

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Recently, important improvements in the era of diagnostic imaging technology have been made. However, percutaneous core liver biopsy is still used as a confirmative diagnostic method of diffuse liver disease, as well as focal liver lesions (1). In general, more accurate and reliable the pathology results are obtained with more biopsy specimens of larger size (23). However, the size and the number of biopsy specimens to be taken are limited because of the concern for bleeding complication, especially for patients with bleeding tendencies (coagulation defects, decreased platelet counts, or large amounts of perihepatic ascites and etc.).
Many efforts have been made to prevent bleeding complications after hepatic core needle biopsy. These included 1) biopsy through a transjugular route (4); 2) embolization of endogenous or exogenous materials along biopsy tract (5678910); and 3) thermal ablation of biopsy tract using radiofrequency (RF) energy (111213). Several experimental studies of RF ablation have demonstrated promising results of post-biopsy bleeding control (11121314). However, clinical adoption of these techniques has been slow, perhaps because the devices including RF electrode used are mostly designed for only experimental aim and are limited to use in clinical settings.
This study was based on our 10 years of experience performing percutaneous ultrasound (US)-guided RF ablation procedures for hepatocellular carcinoma with the assistance of artificial ascites. Our earlier studies showed that sufficient coagulation of the RF electrode path would minimize the possibility of bleeding, even in patients with artificially infused ascites (15). Currently, large amount of ascites is no longer a contraindication for percutaneous RF ablation for hepatic tumors in our institution.
A new RF device for coagulating the biopsy tract is the collective result of previous studies. The combination of insulation sheath and biopsy needle can be used in a coaxial manner during biopsy. Monitoring the temperature of electrode tip using thermocouple facilitates appropriate hemostasis (12). It is also compatible with a commercially-available biopsy needle and an RF generator. Thus, the purpose of the present study was to demonstrate, in an in vivo porcine model, the pre-clinical efficacy of the biopsy tract ablating device for producing hemostasis after core biopsy of the liver, even in the situations with bleeding tendency and when using a 16- and 18-gauge core needle.
MATERIALS AND METHODS
Animals and Animal Preparation
This study protocol was reviewed and approved by the Institutional Animal Care and Use Committee (IACUC No. 20130311001) of the Samsung Biomedical Research Institute. All applicable institutional and/or national guidelines for the care and use of animals were followed. Five female domestic pigs weighing approximately 60 kg each were included as study animals. One pig was used for preliminary study and the others were allocated into one of two groups i.e., non-heparinized group (n = 2), or heparinized group (n = 2).
Each pig was anesthetized with an intramuscular injection of 5 mg/kg of zolazepam-tiletamine (Zoletil; Virbac Laboratories, Carros, France) and 0.5 mg/kg of xylazine hydrochloride (Rompun; Bayer, Leverkusen, Germany). Endotracheal intubation was performed. Anesthesia was maintained with mechanical ventilation using inhaled isoflurane gas (Forane; JW Pharmaceuticals, Seoul, Korea) at a 2% concentration for adequate effect. All pigs were placed in a supine position and a laparotomy was performed to expose the livers through a subcostal incision. Two ground pads connected to a generator were attached bilaterally at the hips before the start of the experiment.
Blood samplings were performed once before the experiment in the non-heparinized group. In the heparinized group, a heparin bolus of 300 U/kg was administered intravenously just after laparotomy (1214). Blood samples were taken before and after heparin administration. A total of six samples were tested for red-blood cell count, hemoglobin level, hematocrit level, platelet count, prothrombin time, and activated partial thromboplastin time (aPTT).
Biopsy-Tract Ablator Design
The needle tract ablator made from the company (STARmed, Goyang, Korea) was composed of two main parts including an insulation sheath and an electrode connected to a multi cable (Fig. 1). The insulation sheath was made of stainless steel and coated with a polyester film marked 1-cm interval. The insulation sheath was 13-cm long. The outer diameter of the insulation sheath was either 17-gauge for an 18-gauge biopsy needle or 15-gauge for a 16-gauge biopsy needle. It can be used as both a trocar during biopsy and an insulation sheath during traction ablation.
The electrode was made of stainless steel without coating. The electrode was 14-cm or 15-cm long and the active tip length was 1 cm or 2 cm when combined with the insulation sheath. A thermocouple was embedded within the tip of electrode. The multi cable with the connector, which is available for delivering energy and receiving thermal information, connects the electrode to the generator.
Preliminary Study to Determine Adequate Ablative Options
A preliminary study was performed with one pig to determine adequate parameters for tract ablation, including active tip length, ablation power (W), and temperature of electrode tip. After acquiring one core needle biopsy specimen, we tested under various combinations at the following settings: electrodes with 1- and 2-cm active tip lengths and ablation power ranging from 10–40 W. We performed all the tract ablation keeping the temperature of the electrode tip within the range of 70–80℃ to avoid insufficient ablation or causing immediate excessive collateral tissue damage, as established in a previous study (12). The preliminary study established ideal parameters for bleeding control by visual inspection without quantitation.
Study Design
Four pigs were assigned to each category according to whether they underwent heparinization and the caliber of the biopsy needle, either an 18- or 16-gauge. In each pig, 28 US-guided core-biopsies were performed under control (no tract ablation, n = 14) and experimental (tract ablation, n = 14) settings.
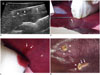
One of the authors (with > 7 years' experience in abdominal imaging and US-guided interventional procedures) performed all biopsies using an automatic side-cutting core biopsy needle (ACECUT; TSK Laboratory, Tochigi, Japan). All biopsy procedures were performed under US-guidance (Accuvix A30; Samsung Medison, Seoul, Korea) to make ensure no large vessels or previous biopsy tract along the current biopsy needle path that would affect the results (Fig. 2A). Control and experimental biopsies were coupled, so that after a control biopsy, the corresponding experimental biopsy was performed close to the control puncture site with tract ablation, in order to avoid location and vascularity bias. A combination of biopsy gun and an insulation sheath were inserted 3 cm into the liver (Fig. 2B). The depth of biopsy gun from the liver surface was checked by reading the marking on an insulation sheath; the biopsy gun automatically advanced 2 cm out from the tip and collected the core specimen. One piece of core specimen was obtained for each puncture site in a coaxial manner as using the insulation sheath as a trocar. All procedures were performed within two hours after heparin injection without additional heparin administration in each pig.
For the control group, the core biopsy needle and the insulation sheath were removed together after biopsy. Any blood from the site was soaked up with dry gauze pads for five minutes without touching the needle tract (Fig. 2C). Bleeding amount was assessed by weighing the gauze pads before and after soaking with blood (121314). A scale (Micro Weighing Scale; CAS, Seoul, Korea) that could measure up to three-digit decimals of a gram was used. If the bleeding did not stop within five minutes, it was controlled using the Electrocauterization Unit (Force FX™ Electorsurgical Generator; Covidien, Boulder, CO, USA). After measuring the amount of blood loss, the operator cleaned the surface of the liver using dry gauze pad to avoid contamination of the results. If there was no bleeding along the biopsy tract for 2 minutes, the operator performed the next biopsy at another site (Fig. 2D).
For the experimental group, after biopsy needle removed, an electrode was inserted into the insulation sheath and the active tip length was 2 cm when combined with the insulation sheath. We used a 200-W generator (VIVA RF System; STARmed). The needle tract was ablated with 40 W of power, based on findings from the preliminary study. The operator monitored the temperature displayed in the generator, and retracting the electrode when it reached 70℃. Thus, the temperature was maintained within 70–80℃ by iterative pulling and staying of the electrode in combination with the insulation sheath. Tract ablation took about 10 seconds. Assessing blood loss in the experimental group was same, as described for the control group.
RESULTS
Optimal Parameters for Tract Ablator from the Preliminary Study
Bleeding control and maintenance of hemostasis occurred most effectively with the following ablation parameters: 2-cm active tip length, 40 W of power, and an electrode-tip temperature range of 70–80℃ during tract ablation. These ablation parameters were then used for the experimental phase.
The RF electrode with a 1-cm active tip was not effective for maintaining the temperature within 70–80℃ during ablation period. The temperature of the 1-cm electrode tip dropped shortly when extracting the electrode and reached 100℃ soon after the electrode was placed. The overheating of the electrode resulted in carbonization of the electrode surface and adhesion to the surrounding tissues. To avoid overheating of the electrode, the operator attempted to withdraw it in haste; however, this did not allow sufficient time to acquire effective coagulation. On the other hand, keeping the temperature within the stable range of 70–80℃ was easier with the 2-cm active tip than the 1-cm active tip.
Comparison of Bleeding Amounts between the Control and the Experimental Group
Table 1 represented the results from laboratory tests before and after intravenous administration of heparin. After heparinization, two pigs (No. 3 and 4) acquired a bleeding tendency, which prolonged the aPTT level. All other results from the laboratory tests were within the normal range.
Blood loss for each liver biopsy with either 18- or 16-gauge needles in the tract ablation and non-tract ablation groups within each non-heparinized and heparinized pig were summarized in Table 2. In the two non-heparinized pigs, bleeding amounts in the experimental group were smaller than those in the control group, although the difference was only significant for the pig that received the 18-gauge biopsy needle (p < 0.001). In two heparinized pigs, the bleeding amounts in the experimental group were significantly smaller than those in the control group (p < 0.001). In the heparinized pigs, the mean amount of bleeding in the experimental group was 3.5% of the controls using an 18-gauge needle (experimental group vs. control group = 0.066 g vs. 1.862 g) and 13.5% of the control group using a 16-gauge needle (0.286 g vs. 2.120 g).
DISCUSSION
The present study was based on our earlier finding that hemostatic effects of the RF electrode path minimizes the possibility of bleeding, even in patients with bleeding tendencies or artificially infused ascites during the hepatic tumor RF ablation (15). The result from the present study demonstrates hemostatic effect by thermal cauterization of the biopsy tract using RF energy, corroborating previous reports (11121314), as well as in cases with high bleeding risk, including anti-coagulated status and use of a large bore (16-gauge) biopsy needle. Pritchard et al. (13) found that RF ablation after liver biopsy reduced bleeding by 63% in the non-heparinized pig model. In another study published by Laeseke et al. (12), mean blood loss after biopsy tract ablation was 0.1% in non-heparinized and 60% in heparinized pigs after non-tract ablation. In this study, mean blood loss after tract ablation, even in the heparinized pigs after non-tract ablation was 3.5% and 13.5%, using either the 18- or 16-gauge biopsy needle (17- and 15-gauge insulation sheath), respectively.
Many studies have been revealed effective hemostasis with embolization along the biopsy tract. Allison and Adam (5) reported their experience using steel coil under fluoroscopic guidance. Animal experimental studies using fibrin sealant for hemostasis also showed no significant bleeding complications (58). Several studies have explored embolization of gelatin particles and sponges under US and/or fluoroscopic guidance (7910). However, Choi et al. (14) reported that RF ablation was the most useful bleeding reduction method in terms of the amount of bleeding and procedure time, among embolization using an absorbable gelatin sponge, and a Histoacryl-Lipiodol mixture plugging after splenic core needle biopsy. While their experiment was conducted on splenic biopsy in a dog model, the result was not expected to differ from the current study.
A new biopsy tract ablator is feasible for even percutaneous clinical application. After acquiring the sufficient core specimens in a coaxial manner, one can change the biopsy needle with the RF electrode through the insulating sheath, allowing thermal coagulation of the biopsy tract by slowly retracting the assembled insulating sheath with the RF electrode. Previous studies (161718) demonstrated that the local temperature for optimal ablation was maintained between 60 and 100℃, with nearly instantaneous tissue coagulation necrosis. If the tissue temperature increases over these values during the procedure, tissue carbonization and adhesion are possible around the electrode. In addition, it is difficult to retract the electrode smoothly. Unlike usual RF device for tumor ablation, this device does not contain a cooling system in the electrode. Thus, the operator has to monitor the temperature of electrode tip for adequate hemostasis.
To date, the molecular-biological information in the treatment of hepatic malignancy has not impacted treatment decisions. However, in the era of molecular and personalized medicine, clinical needs for tissue acquisition before any treatment will be increased for genetic analysis to easily risk-stratify patients, identify dominant oncogenic pathways, and institute-targeted and curative therapies in the near future (1920). Thus, the amount of tissues needed for genetic analysis increases and requires more core tissues from biopsy. Ablation with this new biopsy tract ablator results in adequate hemostasis, as well as avoidance of unnecessary hepatic capsule puncture, thus saving time from needless US-guidance from the skin via co-axial technique during the procedure. Other advantages from the co-axial technique of hepatic core biopsy and the thermal ablation of needle tract have been reported. Two recent studies (2122) have shown that they may be helpful to prevent the needle tract tumor implantation. However, this was not addressed in the current study.
This study had several limitations. First, we obtained a single core specimen from one puncture. While, in actual clinical settings, ≥ 3 biopsies are obtained at an anatomical site. Greater number of biopsy cores would result in increased difference in the bleeding amount between the groups. Second, all procedures performed in this study were conducted in an intraoperative setting to accurately compare the efficacy of the RF biopsy tract coagulator in maintaining hemostasis. Thus, we could not explore the influence on hemostasis of overlaying tissues (i.e., skin, muscle, and fat) or position changes that tend to compress the biopsy site, which may play an important role in maintaining hemostasis in clinical settings. In addition, comparison of delayed bleeding or imaging studies between the two experimental groups was not available. Finally, only one pig was allocated to each experimental setting, which limits the ability to distinguish between statistical trends and individual variation.
In conclusion, the results from the in vivo porcine model experiments indicated that the new RF device for coagulating the biopsy tract may be effective at controlling post-biopsy bleeding, even in the anti-coagulated state and when using a larger (16-gauge) core biopsy needle.



 XML Download
XML Download