

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Recently, whole-body integrated magnetic resonance/positron emission tomography (MR/PET) systems have been introduced in the clinical routine (1). Major advantages of MR/PET over PET/CT are the improved soft-tissue contrast, motion correction, alignment quality, bone marrow evaluation and the reduced radiation exposure with potential improvement of care in cancer patients (234567). In oncologic whole-body imaging, the evaluation of pulmonary lesions plays an important role for staging and treatment decisions. This raises the question of MR/PET performance for the evaluation of lung nodules in cancer patients, in comparison to PET/CT.
State-of-the-art MRI lung protocols comprise fast T1-weighted three-dimensional (3D) gradient-echo sequences, fast spin-echo T2-weighted sequences and steady-state gradient-echo sequences (89). In recent years, MR sequences with radial stack-of-stars trajectory indicated promising fields of applications also in MR/PET (1011). However, to date, the scan times of radial sequences are within the range of minutes. Thus, depending on the individual diagnostic task, a thoracic MR protocol may still last up to 20–30 minutes (8). Due to the limited MR acquisition time in oncologic whole-body MR/PET imaging, it is desirable to use a sequence type that offers high spatial resolution for lung lesion detection and large scan volume coverage in a short time. For these reasons, modified breath-hold 3D gradient-echo MRI sequences were established (121314) with different acronyms depending on the vendor (T1-weighted volumetric interpolated breath-hold examination [VIBE], T1 high resolution isotropic volume excitation or liver acquisition with volume acceleration). In contrast to the above-described sequences, the 2-point Dixon sequence obtained for attenuation correction (AC) of the PET data in whole-body MR/PET has also been proposed for anatomical allocation of lung lesions (15).
For PET/CT, it was demonstrated that the best co-registration quality between PET and CT can be achieved under expiration, under mid-suspend breath-hold or under shallow breathing (16171819). Thus, an additional chest CT scan in inspiration (CTin) is frequently performed in oncologic PET/CT examinations because the detection rate for small pulmonary lesions can be significantly improved, as compared to a CT scan in expiration alone (17).
Therefore, the aim of the study was twofold: primarily, to investigate the diagnostic performance of fast T1-weighted sequences for pulmonary nodule evaluation in oncologic MR/PET patients. Second, to evaluate the influence of image acquisition in inspiration and expiration breath-hold on diagnostic performance.
MATERIALS AND METHODS
Patients
The study was approved by the local Institutional Review Board. All patients gave written informed consent. Retrospective analysis of datasets of 44 oncological fluorodeoxyglucose (FDG)-MR/PET patients who underwent a clinically indicated PET/CT with subsequent voluntary MR/PET was performed (16 female; mean age, 55 ± 15 years). Inclusion criteria were PET/CT and MR/PET examinations on the same day with coverage of the lung, oncological referral with fluorine 18 (18F)-FDG as radiotracer, CT in inspiration in PET/CT, VIBE in inspiration and expiration in PET/MR. Details for patient flow were given in Figure 1. Clinical indication for PET/CT was staging or follow-up of the following diseases: lung cancer (n = 10), melanoma (n = 11), thyroid cancer (n = 9), lymphoma (n = 3), oesophageal cancer (n = 2), sarcoma (n = 2), cancer of unknown primary (n = 2), tongue carcinoma (n = 1), oropharyngeal cancer (n = 1), laryngeal cancer (n = 1), colorectal cancer (n = 1), breast cancer (n = 1).
MR/PET and PET/CT Protocol
All patients fasted overnight before administration of the glucose analogue 18F-FDG. The radiotracer was injected in the PET/CT suite (mean dose ± standard deviation: 351 ± 22 MBq). Blood glucose was measured before injection to ensure blood glucose levels below 150 mg/dL. PET/CT was conducted at a Biograph mCT (Siemens Healthcare, Knoxville, TN, USA) as whole-body examinations in expiration. CT-based attenuation maps were calculated using the vendor-provided algorithm. PET was acquired under free breathing and reconstructed with iterative 3D ordered-subset expectation maximization (OSEM) algorithm using 2 iterations and 21 subsets and a Gaussian filter of 2 mm. The PET was acquired with 2–4 minutes/bed depending on the body region.
MR/PET was performed immediately after PET/CT on a Biograph mMR (Siemens Healthcare, Erlangen, Germany). Mean uptake time in MR/PET was 124 ± 13 minutes. PET was acquired under free breathing and reconstructed with an iterative 3D OSEM algorithm using 3 iterations and 21 subsets and a Gaussian filter of 3 mm. Time per bed was 4–6 minutes.
A whole-body 3D T1-weighted spoiled gradient-echo sequence fast low angle shot in end-expiratory breath-hold with Dixon-based fat-water separation (Dixon, sequence parameters in Table 1) was acquired for the generation of a segmentation-based PET AC map.
Lung Imaging
In PET/CT, the thorax was covered in expiration as part of the whole-body examination (CT acquired in expiration [CTex]). In addition, a lung CT scan in inspiration (CTin) was performed, which is a standard operation procedure of the routine scan protocol in our institution. CT was reconstructed in axial orientation with slice thickness of 3 mm (CTin) and 5 mm (CTex) with an in-plane resolution of 0.8 × 0.8 mm2. In MRI, axial VIBE sequences of the lung were acquired in inspiration and expiration (volume interpolated breath-hold examination acquired in inspiration [VIBEin], volume interpolated breath-hold examination acquired in expiration [VIBEex]). Lung images available from the whole-body Dixon sequence were also included in the evaluation. The 3D Dixon sequence was acquired in expiration for higher alignment quality with the PET data. Per default, the 3D Dixon sequence has to be acquired in coronal orientation. Detailed scan and reconstruction parameters for lung imaging were shown in Table 1.
Image Evaluation
Lung imaging was evaluated in consensus by 2 blinded radiologists experienced in thoracic (12 and 6 years) and hybrid imaging (6 and 4 years) including fellowships in nuclear medicine. Five separate reading sessions with different data sets were performed, each at least 8 weeks apart in a random order (CTex, VIBEin, VIBEex, and Dixon). Number, lobe and size of the lesions (longest diameter in lung window setting with window width, 1500 Hounsfield units [HU] and window level, -500 HU) were recorded for each patient. Confidence in the presence of a potentially malignant lesion was rated on a 4-point Likert scale (1, highly likely; 2, very likely; 3, probable; 4, uncertain) for each finding. Calcified nodules were not included in the analysis. PET was available in all reading sessions and PET images were visually analysed in combination with the morphological images to identify additional lesions only visible in PET.
The reference standard was defined in PET/CT with additional CT in inspiration by a third radiologist experienced in thoracic (11 years) and hybrid imaging (5 years) including fellowships in nuclear medicine. The third radiologist correlated the results (localization and confidence in presence of a lesion) of the 2 blinded readers in the different imaging modalities and performed a lesion-by-lesion comparison in all patients and recorded the detection of each lesion in VIBEin, VIBEex, CTex, and Dixon. Size (long axis diameter) of lesion was measured in CTin in lung window settings. If the lesion was not found by the readers in each modality, it was considered as "false negative". A lesion was defined as false positive if the lesion was not rated as lesion in the reference standard, e.g., small atelectasis or vessel mistaken for pulmonary nodule.
Data Analysis
In a lesion-based analysis, detection rate (sensitivity) of each image data set (CTex, VIBEin, VIBEex, and Dixon) was calculated. Size-depending evaluation was performed according to the size ranges defined by the Fleischner society (≤ 4 mm; > 4 to ≤ 6 mm; > 6 to ≤ 8 mm; > 8 mm) (20). In a lobe-based analysis, sensitivity and specificity were calculated for each image data set. The lobe-based analysis was performed because it is important for tumor node metastasis (TNM) staging in lung cancer and for preoperative treatment planning in patients eligible for metastasectomy. In addition to the overall evaluation, a separate analysis of diagnostic parameters was performed considering only malignant pulmonary lesions as proven by follow-up or biopsy. When biopsy was not available, the follow-up data was used to classify a lesion as malignant. For this purpose, standard diagnostic criteria were applied such as increase in size.
Statistical Analysis
Patients with > 10 lesions per lung were excluded to prevent disproportionate contribution of one patient to the evaluation. The Kruskal-Wallis one-way analysis of variance with post-hoc test was performed to assess for differences in the diagnostic confidence in lesion delineation between the different reading sets. As post-hoc test, a non-parametric multiple comparison test available in SPSS (correction for multiple testing included) was conducted. McNemar test was used to compare the detection rate between VIBEin and VIBEex. These statistical analyses and graphs were performed using SPSS software package (version 22.0.0, SPSS Inc., Chicago, IL, USA). Figures of merit (FOM) were calculated for each imaging set and compared using Jackknife FROC software (Jackknife alternative free-response receiver-operating characteristic, version 4.2.1; http://www.devchakraborty.com), which provides a specific analysis of observer free-response tasks (2122). P < 0.05 was considered statistically significant.
RESULTS
Three patients were excluded due to disseminated metastatic disease in both lungs (> 10 lesions per lung). In 23 of the evaluated 41 patients, 76 lung lesions were present as defined by the reference standard. On average, 3 ± 3 lesions (range: 1–18) per patient were found with a median lesion size of 6 mm (range: 2–86 mm). Size distribution of pulmonary lesions is given in Figure 2. Detection rates obtained in the lesion- and lobe-based analyses are given in Tables 2 and 3.
Lesion-Based Analysis
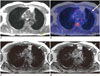
Compared to the reference standard, the lesion-based detection rate of all other modalities was inferior (CTex, 77.6%; VIBEin, 55.3%; VIBEex, 51.3%; and Dixon, 22.4%). In the size-dependent analysis, the detection rates of VIBE sequences ranged between 62.5 and 87.5% and dropped considerably for lesions ≤ 4 mm to 17.2% and 10.3% in VIBEin and VIBEex, respectively. In the Dixon sequence, lesions > 8 mm in size were missed in 38% of cases. In the lesion-based analysis, 5 false positive lesions were found in VIBEin, which could be ascribed to fibrotic and dystelectatic changes. In the Dixon sequence, 1 round atelectasis was falsely rated as lesion (Fig. 3). Adding the PET information to the different MR readings, an additional lung lesion was identified for the Dixon reading set, which was confirmed malignant in follow-up (Fig. 4); while using VIBEin or VIBEex sequences, no additional pulmonary lesion was found in PET.
Lobe-Based Analysis
In the lobe-based analysis, lesions were found in 48/204 lobes (in 1 patient, only 2 lobes were present on the right side after lobectomy). The lobe-based sensitivity of CTex and MRI sequences was generally higher compared to the lesion-based analysis and all T1-weighted MRI sequences still provided inferior detection rates than CT (CTex, 89.6%; VIBEin, 58.3%; VIBEex, 60.4%; and Dixon, 27.1%). In all reading sets (either CT or MRI), lung nodule evaluation showed high specificity (98.7–100%). Two lesions in the VIBEin sequence and 1 lesion in the VIBEex sequence were assigned to another lobe leading to 2 false positive cases in VIBEin and 1 false positive case in VIBEex in the lobe-based analysis. The erroneous lobe attribution occurred due to the limited identifiability of fissures in MRI (Fig. 5).
Diagnostic Confidence Analysis
The diagnostic confidence in lesion delineation was rated highest in VIBEin (1.2 ± 0.6) and CTex (1.2 ± 0.7) followed by VIBEex (1.5 ± 0.9) and Dixon (1.7 ± 1.1). In the post-hoc analysis, no statistical significant difference was found.
Figures of Merit
The diagnostic performance of the different imaging techniques as represented by FOMs is summarized in Table 4. CTex had a significantly higher FOM compared to VIBEin, VIBEex, and Dixon. The Dixon sequence had a significantly lower FOM compared to VIBEin, VIBEex, and CTex. FOM of VIBE in inspiration and expiration did not significantly differ.
Separate Analysis of Malignant Pulmonary Lesions
In 17 of 23 patients with pulmonary lesions, follow-up or biopsy was available. In these 17 patients, 47 lesions were identified. Based on biopsy and follow-up, 33 of these 47 lesions were malignant (median lesion size: 8 mm, range: 2–86 mm). Taking into account only these proven malignant lesions, the lesion-based detection rate increased in all modalities irrespective of inspiration or expiration breath-hold imaging (CTex, 84.8%; VIBEin, 75.8%; VIBEex, 69.7%; and Dixon, 33.3%). Patient-based, it was possible to identify all patients with malignant lesions in CTex, VIBEin and VIBEex, although several single lesions were missed. In contrast, 3 patients were rated false-negative for malignant lesions based on the Dixon sequence alone (Fig. 6). Of these, one could be identified as having a lung nodule when adding the PET information (Fig. 4).
Influence of Image Acquisition in Inspiratory and Expiratory Breath-Hold
In contrast to CT, the percentage difference of lesion detection rates between inspiratory and expiratory breath-hold was small and not significant (3.9% between VIBEin and VIBEex versus 22.4% between CTin and CTex). Taking into account only the malignant lesions, the percentage difference of detection rates between VIBEin and VIBEex was slightly higher with 6.1%, without reaching significance (percentage difference between CTin and CTex: 15.2%).
DISCUSSION
In the present study, the diagnostic performance of standard fast T1-weighted images was investigated for lung nodule assessment in MR/PET imaging of cancer patients. Three different fast T1-weighted sequences commonly used in MR/PET were evaluated to assure large clinical representativeness. The secondary focus was on the influence of the breath-hold in inspiration versus expiration, since scans in expiration are known to show higher alignment quality with PET (1623). In order to consider the diagnostic value for patient management, different evaluation perspectives were considered by performing lesion-, lobe- and patient-based analyses. Moreover, separate evaluation was performed for the different size categories of pulmonary lesions established by the Fleischner society (20).
To our knowledge, no systematic comparison of breath-hold positions used in dedicated VIBE sequences for lung imaging in MR/PET has been performed yet. PET/CT studies have shown that CT in expiration or shallow breathing is inferior in pulmonary lesion detection although it offers higher alignment quality to PET data (2425). This is in accordance with our study results. Interestingly, in contrast to CT, there was no substantial difference between breath-hold positions in the VIBE sequences. Thus, a dedicated lung VIBE sequence in expiration might be sufficient for the assessment of pulmonary lesions in oncologic MR/PET protocols.
In the lesion-based analysis, CT (either in inspiration or expiration) was superior compared to MRI. However, the detection rate in MRI markedly increased when only malignant lesions were taken into account (VIBEin: 76% vs. 55%). In the patient-based evaluation, no patient with pulmonary lesions was missed using the dedicated VIBE sequence irrespective of the breath-hold position. Recently, Raad et al. (11) showed that most pulmonary lesions (97%) missed on MR/PET were stable or vanished in follow-up imaging indicating their benign nature. This observation is also reflected by our data.
In our study, the overall detection rate of VIBEin was 55%, which is below detection rates reported in the literature: Chandarana et al. (26) found a detection rate of 62% using a radial VIBE sequence in an integrated MR/PET. Rauscher et al. (27) report a detection rate of 68% using a VIBE sequence in inspiration with the same scanner type. However, to assure comparability among different studies, the size distribution of the lesions needs to be considered, especially the frequency of small lesions (28). Chandarana et al. (26) included 25 lesions < 5 mm (36% of all lesions evaluated); while Rauscher et al. (27) used ranges below and above 1 cm for evaluation. Moreover, there may be differences between the acquired and reconstructed voxel size reported in the literature, which is important when evaluating small pulmonary nodules. Besides, the size measurement of lung nodules can be significantly affected by respiration-related changes in lung volume (29).
Early in the evolution of MR/PET, the Dixon sequence for AC was hypothesized to contribute to a morphological identification of FDG-avid lesions (1530). However, Rauscher et al. (27) reported low detection rates for the Dixon sequence (32%). In the present study, the lesion-based detection rate for lung nodules was even lower (22%) and 3 patients with malignant pulmonary lesions were missed in the Dixon sequence. In 1 of these 3 patients, the PET information allowed for correct identification of the malignant lesion. The Dixon sequence required for AC is recorded with a relatively low matrix size (determined by the vendor) and cannot be recommended as a sufficient diagnostic option in staging of cancer patients. In contrast, all patients with malignant lesions were identified using dedicated VIBE sequences, irrespective of the breath-hold position.
The reference standard is a critical issue when interpreting comparison studies for pulmonary lesion detection. Stolzmann et al. (31) analysed 66 lesions in 40 patients and found almost comparable detection rates in MRI and CT with the low-dose CT of PET/CT acquired under shallow breathing as reference. In our study, a high-resolution CT in inspiration was the reference standard, which might explain the inferiority of MRI compared to CT.
Another influencing factor for lung nodule evaluation can be the sequence weighting used for lung imaging. Schaarschmidt et al. (32) compared different sequences for T staging in 28 non-small-cell lung cancer patients and found high accuracy for T2-BLADE (proprietary name for periodically rotated overlapping parallel lines with enhanced reconstruction) and T2-half-Fourier acquisition single-shot turbo spin-echo (HASTE) sequences possibly attributable to superior tumor delineation; however, they did not perform a size-based analysis, which limits direct comparison. Although T2-weighted sequences are reportedly beneficial for pulmonary lesion characterization (33), their relatively long acquisition time and the concomitant need for respiratory and/or cardiac gating may interfere with patient compliance and smooth workflow in routine MR/PET schedules. Therefore, dedicated 3D VIBE sequences have been preferred for lung evaluation in oncologic MR/PET, since they can be performed within one breath-hold and have been reported to provide excellent results in lung staging compared with PET/CT (34).
Interestingly, in 2 cases, false diagnosis of lobe involvement was made in MRI because lung fissures essential for correct lobe attribution were not clearly visible. This is important in lung staging when lobe involvement can make a difference in T staging (separate tumor nodule in the same lobe versus separate tumour nodule in different ipsilateral lobe). However, in our study, the false lobe attribution that occurred in 2 metastatic thyroid cancer patients did not alter the overall staging and treatment strategy.
In our study, follow-up examination or biopsy was available for 47 lesions in 17 patients. 33 of those 47 lesions were malignant. Considering only these malignant lesions, the detection rates increased for all modalities. It is important to note, that the median lesion size of these malignant lesions was smaller compared to all lesions (median lesion size: 6 mm vs. 8 mm). This is in accordance with the literature where many small pulmonary nodules are reported to be benign even in oncologic patients (35).
Our study has limitations. First, no intravenous contrast media was used for MR imaging. Lee et al. (36) reported that the application of contrast media did not provide additional value in the detection rate of pulmonary nodules. However, the use of dynamic contrast-enhanced imaging might be helpful in the differentiation between benign and malignant nodules. Acquisition of dynamic series, however, accompanies an increase in acquisition time. Second, in this study set-up, we merely included fast T1-weighted sequences and did not evaluate T2-weighted sequences or gradient-echo sequences with radial stack-of-stars trajectory because the latter have acquisition times of several minutes. Our study was focused on fast sequences that can smoothly be integrated in an oncologic whole-body MR/PET protocol. Third, the reconstruction parameters of CTin and CTex differed because CTex was part of the whole-body acquisition while CTin was a dedicated lung scan. These CT reconstructions are part of the routine clinical PET/CT protocol, which was not explicitly changed for this retrospective comparison study. However, the analysis of the CT in expiration was not the primary scope of the study designed to investigate the diagnostic performance of fast dedicated MR sequences used for pulmonary lesion evaluation in oncologic MR/PET patients. Fourth, there is a selection bias due to the retrospective evaluation of the imaging data and the patient number was rather small limiting the representativeness for a general oncology patient collective. Finally, histological correlation was not available for each single lesion. This is not realizable in patients with numerous small lung nodules for obvious reasons. However, we included a separate analysis of diagnostic performance considering only malignant pulmonary lesions, which were confirmed by follow-up or biopsy.
In conclusion, the value of fast T1-weighted sequences used for lung nodule assessment in MR/PET imaging of cancer patients depends on the evaluation strategy: in a lesion-based comparison, MRI clearly remains inferior to CT irrespective of the breath-hold position with very low detection rates for small (< 4 mm) lung nodules. However, the diagnostic performance of fast VIBE sequences improves when moving to lobe- or patient-based analyses, which may represent a more treatment-orientated evaluation strategy. Fast T1-weighted VIBE sequences as routinely available in MR/PET protocols allow for reliable identification of patients with malignant pulmonary lesions. The Dixon sequence routinely included for AC cannot be considered adequate for lung nodule evaluation in cancer patients irrespective of the evaluation strategy (lesion-/lobe-/size-based) due to the poor detection rate and the low confidence in lesion delineation. In contrast to CT, the breath-hold position does not substantially alter the detection rate for lung nodules in fast T1-weighted VIBE sequences in MR/PET but plays an important role for the diagnostic confidence in lesion delineation.









 XML Download
XML Download