

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Asbestos, once considered as a miracle mineral, being resistant to fire, heat, and corrosion, is strong, durable, flexible and inexpensive, and has been used to make a vast array of friction materials, gaskets, roofing, and fireproofing materials (12). There was a sharp increase in the use of asbestos in the 1970s as the Korean economy developed rapidly. However, asbestos is associated with many health problems, affecting principally the pleura and lung parenchyma, and is banned from Korea since 2009. Nonetheless, previous exposure to asbestos still causes many problems because asbestos-caused disease has a long latency period (2).
The most significant change that occurs in the lung parenchyma after asbestos exposure is lung fibrosis caused by asbestos dust, which is termed asbestosis (3). A definite dose-effect is evident between the asbestos exposure level and the severity of fibrosis (45). Disease usually develops approximately 20 years after initial exposure (5). Asbestosis is a principal disease of lung parenchyma exposed to asbestos, being second only to bronchogenic carcinoma in terms of frequency (67).
Asbestos-related diseases is expected to increase in frequency for many years to come (89). Based on a historical review of asbestos use and exposure in Korea, the disease is expected to peak in 2045 (10). In 2011, the Asbestos Damage Relief Law was established in Korea, and individuals who apply to the Korea Environment Corporation for asbestos damage relief are required to undergo chest computed tomography (CT) to evaluate the lung parenchyma and pleura. If compensation is to be made, CT must show changes consistent with asbestosis. In addition, it is necessary to document a history of asbestos exposure in combination with the chest CT findings, and/or to show impairment of pulmonary function. This is because pathological confirmation of disease is difficult even when asbestosis is suspected.
Therefore, radiologic evaluation of individuals exposed to asbestos plays a critical role in the assessment of asbestosis. It is important to be familiar with the radiologic characteristics of the disease because it will persist for some time. This article illustrates the imaging characteristics of early to advanced asbestosis, with particular emphasis on chest CT findings.
Pathogenesis of Asbestosis
Asbestos fibers are carried deep into the lungs, and activated macrophages attempt to ingest and remove them. However, many are retained in the lung parenchyma (1112). The fibers induce apoptosis of macrophages and trigger inflammation. The latter effect is reduced if fibers become coated to create asbestos bodies, but most fibers in the lung parenchyma remain uncoated. Thus, asbestos fibers remain in the lung parenchyma for prolonged periods and penetrate the interstitium of the distal lung (11). The fibers induce inflammatory processes including alveolitis and inflammation of the surrounding interstitium, followed by fibrotic changes in the respiratory bronchioles that extend to adjacent alveolar tissue (1314).
The College of American Pathologists' grading system of histologic criteria of asbestosis to describe severity and extent includes Grade I involving alveolar walls of respiratory bronchioles and the alveolar ducts; Grade II involving greater proportions of acini; Grade III involving the whole acinar structure; and Grade IV when honeycomb remodeling and large (up to 1 cm) dilated spaces are grossly visible in the lung parenchyma (1516).
Diagnostic Criteria and Guidelines for Asbestosis
The diagnosis of asbestosis is based on the 2004 American Thoracic Society criteria and the 2014 Helsinki criteria. The former is slightly modified from the initial 1986 diagnostic criteria. Structural pathology consistent with asbestos-related disease is required. This can be shown by imaging or histology. Imaging includes chest radiography, high-resolution CT (HRCT), and possibly future imaging methods. Chest radiographs are evaluated using the International Labor Organization (ILO) classification, and must show irregular opacities and profusion score of more than 1/1. Such findings, together with a history of asbestos exposure, are adequate for a diagnosis of asbestosis. In subjects with low profusion scores on chest radiographs, CT can be helpful to diagnose asbestosis. In addition, evidence of disease causation by asbestos is required. This can be achieved by documenting occupational and environmental history, identifying a plausible latency period, demonstrating markers of asbestos exposure (usually pleural plaques), and/or recovering asbestos bodies from lung tissue. Evidence of functional impairments such as signs and symptoms and/or changes in pulmonary function test, are not required for a diagnosis, but are part of complete evaluation (17).
The 2014 Helsinki criteria require the patient to have a work history compatible with significant asbestos exposure. This may be documented via a structured interview and/or by identifying asbestos fibers in lung tissue and bronchoalveolar lavage fluid (18). For histologic diagnosis of asbestosis, the updated 2010 diagnostic criteria for asbestosis by a Committee of the College of American Pathologists and the Pulmonary Pathology Society are recommended (1819). For radiologic diagnosis, chest radiographs revealing small opacities (ILO grade 1/0) are considered to indicate early-stage asbestosis. The use of CT imaging in diagnosis of asbestos-related diseases may be useful under the following conditions: 1) a borderline finding of lung fibrosis (ILO grade 0/1–1/0); 2) discrepancy between lung function findings of restriction and radiographs interpreted as normal; and 3) widespread pleural changes that severely hamper the radiographic visibility of lung parenchyma (18). The Helsinki criteria recommend the use of the International Classification of HRCT for Occupational and Environmental Respiratory Diseases to evaluate HRCT findings associated with asbestosis (1820).
Asbestos-Related Malignancy
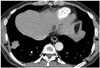
Asbestos related malignancies are lung cancer and malignant mesothelioma. Asbestos related lung cancer accounts for about 3–8% of all the lung cancers and the histologic type of cancer and its signs and symptoms in asbestos-exposed and unexposed individuals are similar (Fig. 1) (21). The exact mechanism of carcinogenesis is as yet unclear (3). However, risk of developing lung cancer is related to cumulative asbestos exposure. According to the Helsinki criteria, a cumulative exposure of 25 fibre-years is estimated to increase the risk of lung cancer 2-fold, and the clinical cases of asbestosis may occur at comparable cumulative exposures (18). In addition, asbestosis can be a marker for increased risk of lung cancer (22).
Malignant mesothelioma is the most common primary neoplasm of the pleura, arising from mesothelial cells. Although the necessary degree of asbestos exposure is considerably less than that of asbestosis and lung cancer, a dose dependent relationship is recognized (323). The attributable risk of asbestos for malignant mesothelioma is generally considered as 80 to 90%, but is around 60% in Korea. Pathologically confirmed malignant mesothelioma is internationally accepted as related to asbestos regardless of the patient's history of asbestos exposure (24). Several previous studies (25262728) report a higher mortality rate of malignant mesothelioma in workers with asbestosis, which suggests that asbestosis might have positive association between malignant mesothelioma (29).
Chest Radiographic Findings of Asbestosis
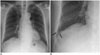
The initial radiographic characteristics of asbestosis are small, irregular or reticular opacities, predominantly in the bases of the lungs (Fig. 2), indicative of peribronchiolar and adjacent alveolar interstitial fibrosis (30). The opacities may progressively spread through the middle and upper lung zones (17). In more advanced cases, honeycombing is evident on chest radiographs (Fig. 3) (5). In addition, pleural thickening or pleural plaques may also be seen. However, there is no known radiographic finding that is pathognomonic of asbestosis. When asbestosis is evaluated via chest radiograph alone using the ILO classification, the diagnostic specificity is low in asbestos exposed individuals (7). Kipen et al. (31) show that 18% of patients with biopsy proven asbestosis have no radiographic abnormalities and 80% yield chest radiographic findings that do not correlate with their histopathologic grades. For these reasons, chest radiographs are of limited use for diagnosing asbestosis. A normal chest radiograph does not exclude the possibility of asbestosis in an asbestos-exposed individual.
Nonetheless, chest radiograph is important in the diagnosis of asbestosis, because it can document the presence or absence of pleural plaques as a marker of asbestos exposure, and allows the evaluation of the presence and extent of other complications such as lung cancer, pleural abnormalities, malignant mesothelioma, and round atelectasis (5).
Digital tomosynthesis is an alternative method with a low radiation dose compared to chest CT as well as better detection rate compared with chest radiograph (32333435). Digital tomosynthesis findings of asbestosis are presence of reticular opacities and/or honeycomb cysts in the bases of the lung, which are same as chest radiographs (3637). Lee et al. (37) report that digital tomosynthesis is more sensitive than chest radiographs in the detection of asbestosis and also with detection of pleural plaques.
CT Findings of Asbestosis
Chest CT is much more sensitive than chest radiograph in evaluating asbestosis. Staples et al. (38) report that 57 of 169 asbestos exposed workers with normal chest radiographs show findings of asbestosis on CT. The chest radiographic findings are discrepant from the CT findings; only subtle changes of reticular densities are seen in chest radiographs; whereas, CT may reveal more advanced features of fibrosis such as honeycomb cysts (Fig. 4). Friedman et al. (39) show that 14 of 60 chest radiographs considered to reflect asbestosis are actually false-positives; and CT shows that the chest radiographic abnormalities are caused by emphysema, en-face plaques, or scarring from old tuberculosis.
Since early findings of asbestosis on CT are very subtle, it may be unsuitable to scan the patient with low dose or ultra-low dose CT scan, which increases image noise that may diminish image quality and depiction of radiologic findings of asbestosis. Tekath et al. (40) compare ultralow dose CT with standard CT for detecting asbestos related diseases. Ultra-low dose CT compares favorably with standard CT in detecting pleural plaques and diffuse pleural thickening, however interstitial pulmonary abnormalities are less frequent in ultra-low dose CT than standard CT.
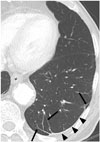
Subpleural Dot-Like or Branching Opacities
The earliest CT findings in asbestosis are subpleural dot-like or branching opacities located a few millimeters from the pleura but seldom touching the pleura, or they may appear as a fine branching structure (Fig. 5) (4142). Some nodules are obvious whereas others present as very faint nodules of ground-glass opacity (GGO). Pathologically, subpleural dots correlate with the appearance of peribronchiolar fibrosis (4142).
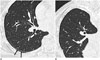
Subpleural Curvilinear Lines
As the subpleural dot-like or branching opacities increase in number, confluence of dots creates subpleural curvilinear lines. Such lines are defined as linear areas of increased density located within 1 cm of the pleura and lying parallel to the inner chest wall on CT (Fig. 6). The development of subpleural curvilinear lines correlates with peribronchiolar fibrotic thickening combined with alveolar flattening and collapse attributable to fibrosis (4142). Subpleural curvilinear lines can also indicate the presence of atelectasis, which has a propensity to occur adjacent to plaques (43).
Parenchymal Bands
Parenchymal bands are also commonly seen in asbestosis. On CT, the bands are linear, 2–5 cm in length, and contact the pleural surface (Fig. 7) (44). The bands reflect the development of fibrosis along the bronchovascular sheathes or interlobular septa, with distortion of the lung parenchyma (42). In asbestosis, these bands are often associated with areas of pleural plaques and frequently occur at the lung bases (Fig. 8) (445). According to Akira et al. (46), parenchymal bands occur significantly more often in patients with pleural thickening than in others.
Findings of Advanced Asbestosis
As the pulmonary fibrosis extends from the peribronchiolar lesions to involve the residual pulmonary lobules, other characteristic CT findings of pulmonary fibrosis develop. These include intralobular interstitial thickening, interlobular septal thickening (Fig. 9), traction bronchiectasis or bronchiolectasis, and honeycomb cysts (Fig. 10) (424546). Intralobular interstitial thickening correlates with peribronchiolar fibrosis with subsequent involvement of the alveolar ducts and interlobular septal thickening correlates with interlobular fibrotic or edematous thickening. As findings of advanced asbestosis are similar to pulmonary fibrosis by other causes, they are difficult to distinguish.
These above mentioned CT abnormalities associated with asbestosis usually develop in the lower lung, posterior, and basal subpleural areas. As disease progresses, abnormalities also develop in the middle and upper lung zones. The CT abnormalities are usually bilateral and often somewhat symmetrical (414648). As the posterior lung regions are typically involved early in asbestosis (49), it is important to scan asbestos-exposed individuals in the prone position to differentiate normal dependent atelectasis from early asbestosis in the posterior lung (Fig. 11) (4445).
CT Findings of Asbestosis in Korea
Our previous study (50) indicates that the common CT findings of asbestosis in patients environmentally exposed to asbestos in Korea are centrilobular opacities, subpleural dot-like or branching opacities, interlobular septal thickening, intralobular interstitial thickening, parenchymal bands and subpleural curvilinear lines. Asbestos related lung parenchymal CT findings in the participants with environmental exposure are similar to those from occupational exposure. However, Kim et al. (51) show that occupationally exposed participants have larger extents of pleural plaques and pulmonary fibrosis than environmentally exposed participants. Subsequently, we retrospectively reviewed the chest CTs of 200 asbestosis patients compensated under the Asbestos Damage Relief Law from January 2011 to May 2013. We also reviewed 11 cases of idiopathic pulmonary fibrosis (IPF) to compare the imaging characteristics of asbestosis and IPF (Table 1).
In our study, subpleural dot-like or branching opacities are the most common feature of asbestosis (97.5%) but are absent in IPF (p < 0.001). The subpleural curvilinear lines are characteristic findings of asbestosis, but have relatively low frequency (17.0%) in the present study. However, such lines are absent in IPF, so the lines are very useful for the diagnosis of asbestosis. Parenchymal bands are often evident in asbestosis (50.5%) but not found in IPF (p = 0.012). Therefore, parenchymal bands are a characteristic feature of asbestosis. Parenchymal changes adjacent to pleural plaques are frequently seen in asbestosis (39.5%) (p < 0.05). Both parenchymal bands (54.4%) and round atelectasis (8.9%) are common findings. So parenchymal changes adjacent to pleural plaques are helpful in differentiating between asbestosis and IPF. Pleural plaques are observed in most cases of asbestosis (98.5%) but not IPF (p < 0.001). Therefore, pulmonary fibrosis associated with pleural plaques is helpful in the diagnosis of asbestosis. Thus, pleural plaques require careful consideration, particularly thin and small plaques.
In our study, intralobular interstitial thickening and interlobular septal thickening are common in both asbestosis and IPF. They are general findings of pulmonary fibrosis, and do not aid in differential diagnosis. Traction bronchiectasis is found in both asbestosis (43.5%) and IPF (100%) (p = 0.004). But traction bronchiectasis is more common in IPF than asbestosis, traction bronchiectasis is more indicative of IPF than asbestosis. Honeycomb cysts are much more frequently seen in IPF (81.8%) than asbestosis (17.5%) (p = 0.009). However, it is difficult to differentiate asbestosis featuring honeycomb cysts from IPF solely by findings of honeycomb cysts, and it is necessary to evaluate finding of subpleural dot-like or branching opacities in the less severely diseased lung, the history of asbestos exposure, and the presence of pleural plaques. GGO is also more frequent in IPF (100%) than asbestosis (15.5%) (p < 0.001). Although GGO is a helpful finding, it is considered a nonspecific feature of pulmonary fibrosis.
In summary, CT findings of subpleural dot-like or branching opacities, parenchymal bands, parenchymal changes adjacent to pleural plaques, and plaques are more frequently noted in asbestosis. Honeycomb cysts, GGOs, and traction bronchiectasis are more frequently noted in IPF. Although we have made an effort to differentiate asbestosis from IPF, some cases are very difficult to diagnose using CT findings alone. Appropriate history of asbestos exposure combined with CT abnormalities of the lung parenchyma and pleura must be used to ensure a reliable asbestosis diagnosis.
Differential Diagnosis between Asbestosis and IPF
A study by Akira et al. (46), emphasizes the specific combinations of CT findings strongly suggesting either asbestosis or IPF solely based on lung parenchymal findings other than associated pleural abnormalities. They show that subpleural dot-like or branching opacities, subpleural curvilinear lines, mosaic perfusions, and parenchymal bands are more common in patients with asbestosis. Honeycomb cysts, visible intralobular bronchioles and traction bronchiectasis are more common in patients with IPF; whereas, GGO, interlobular septal thickening, and emphysema are similar in both groups. They further indicate that the most important difference between asbestosis and IPF is subpleural dot-like or branching opacities in the subpleural region. Subpleural dot-like or branching opacities are found in mild as well as advanced cases of asbestosis. In advanced asbestosis, these opacities are found in less severely diseased regions of the lung (46). Copley et al. (52) compare the CT features of asbestosis with those of patients with biopsy proven nonspecific interstitial pneumonia (NSIP) and biopsy proven IPF. CT reveals coarser fibrosis in the asbestosis patients, as compared to NSIP cases; however, the fibrosis of the asbestosis is similar to that of the IPF. In study by Arakawa et al. (53) of 33 asbestos-exposed patients with pathologically confirmed pulmonary fibrosis, 15 patients are asbestosis and 18 patients include various kinds of fibrosis; subpleural curvilinear lines are the sole CT finding that differ between asbestosis and non-asbestosis cases.
CONCLUSION
The characteristic chest radiographic findings of early asbestosis are small irregular or reticular opacities, located predominantly in the lung bases and show honeycombing in advanced stages. The characteristic CT findings of asbestosis are subpleural dot-like or branching opacities, parenchymal bands, parenchymal changes adjacent to pleural plaques, subpleural curvilinear lines and plaques. In more advanced cases, honeycomb cysts, traction bronchiectasis, intralobular interstitial thickening and interlobular septal thickening are also seen. CT plays a key role in the diagnosis of asbestosis in Korea. Thus, knowledge of the characteristic CT findings of asbestosis can guide the diagnosis and management of patients. In addition, accurate diagnosis would encourage responsible asbestos-related damage judgments and lead to appropriate compensation.








 XML Download
XML Download