

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The neck has neural structures intricately connected to the skull base, cervicothoracic spine, upper extremities, or functional end organs located in the neck. These neural structures include cervical and brachial plexi, the sympathetic system going into the skull base and the bilateral orbit, lower cranial nerves from IX to XII, and their branches. Although the brachial plexus has been intensely investigated with MRI, there has been little research regarding the normal imaging appearance or the corresponding pathologies of other neural structures using CT or MRI probably due to their complex anatomies and small dimensions. However, the development of imaging techniques with better resolution and signal-to-noise ratio can now enable the visualization of tiny neural structures, consequently making it possible to predict complications related to image-guided minimally invasive procedures such as tumor ablation and core needle biopsy that have gained increased popularity as alternatives to surgery. CT and MRI have also been increasingly used in oncology patients before and after treatment or to assess tumor response after chemoradiation therapy and the use of cytostatic drugs. For those purposes, it is important to know the normal findings and pathologic findings of neural structures on CT or MR for better prediction of patient outcomes and management. Therefore, the purpose of this review was to systematically present imaging-based anatomy and landmarks of major neural structures in the neck. By presenting their normal imaging appearance on CT or MRI, their relevant clinical significance and representative pathologies of the regarded nerves in oncology patients before and after treatment are explained in this study.
Imaging Anatomy and Pathologies of the Major Nerves in the Neck
Cervical Sympathetic Trunk
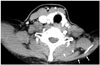
Cervical ganglia are composed of three paravertebral ganglia of the sympathetic nervous system. Superior cervical sympathetic ganglion (CSG), the largest one, is located close to the longus capitis muscle at the level of C2/C3 transverse process. Middle CSG, the smallest one, lies close to the inferior thyroid artery at the level of C6/C7 intervertebral disc. Inferior CSG, the intermediate in size, is 80% fused with the first thoracic ganglion to form a star-shaped enlargement called stellate ganglion. It is located lateral to the longus colli muscle at the level of C7/T1 vertebra (Fig. 1A) (1). Cadaveric studies have revealed that all specimens have the superior and inferior CSGs. Only one-third to less than half of specimens have middle CSGs (2). Injury to the CSG can cause ipsilateral blepharoptosis, pupillary miosis, and facial anhidrosis (also known as Horner's syndrome) (3).
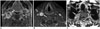
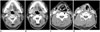
A recent study using 3T-MRI has revealed that 73% of superior CSGs can be identified in medial to internal carotid artery (ICA) and lateral to longus capitis muscle at the level of C2 or C3 vertebra (4) with a 3-dimensional size of 0.5–1.3 cm in width, 0.2–0.6 cm in thickness, and 1.5–4.5 cm in length. Other superior CSGs have positional variations (4), including anterior to longus capitis muscle (18%), lateral to ICA (7%), and posterior to ICA (3%) (Fig. 2). The authors of that study have suggested that intra-ganglionic hypointensity ‘on both T2WI and CET1WI’ as well as their typical location can be used as imaging clues for differentiating SCSGs from retropharyngeal lymph node metastasis (Fig. 3).
The inferior or stellate ganglion can be easily visualized on CT or MR images (5). It is located at the thoracic inlet adjacent to the neck of the 1st rib, lateral to the longus colli muscle, and posterior to the vertebral artery. It is 1–2.5 cm in length, 1 cm in width, and 0.5 cm in thickness (15). Different from the superior and inferior CSGs, the middle CSG has been found in only 41% of normal patients by sonographic studies, in agreement with previous cadaveric results (126). The mean size of the middle CSG is 0.4 cm in width, 0.2 cm in thickness, and 0.9 cm in length. They are mainly located at the C6/C7 level lateral to the common carotid artery (CCA) on ultrasonography (US) corresponding to the posterior position to CCA on CT or MRI (Fig. 4).
Brachial Plexus
The ventral rami of C5–C8 and T1 constitute the brachial plexus that can be divided into roots, trunks, divisions, cords, and terminal branches (Fig. 1B). The brachial plexus gives rise to the motor and sensory innervation to the upper extremities. The five roots are fused to form the upper (C5 and C6), middle (C7), and inferior (C8 and T1) trunks at the level of subclavian artery (SCA) immediately after leaving the interscalene triangle between the anterior and middle scalene muscles. While crossing the clavicle, each trunk is separated into anterior and posterior divisions. The anterior divisions from the upper and middle trunks, the posterior divisions from the upper, middle, and lower trunks, and the anterior divisions of the lower trunk will reunite to form the lateral, posterior, and medial cords around the axillary artery, respectively. After passing the lateral border of the pectoralis minor muscle, these cords are separated into five terminal branches (7).
MRI is the imaging modality of choice to evaluate the anatomy and pathologic conditions of the brachial plexus. Single axial, coronal plane, and sagittal plane are difficult to show the whole course of brachial plexus structures because the image plane is not aligned with the orientation of the brachial plexus. Our standard protocol includes axial T1- and T2-weighted images, coronal T2-weighted images with fat suppression and T1-weighted images, and sagittal T1- and T2-weighted images of the symptomatic side. Oblique planes to the axis of the brachial plexus are not performed because the anatomical relationships are not familiar to radiologists. In addition, the scanograms have to be referred to read the images. Intravenous gadolinium agent is useful in case of tumor. MR myelographic images are reserved for the evaluation of nerve root avulsion or pseudomeningocele. Brachial plexopathy can be caused by trauma, inflammation, neoplastic condition, and extrinsic compression. A neoplastic condition constitutes 60% of non-traumatic brachial plexopathy. It is mostly caused by direct invasion of lymphatic spread from malignant tumors (Fig. 5). Carcinomas of the lung and breast are the most common ones involving the brachial plexus. Lymphoma can involve the brachial plexus in two ways (infiltration of the plexus by affected lymph nodes and by neurolymphoma, i.e., primary lymphoma of the peripheral nerves) (Fig. 6) (8). It is often difficult to differentiate between recurrent tumor and radiation-induced plexopathy in patients with history of cancer and clinical evidence of plexopathy following radiation therapy. Typical radiation-induced plexopathy is usually low on T1- and low or high on T2-weighted images showing diffuse thickening of the plexus with various degrees of enhancement of the intravenous contrast agent (Fig. 7). Tumors have various signal intensities according to primary tumors. They are usually enhanced by a contrast agent, showing irregular or nodular thickening of the plexus or accompanied by a focal or infiltrative mass (Fig. 8) (910).
Cervical Plexus
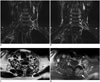
The ventral rami of the first four cervical spinal nerves constitute the cervical plexus. They are located in front of the C1 to C4 vertebra, deep and posterior to the sternocleidomastoid muscle (SCM), anterior to the middle scalene muscle, and posterolateral to the longus capitis muscle (Fig. 9). The cervical plexus has cutaneous and muscular branches. Cutaneous branches innervate the skin surrounding the auricle (greater auricular but lesser occipital nerves), neck, and clavicle (transverse cervical and supraclavicular nerves). Muscular branches innervate the infrahyoid muscles (except for the thyrohyoid muscle) and the diaphragm (phrenic nerve) (7). Axial T1-, T2-, and contrast-enhanced T1-weighted images of thin slices (< 3-mm in thickness/no gap) should be used to find their locations due to the small diameter of the branches from the cervical plexus and accompanying venules or arterioles.
The greater auricular nerve is the largest ascending cutaneous branch of the cervical plexus. Arising from the ventral rami of C2 and C3, it goes to the posterior edge of the SCM. After wrapping around the edge of the SCM, it ascends on the outer surface of the muscle beneath the platysma after perforating the deep cervical fascia (7). After passing to the parotid gland, it is divided into two branches innervating the facial skin over the parotid gland (“anterior branch”) and the skin over the mastoid process on the back of the auricle (“posterior branch”) (Figs. 10, 11).
The supraclavicular nerves arise from a common trunk formed from rami from C3 and C4 nerves. They emerge at the posterior border of the SCM. The trunk descends under the platysma and the deep cervical fascia. It is divided into branches that diverge to pierce the deep fascia above the clavicle slightly. It supplies the skin over the clavicle, upper chest, and part of the shoulder (7).
The phrenic nerve arises chiefly from the C4 ventral ramus. It also receives contributions from the third and fifth cervical nerves. It is formed at the upper part of the lateral border of the anterior scalene muscle. It descends almost vertically across its anterior surface behind the prevertebral fascia (Fig. 12) (7).
The signs and symptoms of cervical plexus damage can vary depending on the severity and the location of the involved nerves. After neck dissection, traumatic neuroma usually arises from injury to the peripheral sensory nerves of the cervical plexus as a reparative process at the proximal end of the transected nerve (1112). It can be confused with a metastatic lymph node, especially on US. However, identification of the direct continuity of the transected nerve can easily verify a traumatic neuroma, thus avoiding unnecessary biopsy (Fig. 13) (12).
Vagus Nerve
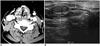
The vagus nerve is the longest cranial nerve. It has the widest distribution in the body. It contains parasympathetic, motor, sensory, and taste fibers. The vagus nerve exits the skull base through the pars vascularis of the jugular foramen. It courses downward within the carotid space, mostly posterolateral to the ICA, and then to the CCA and posteromedial to the internal jugular vein (IJV) (Fig. 14A) (13). The vagus nerve has two marked enlargements, including a smaller superior ganglion located in the middle of the jugular foramen and a larger inferior ganglion located at the level of the transverse process of the C1 vertebra (714). The superior ganglion is spherical and approximately 4 mm in diameter. The inferior or nodose ganglion is elongated and cylindrical in shape with a length of approximately 2.5 cm and a maximum width of 5 mm (Fig. 15) (7). Running down the neck to the level of the thyroid gland, the vagus nerve can change its position relative to CCA. According to US studies, the vagus nerve has anatomical variations in its course (from lateral to anterior in 4.3–21.1% of cases and from lateral to medial in 1.2–1.6% of cases) (1315). In one study, there was even posterior variation of vagus nerve in 0.3% of the patients (Fig. 16) (13).
The branches of the vagus in the neck are meningeal, auricular, pharyngeal, carotid body, superior, and recurrent laryngeal nerves cardiac branches. The vagus nerve enters the thorax after descending posterior to the IJV to cross anterior to the SCA on the right side and between the CCA and SCA (behind the brachiocephalic vein) on the left side.
After arising from the vagus in the neck, the superior laryngeal nerve descends by the side of the pharynx medial to the carotid sheath. It is divided into two branches that are approximately 2–3 cm above the thyroid gland (7). The external branch is accompanied by the superior thyroid artery and its branch while the internal branch is accompanied by the superior laryngeal artery. The external branch gives rise to motor innervation to the cricothyroid muscle, enabling sound pitch increase by tensing the true vocal cord. The internal branch pierces the thyrohyoid membrane with the superior laryngeal artery and receives sensory fibers from the hypopharynx and supraglottic larynx.
The recurrent laryngeal nerve gives rise to motor innervation to all intrinsic muscles of the larynx except for the cricothyroid muscle as it receives sensory fibers from the larynx below the vocal cord. The nerve loops under the SCA on the right side and the aortic arch on the left side. It then travels upwards in the tracheoesophageal groove posteromedial to both lobes of the thyroid. Both nerves finally enter the larynx by penetrating the thyrohyoid membrane at the level of the cricothyroid joint (Fig. 17).
Non-recurrent laryngeal nerve is a rare anatomical variation with 0.5–0.6% of cases on the right side and 0.04% of cases on the left side (1617). A right non-recurrent laryngeal nerve is associated with aberrant right SCA while a left non-recurrent laryngeal nerve is associated with situs inversus. As non-recurrent laryngeal nerve directly goes into the larynx along with the superior or inferior thyroid artery, it is important to recognize the presence of a non-recurrent laryngeal nerve before thyroidectomy or cervical spine surgery using an anterior approach in order to avoid incidental injury to the nerve (Fig. 18) (1819).
Spinal Accessory Nerve
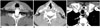
The spinal accessory nerve has two components (the cranial root and the spinal root). However, it conveys pure motor innervation to both SCM and the trapezius muscle in the neck as the cranial root separates from the spinal root immediately after exiting the jugular foramen anteromedial to the IJV via the pars vascularis and joins the vagus nerve superior to the inferior vagal ganglion (Fig. 14A). The spinal accessory nerve runs posterolaterally to enter the posterior cervical triangle crossing the IJV at the level of the posterior belly of the digastric muscle. Approximately 80% of spinal accessory nerves cross the IJV anteriorly while the remaining 19% of spinal accessory nerves cross the IJV posteriorly (20). The spinal accessory nerve keeps coursing inferiorly and posteriorly into the posterior neck deep into the SCM. It is superficial to the levator scapulae muscle. It terminates in the trapezius muscle (Fig. 14B). It is practically impossible to see the nerve on conventional CT or MRI. However, it can be consistently detected between the trapezius muscle and the levator scapulae muscle by US (21). More than 90% of spinal accessory nerve injuries are of iatrogenic causes such as neck dissection surgery (either intentional or non-intentional) and excisional biopsy of a lymph node due to its close vicinity to cervical lymphatics at cervical levels II, III, and V (Figs. 19, 20) (2223).
CONCLUSION
CT and MRI are feasible modalities for evaluating major nerves in the neck and associated pathologic conditions. Knowledge of CT- and MRI-based normal neural anatomy and adjacent relevant landmarks of the neck can avoid complications related to iatrogenic procedures. Understanding the clinical features of nerve damage can assist in the identification of the underlying pathologic process involving neural structures in the neck.














 XML Download
XML Download