

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The anterior cruciate ligament (ACL) is the most frequently reported injured knee ligament that requires surgical reconstruction. ACL injuries most commonly occur in athletes playing multidirectional sports (12). Imaging is frequently used to evaluate complications in patients with postoperative symptoms. Hence, radiologists should be familiar with the normal postoperative appearance and complications that can be diagnosed with imaging. The purpose of this article is to review brief surgical techniques, surgical navigation terminology, and anatomic positions of tunnels and fixation devices. We also review procedure-related radiographic and CT imaging findings after ACL reconstruction with examples of measurements and abnormal findings in the post-operative phase.
Surgical Techniques and Surgical Navigation Terminology
Surgical Techniques
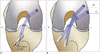
The ACL consists of two major functional bundles: the anteromedial (AM) bundle and the posterolateral (PL) bundle. The bundles are named according to their insertion on the tibia. Both contribute substantially to the anterior and rotational stability of the knee. The AM bundle is inserted more anteromedially on the tibia and originates more proximally on the femur than the PL bundle (345). The two bundles run parallel on knee extension during which the AM bundle loosens and the PL bundle tightens; and cross on knee flexion, when the AM bundle tightens and the PL bundle loosens (Fig. 1) (678). The PL bundle also tightens during internal and external knee rotation (6).
Single-bundle, double-bundle, and selective single-bundle augmentation techniques are widely practiced in ACL reconstruction (Fig. 2) (9). A single-bundle reconstruction is performed by producing one single femoral tunnel and one single tibial tunnel, with focus on reproducing the AM bundle. The selective single-bundle augmentation reconstruction is focused on AM or PL bundle repair with preservation of the remaining intact bundle, while the double-bundle reconstruction uses two separate grafts to replace the positioning of both the AM and PL bundles (9). An anatomic double-bundle, four-tunnel reconstruction using the double-bundle technique has the potential to restore the biomechanics of the knee better than the classic single-bundle, two-tunnel technique (Fig. 3) (10). However, similar long-term results for both techniques are reported in a previous study (11). The double-bundle and single-bundle techniques, aim to place the tunnels in the anatomically correct insertion sites of the native ACL on the femur and tibia, respectively (1213). A recent systematic review (14) comparing single- and double-bundle ACL reconstructions shows that double-bundle reconstruction has fewer re-ruptures and less anteroposterior and rotatory laxity, while complications of double-bundle and selective single-bundle augmentation ACL reconstructions such as graft disruption, graft impingement, arthrofibrosis, hardware failure, and dislodgement are similar to those of single-bundle reconstructions (4).
Surgical Navigation Terminology
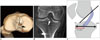
Since surgery is performed with the knee in flexion, surgical terminology differs from anatomical terminology (Fig. 4). The following are the most commonly used terms for navigating in the femoral intercondylar notch: shallow or deep and high or low and should avoid confusion with anatomical position.
Measurements of Tunnel Positions: Imaging-Based Methods
Malpositioning of the bone tunnels is considered as one of the most common technical errors in ACL reconstruction (15). It is estimated that up to 80% of technical failures are based on improper tunnel placement (16). When used, radiographic and three dimensional CT measurements show reliable correlation with anatomic dissection measurements of ACL insertion sites (17).
Femoral Tunnel
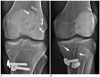
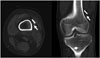
In anatomic single-bundle ACL reconstruction, the femoral tunnel is placed at the site of insertion of the native ACL. Correct tunnel positioning is essential for an optimum clinical outcome in all these techniques (18). Blumensaat's line and "Bernard and Hertel grid" are commonly adopted radiographic markers to determine the location of the tunnels in the distal femoral shaft (19). In this grid-based technique, the optimal placement for deep-shallow direction has a ratio of 24 to 27%. For the optimal placement for the high-low direction, a ratio of 28 to 34% is proposed (Fig. 5A) (2021). A superficial placement is the most frequent malposition of the femoral tunnel (22). The angle measured between a line drawn along the femur diaphysis and the femoral tunnel angle must be approximately 39°. Angles of approximately ≤ 17° are associated with rotational instability (Fig. 5B) (2324).
Tibial Tunnel
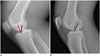
The single-bundle graft is required to provide both anterior-posterior and rotational (pivotal) stability. The optimal placement is within the anatomic footprint (Fig. 6A). On coronal plane, its center should enter the intercondylar notch 2–3 mm posterior to the normal distal ACL insertion on the tibial plateau (Fig. 6B) (25).
The Amis and Jakob line is one of the most commonly used methods to evaluate the anterior-posterior direction of the tibial tunnel (Fig. 6C), which passes through the widest part of the posterior corner of medial tibial plateau, parallel to the medial joint line (20). The measurement originally performed on a mid-sagittal MR image is reported at around 43%. Normal values range between 27 and 60% (2026). The entire opening of the tibial tunnel must be located dorsally to the line drawn along the Blumensaat's line (Fig. 6C) (27). When the femoral tunnel is drilled through the tibial tunnel, it is recommended to drill the tibial tunnel at an angle of 65 degrees to 70 degrees in the coronal plane (Fig. 7) (27).
Multi-Detector CT Evaluation
Recent advances in multi-detector CT technology facilitate the acquisition of isotropic data in nearly every CT examination. Multi-detector CT technology has the ability to create multi-planar reformation and volume rendering for the creation of three-dimensional images. Post-processing methods after ACL reconstruction surgery vary because of differences in available equipment and personal preferences. CT scans and three-dimensional volume rendering images are more reliable in assessing postoperative bone tunnel placement following ACL reconstruction than standard radiographs (28). We create orthogonal coronal and sagittal plane reformat images and two volume rendered images for radiological assessment of tunnel position. To access femoral tunnel location, a volume-rendered image of lateral view on the lateral femoral condyle (Fig. 5A) is reconstructed. Tibial tunnel placement is intuitively recognized on cranial view of the tibia's volume rendered image (Fig. 6A) (2428). Although bone tunnel widening is usually assessed with plain radiographs, CT reconstructions aligned along the axis of the bone tunnel are helpful for follow-up in tunnel widening, especially when multiple tunnels exist e.g., after revision surgery (Fig. 8) (29).
Abnormalities in the Early Post-Operative Imaging
Deviations from the Optimal Location
When femoral tunnel placement is too shallow and too high, the graft is taut in flexion. If tunnel placement is too high, the graft may overstretch in extension and reduce the range of motion (Fig. 9) (24). If the tibial tunnel position is too anterior, it might result in pathological impingement of the ACL onto the notch roof, resulting in extension deficit. In contrast, if the tibial tunnel position is too posterior, it might result in persistent instability (Fig. 10) (30). Rotational instability is associated, if the tibial and femoral tunnels are too steep. Femoral tunnel angles < 17° and tibial tunnel angles > 72° are indicative of an unstable knee joint (Fig. 7B).
Abnormal Findings at Fixation Site
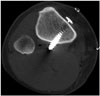
Hamstring grafts are fixed with a device (like a button) to suspend it at the femur and a screw (for instance bioabsorbable screw) to fix it in the tibia. The EndoButton (Acufex Microsurgical, Mansfield, MA, USA) is one of the most often used materials for fixation in recent years. Although it achieves a rapid and secure fixation, button style extra-cortical fixation device can slide into the tunnel (Fig. 11) (31). Possible interpositioning of tissue between extra-cortical devices and the cortex has no effect on the long-term outcome (Fig. 12) (32). Patellar tendon grafts are usually fixed with two interference screws, as they have bony attachments at each end. Since migration of screw is a potential complication of radiolucent "bioabsorbable" interference screws (33), radiologists should carefully examine postoperative images (Fig. 13).
Tunnel Widening
Tunnel enlargement after ACL reconstruction is a well-known phenomenon that predominantly occurs during the first six months after surgery, and represents a potential problem for revision surgery (34). Early post-operative imaging is used as a baseline for future reference. Because tunnels are originally drilled with a bore, the tunnels should have parallel walls. Any change in parallel walls (into a cone shaped tunnel) should raise suspicion of tunnel widening. Tunnel widening can be defined as postoperative enlargement > 2 mm on antero-posterior or lateral radiographs (Fig. 14) (35).
Intramuscular Location of a Screw Tip
Protrusion of screw tip into calf muscles can cause indentation and popliteal area pain. Intramuscular location of a screw tip may be detected in routine post-operative CT scan (Fig. 15).
Divergence
Interference screws provide the most secure fixation in the immediate postoperative period, and the optimal orientation of the screw within the tunnel for maximum fixation strength is parallel to the graft. If the screws diverge or converge, fixation strength may be compromised. The divergence angle is the angle between a line drawn down the long axis of the screw and a line drawn down the long axis of the tunnel (Fig. 2A), and should not exceed 15 to 30° (36).
Miscellaneous
Any case resulting in intra-operative bone fractures can be fixated during the operation or can heal spontaneously without complication. Although, few reports describe tibial plateau fracture complicating ACL reconstruction after 7 to 18 months postoperatively and are induced by torsional trauma (37). Although aseptic wound healing problems can be managed without revision of ACL, septic arthritis after ACL reconstruction is a rare but potentially devastating complication. The correct diagnosis relies on clinical evaluation, laboratory tests, synovial fluid analysis, and bacterial culture. The infection can be successfully managed with early diagnosis and prompt treatment (38).
Summary
Given the increasing number of patients undergoing ACL reconstruction, it is imperative for radiologists to be familiar with these procedures and the associated abnormalities. In addition, adhering to recommended assessment criteria, measurements, and terminology is crucial. Early, post-operative radiographic and CT images are easy to obtain and provide good information regarding tunnel position, bony structures, and fixation devices. Imaging serves as a baseline examination for further follow-ups, helps avoid confusion, and increases the usefulness of the reports.









 XML Download
XML Download