequently have central calcification within the central fibrous scar (1).
Liver
Mucinous cystic neoplasm of the liver is a rare neoplasm of the biliary system and has been previously referred to as biliary cystadenoma and biliary cystadenocarcinoma (18). It occurs usually in the intrahepatic bile duct (85%), and occurs predominantly among middle-aged females (23). On cross-sectional imaging, mucinous cystic neoplasm of the liver appears as a solitary, well-encapsulated cystic mass with internal septa and/or mural nodules (2324). Intratumoral calcification is rarely found, but was reported in 47% (7/15) of the cases in a recent study (19). It is usually seen within the wall (peripheral) (Fig. 6) and the septa (septal) (Fig. 7) (24). However, calcification can be also seen in intraductal papillary neoplasms and solitary bile duct cysts, which should be differentiated from mucinous cystic neoplasms of the liver (19). Some radiologic features, including the presence of internal septa and solid mural nodules, are more likely to be mucinous cystic neoplasms with invasive carcinoma (biliary cystadenocarcinoma) (25).
Appendix
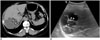
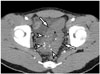
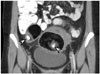
The descriptive term “mucocele” refers to luminal distension of the appendix by the mucin, regardless of the underlying pathology (26). It can be caused by a variety of non-neoplastic, benign neoplastic, and malignant conditions; however, mucinous neoplasm of the appendix is the most common cause of mucocele (23). The WHO classification recognizes 3 main categories of mucinous neoplasm of the appendix: mucinous adenoma, low-grade mucinous neoplasm, and mucinous adenocarcinoma (2728). CT is preferred as the modality of choice because it depicts well the anatomical relationship between the cystic mass and cecum, as well as the tissue characteristics. On CT, an appendiceal mucinous neoplasm appears as a round or tubular cystic mass with an enhancing wall in the expected position of the appendix (Fig. 8) (23). Curvilinear, peripheral (mural) calcification occurs in < 50% of cases (2629) (Figs. 8, 9), and it is highly suggestive of the diagnosis. Soft tissue mass, wall thickening, and irregularity raise the suspicion of malignancy (Fig. 9) (2830).
Metastasis
Intratumoral calcification is also seen in metastatic lesions. First, some metastases may develop calcifications because of the histology of the primary malignancy. Metastasis from mucinous adenocarcinoma most commonly contains calcification with a punctate pattern, similar to the primary lesion (317). Metastasis from other primary malignancies such as papillary thyroid cancer, breast cancer, and chondrosarcoma are rare, but may show calcification (Fig. 10) (3).
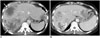
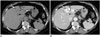
Secondarily, after systemic chemotherapy or radiation therapy, dystrophic calcification can develop in the metastatic lesion. Calcification in colorectal liver metastasis after chemotherapy is occasionally encountered in clinical practice. Calcification in hepatic metastasis shows a variable pattern and distribution (central and peripheral), and may develop or change during therapy (Fig. 11) (31). Calcification in colorectal liver metastasis is generally considered to be a good indicator of the response to treatment (32).
Hemangioma
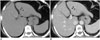
Hemangioma is a benign vascular tumor and is composed of a blood-filled space lined by single or multiple layers of endothelial cells and a thin fibrous stroma (3). In the abdominal pelvic cavity, hepatic hemangioma is the most common. It has the characteristic imaging features of a progressive peripheral to central fill-in enhancement pattern on dynamic imaging (33). Calcification is rarely demonstrated in hepatic hemangioma but is often found in sclerosing hemangioma or giant hemangioma (343536). Calcification in hemangioma is known as a phlebolith, which arises because of thrombosis from inflammation or stasis of blood flow (37). It usually appears as a discrete, rounded pattern (punctate) with a central or peripheral location (Figs. 12, 13) (333435).
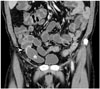
Hemangioma of the gastrointestinal tract is rare, and gastrointestinal bleeding is the most common clinical presentation. Hemangioma may occur anywhere in the gastrointestinal tract; the small bowel is the most frequent site, and the colon is the second most frequent site (38). Most hemangiomas are seen to be pedunculated intraluminal polypoid masses, but occasionally they have an infiltrative submucosal growth pattern (39). In the colon, rectosigmoid is the most commonly involved colonic segment; and colorectal hemangioma shows characteristic imaging features of transmural enhanced bowel wall thickening containing multiple, punctate calcifications (phleboliths) (Fig. 14) (383940). The presence of multiple, punctate phleboliths is the pathognomonic imaging feature of gastrointestinal hemangioma that enables its differentiation from carcinoma (39).
Mature Cystic Teratoma
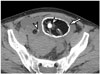
Mature cystic teratoma, also called dermoid cyst, is a cystic tumor of the ovary. The tumor is composed of well-differentiated tissues from at least two of the three germ cell layers (41). Most cases are asymptomatic; however they, can cause acute abdominal symptoms by torsion or rupture of the tumor (42). On CT, fat attenuation within a cyst with or without calcification is diagnostic of mature cystic teratoma (414344). Teeth or other calcifications are frequently seen (56%) (4445). When bone or teeth are present, they tend to be located within the Rokitansky nodule (4146). Thus, intratumoral calcification in mature cystic teratoma usually appears as a single, punctate pattern within the mass (Fig. 15) (4147). Occasionally, it is possible to observe unusual dense rim calcification of the cyst wall (Fig. 16) (464748).
Miscellaneous Tumors
Gastrointestinal Stromal Tumor (GIST)
Gastrointestinal stromal tumor (GIST) is the most common primary mesenchymal tumor of the gastrointestinal tract, and arises from the interstitial cell of Cajal (49). Generally, GIST is defined as a KIT (CD117)-positive tumor with a characteristic histologic feature (50). The radiologic appearance of GIST depends on the tumor size: a small GIST is seen as a well-defined mass with homogeneous enhancement, whereas a large GIST is seen as an exophytic heterogeneously enhancing mass with intratumoral hemorrhage or necrosis (4951). Calcification in a GIST is unusual (3–10%) and it may occur as a punctate pattern (Fig. 17) (515253).
Solid Pseudopapillary Neoplasm (SPN)
Solid pseudopapillary neoplasms is a rare neoplasm of the pancreas that typically occurs in young females (54). The characteristic finding of SPN is a large, solitary, well-encapsulated mass with varying amounts of intratumoral hemorrhage or cystic component (5556). Intratumoral calcification is occasionally associated with SPN; and a peripheral curvilinear, rim (eggshell), or punctate pattern is usually seen (Fig. 18) (5).
Pancreatic Neuroendocrine Tumor (PNET)
Pancreatic neuroendocrine tumor (PNET) is a rare pancreatic neoplasm which demonstrates neuroendocrine differentiation (57). It is classified as functioning or non-functioning by hormonogenesis, and non-functional tumors currently account for the majority of newly diagnostic PNETs (up to 60–80%) (58). On imaging, a functioning PNET is typically found as a small (1–2 cm) hypervascular mass, whereas a non-functioning PNET appears as a relatively larger heterogeneous mass and commonly contains calcification, necrosis, or cystic change (5960). Calcification is found in approximately 20% (30/133) of them, and large tumors were more likely to be associated with calcification regardless of whether they are either functioning or non-functioning tumors (61). The pattern of calcification is very diverse and includes punctate, coarse (amorphous), and multiple pattern (Fig. 19) (6062). Calcification has often been thought to be indicative of a malignant lesion (5862). A recent study, however, found no significant correlation between the calcification and tumor grade (63). Intratumoral calcification can be helpful in differentiating PNET from pancreatic adenocarcinoma, because only 2% of adenocarcinomas show calcification as compared with 20% of PNETs (64).
Neurogenic Tumors
Neurogenic tumor is classified into ganglion cell origin (e.g., neuroblastoma, usually in children), paraganglionic system origin (e.g., pheochromocytoma, paraganglioma), and nerve sheath origin (e.g., neurilemmoma, so called schwannoma) (65). In the abdominal cavity, the tumor usually occurs in the retroperitoneum or the adrenal gland. It commonly appears as a well-circumscribed, smooth, or lobulating mass. Calcification may be seen in all types of neurogenic tumors with various patterns (Fig. 20) (65).
Castleman Disease
Castleman disease is an uncommon, benign lymphoproliferative disorder characterized by hyperplasia of the lymphoid follicles (66). Approximately 70% of cases are located in the thorax; 10–15% in the neck; and 10–15% in the abdomen, retroperitoneum, and pelvis (6768). Castleman disease commonly presents as single, well-circumscribed enhancing mass of varying locations in the abdomen and pelvis. Intratumoral calcification is reported in up to 31% (5/16) of cases of Castleman disease of the abdomen and pelvis (69). A variety of calcification patterns including punctate, peripheral, central, and arborizing patterns can be seen (Fig. 21) (6669). The presence of calcification may help in differentiating Castleman disease from lymphoma, since calcification would be rare in untreated lymphoma (70).
CONCLUSION
Intratumoral calcification exhibits various imaging patterns in various types of abdominopelvic tumors. However, several commonly-encountered tumors have a tendency towards showing typical patterns of intratumoral calcification. Although a specific diagnosis of a precise kind of tumor may not always be possible using only intratumoral calcification, imaging patterns of intratumoral calcification can help to facilitate accurate diagnosis and improve diagnostic confidence with regards to abdominopelvic tumors. Therefore, it is useful to be aware of, and to be familiar with, the imaging patterns of intratumoral calcification in abdominopelvic tumors.












 XML Download
XML Download