

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Proton magnetic resonance spectroscopy (1H-MRS) has traditionally been used in the metabolic research of gliomas and its diagnostic value is well explored (123456789). Currently, however, 1H-MRS is used only as a supplemental tool to magnetic resonance imaging (MRI) in the diagnosis of gliomas (259). Such limited application of 1H-MRS in the diagnosis of gliomas can be attributed to the intrinsic low concentrations of metabolites and the limited spectral signal-to-noise ratio (SNR) and dispersion at clinical field strength. In addition, lack of specificity of metabolites that are previously proposed as biomarkers of gliomas is also responsible for its low demand by neuroradiologists. In this regard, the emergence of 2-hydroxyglutarate (2HG) as an onco-metabolite overproduced in isocitrate dehydrogenase (IDH)-mutated (IDH-MT) gliomas (10111213), the substantially longer survival duration of IDH-MT glioma patients relative to those with IDH wild-type (IDH-WT) gliomas (11), and recent pioneering studies on the feasibility of non-invasive detection of 2HG by 1H-MRS (141516), collectively, have recently drawn attention of neuroradiologists. However, due to severe spectral overlap with its background signal, the quantification of 2HG is reportedly challenging (1516). As such, despite a total of only 9 studies reported to date (141516171819202122) on in-vivo 1H-MRS of 2HG in gliomas including 2 animal studies (2022), 5 different 1H-MRS methods were already explored.
In this review, we first summarize the biochemistry of 2HG and its significance in the diagnosis of IDH-MT gliomas. Secondly, we comparatively review 1H-MRS methods and findings in the previous studies. Finally, we discuss the current status of 1H-MRS in the diagnosis of IDH-MT gliomas as a technical guideline for neuroradiologists.
Altered Metabolism and Overproduction of 2HG in IDH-MT Gliomas and Their Significance in Noninvasive Detection of 2HG by 1H-MRS
Isocitrate dehydrogenase is an enzyme with three isoforms, i.e., IDH1, IDH2, and IDH3 (13). Intra-cellularly, it catalyzes the oxidative decarboxylation of isocitrate to α-ketoglutarate (α-KG) in cytoplasm and peroxisomes (IDH1) and in mitochondria (IDH2 and IDH3) (Fig. 1) (1323). Highly frequent mutations in IDH1 and IDH2 genes are reported in low grade gliomas and secondary glioblastomas (1011). These mutations result in altered enzymatic activities of IDH1 and IDH2 such that they catalyze the reduction of α-KG to 2HG (12) instead of facilitating the production of the former (Fig. 1). As it is an aberrant product arising from altered metabolism in IDH-MT gliomas, 2HG is designated as an onco-metabolite (1324).
In IDH-MT gliomas, 2HG accumulates to a similar or higher level than 1H-MRS-visible brain metabolites, and 2–3 orders of magnitude higher than in IDH-WT gliomas or normal brain tissue (13). Thus, 1H-MRS has the potential to quantify 2HG non-invasively and discriminate IDH-MT gliomas from IDH-WT gliomas as well as normal tissue. Thus, 1H-MRS can directly determine the mutational status of gliomas non-invasively. The substantial difference in the frequency of IDH-mutational status between primary and secondary glioblastomas (11) further contributes to the potential diagnostic efficacy of 1H-MRS of 2HG (24). In cases where 2HG content correlates with tumor cellularity, 1H-MRS of 2HG can be used for guiding biopsy and surgery (1518), and monitoring treatment response (16). In addition, the longer survival duration of patients with IDH-MT gliomas than IDH-WT gliomas (11) also suggests a potential prognostic value of 1H-MRS of 2HG. These characteristics distinguish 2HG from previously proposed brain metabolites as 1H-MRS-etectable biomarkers of gliomas (126).
Recent findings also emphasize the potential importance of other brain metabolites in IDH-MT gliomas. For instance, the carbon source of 2HG is derived from glutamine (Gln) (12), and the reduction of glutamate (Glu) levels may be associated with the pathogenesis of the IDH1-MT gliomas (2526). Also, the down-regulation of glutathione (GSH) in IDH1-MT gliomas is proposed as a potential therapeutic target (27). Therefore, developing 1H-MRS methods that allow for more comprehensive metabolic profiling can play a pivotal role for better understanding the pathogenesis and progression of the diseases such as whether the oncogenesis is directly associated with 2HG or a consequence of the subsequent metabolic alterations. It may also shed light on the underlying mechanism of longer survival of patients with IDH-MT glioma vs. IDH-WT gliomas (20252627), and the development of novel therapeutic strategies (262728).
Spectral Characteristics of 2HG and Its Background Metabolites
The 2HG molecule has 5 non-exchangeable protons (5-spin system) with complicated J-coupling interactions (16). These interactions refer to inter-spin interactions through electron bonds in a molecule (2930). Such an indirect interaction between spins rather than a direct interaction through space is termed as J-coupling and the spins involved in the interaction are said to be J-coupled (2930). J-coupling results in peak splitting (e.g., a singlet into a multiplet) and changes in line shape and signal amplitude as a function of time (typically, echo time [TE]), namely J-evolution (2930). Different spin systems undergo different J-evolution depending on their coupling networks and coupling strength expressed as a J-constant in Hz (2930). The majority of the 1H-MRS-detectable metabolites have coupled spins such as 2HG, Glu, Gln, gamma-aminobutylic acid (GABA), and N-acetylaspartylglutamate (NAAG) (31). On the other hand, water and creatine (Cr) are representative metabolites with uncoupled spins only. The spectral characteristics of 2HG are determined by J-coupling in combination with the resonance frequencies of the 5 protons that are determined by chemical environments of the protons in the molecule (chemical-shift), giving rise to three multiplets at 3T centered at ~4.0, ~2.3, and ~1.9 ppm (contributed by 1, 2, and 2 spins, respectively) (Fig. 2) (16). The spins resonating at ~1.9 ppm are J-coupled with the spin resonating at ~4.0 ppm and also with those resonating at ~2.3 ppm (16). The multiplet at ~4.0 ppm is relatively small in amplitude as it is contributed by only one proton, overlaps with signals from lactate (Lac) and myo-inositol (mI) (Fig. 3), and is close to the strong Cr (~3.9 ppm) and water (~4.7 ppm) signals. The multiplet at ~1.9 ppm also overlaps with signals from other metabolites (Fig. 2), in particular, with N-acetylaspartate (NAA) (Fig. 3). The multiplet at ~2.3 ppm has the largest signal and is therefore widely used as a target signal for 2HG quantification (Fig. 2). However, it also severely overlaps with signals from at least 4 other metabolites (Figs. 2, 3) (1516).
Short TE, Long TE, Difference Editing and 2D Methods, and Data Post-Processing
Short TE
In a short TE method, spectra are acquired at a shortest TE attainable in order to minimize signal loss resulting from relaxation and, for coupled spins, J-evolution. For a PRESS sequence (32) that is one of the most widely used single-voxel 1H-MRS pulse sequences together with a STEAM sequence (33) at clinical field strength, a shortest TE can slightly differ for different MR scanners depending on the design of radio-frequency (RF) and gradient pulses, but is ~30 ms at 3T. At a shortest TE, all metabolite signals are maximized, which is of great advantage in terms of SNR of spectra and thus scan time. A short TE method does not require any modification of vendor-provided pulse sequences, hence is most commonly used in 1H-MRS in combination with spectral fitting for quantification of individual metabolites.
However, a shortest TE maximizes not only the target signal of 2HG at ~2.3 ppm but also those background signals from Glu, Gln, GABA, and NAAG (Fig. 2). The resulting severe spectral overlap is exacerbated by the presence of spectral baseline that is also maximized at the shortest TE (Fig. 3). Spectral baseline is contributed mainly by macromolecules (MMs) such as proteins and peptides (34), and also by lipid (3536). MMs also have J-coupled spins and their T1 and T2 are short relative to metabolites (34). The influence of spectral baseline on the quantitative analysis of spectra acquired at a shortest TE is well documented (3738). In particular, quantification of Glu and Gln is most influenced by spectral baseline among the 1H-MRS-visible metabolites (37). As the target signal of 2HG at ~2.3 ppm directly overlaps with Glu and Gln, the quantification of 2HG by using a short TE method can be very challenging, sometimes resulting in false 2HG-positive or 2HG-negative cases, as previously demonstrated (141517). For this reason, different 1H-MRS methods were explored in the previous 1H-MRS 2HG studies such as a long TE method (16171921), a difference editing (1516), and a 2-dimensional (2D) method (15).
To minimize its influence on the quantitative outcome, spectral baseline can be modeled based on metabolite-nulled spectra as a surrogate of true spectral baseline, which are acquired with T1-weighting by taking advantage of the substantially short T1 of MMs relative to those of metabolites (3537). The modeled spectral baseline is then incorporated into the spectral fitting. A better but more time-consuming approach is to acquire such a metabolite-nulled spectrum in a subject-specific manner (3940).
Long TE
A long TE method, which is a simplest practice of 'spectral editing', takes advantage of different J-evolution of different coupled spin systems (3041). It also takes advantage of different T2 between metabolites and spectral baseline (41). Using J-evolution and T2 as 'spectral contrast', spectra can be 'edited' for discriminating a target signal from background signals, and the integrity of the edited target signal is determined by how precisely the long TE is tuned.
In fact, a long TE method has long been used for 1H-MRS of gliomas, for instance, for the quantification of Cr and choline (Cho) (Fig. 3) (7). A long TE does not need to be fine-tuned for such singlets from uncoupled spins. It is simply optimized by making it as long as possible such that spectral baseline and background metabolite signals from coupled spins are effectively suppressed, while retaining an observable amount of signal from the target singlet(s) (Fig. 3). However, for spectral editing of a target metabolite with coupled spins against background metabolites also with coupled spins, thorough analyses of the evolution of all spin systems involved are required for optimization of TE (4142). For a simple coupled spin system, this can be achieved by analytically calculating the spin evolution using product operators (43) assuming that all RF pulses are applied instantaneously (2943). For instance, for the Lac spin system, the J-evolution of the doublet at ~1.3 ppm can be approximated simply with a cos (π·J·TE) term, where J is the J-constant between the coupled spins (=6.93 Hz for Lac) (29). However, for more complicated spin systems such as 2HG, Glu, and Gln, analytic solution of spin evolution is difficult and requires numerical calculation (424445) or investigation at least in phantom. This approach can also incorporate the intra-pulse spin evolution particularly during slice selection (424445). The signal yield of coupled spins can substantially differ for different combinations of TE1 and TE2 for a given total TE (= TE1 + TE2) with a PRESS sequence (4146). Also, to minimize the signal loss of a target signal and maximize the suppression of spectral baseline, an optimal total TE is chosen as ≥ ~100 ms at 3T (161941). Optimal TE facilitates great improvement of the signal-to-background ratio of a target signal at the cost of its SNR, which is the primary purpose of spectral editing (41).
While a long TE method may provide an effectively isolated target signal, it is subject to quantitative error due to T2 relaxation, which may be altered in the diseased brain or in the progression of diseases (2147). Also, a long TE method with a PRESS sequence may require pulse sequence modification for individually adjustable TE1 and TE2.
Difference Editing
A difference editing method utilizes J-coupling as spectral contrast as in the long TE method, and has long been used in glioma for Lac editing against lipid that also has the major signal at ~1.3 ppm (48). Recalling that the J-evolution of the Lac doublet at ~1.3 ppm can be approximated by cos (π·J·TE) with J = 6.93 Hz, the Lac signal is inverted at TE = 1/J = 144 ms (because cos (π) = -1), and evolves back to positive signal at TE = 2/J = 288 ms (because cos (2π) = 1) (48). By subtracting the former from the latter, the target spectral region of the resulting 'difference' spectrum is contributed mainly by Lac (48). Alternative to this approach using two different TEs, frequency-selective RF pulses (a pair of editing pulses) can be used for difference editing, often with a set of spoiling gradient pulses (495051). In the case of 2HG (1516), the editing pulses are tuned at ~1.9 ppm, and yet indirectly influence the line shape of the multiplet at ~4.0 ppm due to J-coupling between the spins contributing to the two multiplets (Fig. 4). By subtracting the two spectra acquired at the same TE but with and without the editing pulses from each other, the target spectral region (~4.0 ppm) in the difference spectrum consists mainly of the signal from 2HG (Fig. 4). Note that although the 2HG signal at ~4.0 ppm has spectral overlap with Lac and mI, those Lac and mI spins responsible for the signals at this target spectral region do not have their J-coupled counterpart spins resonating in the vicinity of ~1.9 ppm (1516). Therefore, their signals at the target spectral region are canceled out by subtraction.
In difference editing, the pulse sequence optimization requires finding a TE that can yield a maximum signal after subtraction. In the case of using editing pulses, the choice of a TE is subject to the duration of the editing pulses, which are much longer than those pulses for spatial localization to achieve high spectral selectivity (1516). As such, the total TE is also indispensably long, which may therefore be subject to quantification errors inherent to long TE method. The difference spectra cannot provide comprehensive metabolic profiles. However, the spectrum acquired without the editing pulses may be used instead. As it requires subtraction of spectra with a relatively long scan time, all difference spectra methods are particularly subject to patient motion (29). For 2HG, the subtracted 2HG signal at ~4.0 ppm appears a doublet (Fig. 4), and the peak-to-peak distance of the doublet is very useful for examining the integrity of the edited 2HG signal. This is particularly so, given the spectral proximity of the target signal of 2HG to the strong water signal. A basic pulse sequence for difference editing is available commercially. For instance, in Siemens, a generic PRESS sequence can be used in combination with a MEGA module (49) implemented in the sequence for additional suppression of water and lipid. The frequency of the editing pulses needs to be adjusted accordingly, and for optimization of TE1 and TE2 separately it may also require sequence modification as with a long TE PRESS sequence.
2D
Two-dimensional methods are in use for high resolution nuclear magnetic resonance to identify the J-coupling network of spin systems (peak assignment) (52). The extension of the dimension of spectra is achieved by two time variables in the sequence-one for the time between the excitation and the onset of data acquisition (t1) and the other for the duration of data acquisition period (t2). For instance, in the correlation spectroscopy (5253), signal is acquired during the t2 period as in one-dimensional spectroscopy, but repetitively with different t1 values. The resulting spectra are expressed on a 2D frequency space (f1, f2) via the 2D fast Fourier transformation of the signal, S (t1, t2). The resolution of the spectra is determined not only by the number of data points during t2 period, but also by the number of experiments with different t1 values. Among the peaks in the diagonal (f1 = f2) and off-diagonal regions of the spectra, those off-diagonal peaks or cross-peaks provide information on correlations (J-coupling) between peaks, and therefore allow for unambiguous assignment of peaks (53). However, due to the long acquisition time required to obtain reasonable spectral resolution, the in-vivo application of 2D-MRS is limited only when a target spectral region is severely crowded with background signals as in the case with 2HG (15). Also, a 2D pulse sequence is usually unavailable in clinical scanners, and the method requires additional data post-processing for metabolite quantification (15).
Finally, optimal sequence parameters (e.g., TE) can differ for different designs of RF and gradient pulses, and at different field strength. Therefore, sequence optimization needs to be performed for the given MR scanner and pulse sequence.
Data Post-Processing
The LCModel (3854) is currently the most widely used 1H-MRS data post-processing software package, which performs spectral fitting in frequency-domain. The current version of LCModel employs an extended spectral basis set including modeled MMs and lipids (35365455), and therefore does not require a priori knowledge about spectral baseline. The MRUI (56) is another frequently used software package for metabolite quantification, which employs time-domain analysis. In general, one of such software packages is necessary for metabolite quantification for spectra obtained by a short TE method. For those edited spectra, spectral fitting may not be necessary if the target signal is effectively isolated from its background signals. The precision of spectral fitting is typically reported for individual metabolites in terms of the Cramer-Rao-Lower-Bound (CRLB) that sets a lower bound on the variance of the fitting estimate (4457). A CRLB of ≤ 20% is often used to indicate successful fitting (1112152229).
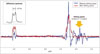
The representative spectra from IDH-WT and IDH-MT glioma patients obtained by short TE and long TE methods are shown in Figure 5, for which LCModel was used for data post-processing.
Reviews on In-Vivo 1H-MRS Studies in IDH-MT Gliomas
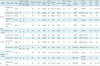
The 1H-MRS methods for identifying IDH-mutational status in gliomas in the previous in-vivo studies are summarized in Table 1.
Short TE
Pope et al. (14) report 100% sensitivity and 74% specificity of a short TE method, in 9 IDH-MT and 15 IDH-WT glioma patients with 4 false positive cases. The 2HG concentrations as measured by 1H-MRS and liquid chromatography-mass spectrometry (LC-MS) are highly correlated (r2 > 0.56); but 2HG concentrations (LC-MS) are not correlated with tumor grades. Andronesi et al. (15) compare performance of a short TE method to difference editing and 2D methods; while sensitivity and specificity are not reported, limited performance of a short TE method is shown, wherein 3 spectra from 2 healthy voxels and 1 IDH-WT tumor voxel result in false positive cases (including one case with CRLB > 20% from a healthy subject). Choi et al. (17) show a 77% sensitivity and 100% specificity for a short TE method in comparison to a long TE method. In a study on 1H-MRS performance in patients, Natsumeda et al. (18) report 100% sensitivity and 72% specificity where a 2HG cutoff concentration of 1.489 mM is used in differentiation between 2HG-positive and -negative cases in consideration of the limited SNR of 1H-MRS. In this study, 10 of 25 data (40%) from IDH-MT glioma patients and 9 of 27 data (33%) from IDH-WT glioma patients are excluded according to the data exclusion criteria based on the resulting 2HG concentrations and respective CRLB values. Interestingly, the survival rate of the IDH-MT glioma patients is significantly higher than the IDH-WT glioma patients (80% vs. 44.4%), corroborating previous reports (11); in addition, patients with high 2HG concentrations (> 1.489 mM) show a longer overall survival trend than those with low 2HG concentrations.
The performance of a short TE method is also tested in animal models at high field (2022). Given the heterogeneity of gliomas in humans, the use of animal models can provide a better comparison between the study cohorts with and without IDH-mutation (20). Lazovic et al. (20) report 100% sensitivity and specificity at 7T in mouse glioma models using human U87 glioma cells overexpressing IDH1-mutation. Such excellent performance of a short TE method most likely results from higher spectral SNR and dispersion of the spectra at high field, large voxel size and number of signal averages, and high 2HG concentrations (10–20 mM) in the animal models. Additionally, diffusion, perfusion, and T2-weighted (T2-mapping) MRI scans show no significant difference in the respective MRI measures between the animal groups with and without IDH-mutation. Using rat models of IDH1/2-mutant-overexpressing F98 glioma, Heo et al. (22) also describe the challenges with 1H-MRS of 2HG even at 9.4T. Given that spectral baseline is the primary factor hindering the differentiation between Glu and Gln (3738), that the main signal of 2HG directly overlaps with these metabolites, and that measured spectral baseline provides better information than those modeled (3940), they investigated the performance of a short TE method in combination with voxel-specifically measured spectral baseline, and report 100% sensitivity and 83% specificity.
Overall, the reported sensitivity and specificity of a short TE method ranges 77–100% and 72–100%, respectively, and there is a trend towards lower specificity than sensitivity. Despite the severe spectral overlaps, these results support the potential applicability of 1H-MRS in the non-invasive detection of 2HG. However, the reported limitation of the short TE method should be noted.
Long TE
Choi et al. (1617) report 100% sensitivity and specificity in two different patient studies with a long TE method. In comparison to a short TE method, the long TE method improves the sensitivity from 77% to 100% (17). Using a long TE method, de la Fuente et al. (19) investigate the impact of voxel size on the detectability of 2HG. Three different voxel sizes of < 3.4 mL, ≥ 3.4 and < 8 mL, and ≥ 8 mL result in 8% (2/24), 47% (16/34), and 91% (20/22) sensitivity. Also, 6 of the 6 voxels (voxel size ≥ 8 mL) from IDH-WT gliomas do not show 2HG signal at the target spectral region. In this study, 2HG concentrations are correlated with tumor cellularity but not with the degree of tumor cell proliferation. Importantly, 2HG levels gradually reduce following treatment with radiation and chemotherapy. A long TE method is also tested at 7T by Emir et al. (21) where the specificity from 29 healthy or IDH-WT glioma tissue is 93% (sensitivity data not shown explicitly). Although a small number of voxels is used, the 2HG concentrations are higher in IDH2-MT gliomas (n = 3) than in IDH1-MT gliomas (n = 7) in that study.
Overall, the reported sensitivity and specificity with a long TE method are ~90–100% for both, and appear better than those with a short TE method, most likely due to the effective isolation of the target 2HG signal and negligible contribution from spectral baseline at a total TE of ~100 ms (1617). However, as discussed by the authors (161721), the resulting 2HG content may be prone to quantitative errors resulting from signal loss due to relaxation. The signal loss arising from a long TE may also hinder the quantification of other metabolites in the edited spectra (21).
Difference Editing and 2D
Using a difference editing method (49), Choi et al. (16) acquire spectra from 7 subjects with either IDH-MT or -WT gliomas. Although the mutational status of the patients is not given explicitly, the diagnostic outcome with difference editing is comparable to a long TE method with 100% sensitivity and specificity. Andronesi et al. (15) also test a difference editing method (49) together with a 2D method in 10 humans including 2 IDH-MT glioma patients. In their study, the mean 2HG levels (normalized to Glu + Gln) from IDH-WT voxels are non-zero with both methods; however, they are substantially lower than with a short TE method.
To date, the performance of a difference editing method in IDH-MT gliomas is reported from only 2 studies with small numbers of subjects (1516)–only 1 study for a 2D method (15). However, given the effective isolation of a target signal provided by a difference editing method and the additional information for unambiguous peak assignment provided by a 2D method, these methods have potential applicability.
Alterations in the Concentrations of Other Metabolites in IDH-MT Gliomas
Pope et al. (14) report that voxels that result in the 4 false positive cases in their study have higher Glu and Gln levels than other IDH-WT voxels. This observation emphasizes the influence of the background signals on the quantification of 2HG in the spectral fitting. However, no difference in Glu and Gln concentrations are found between the study cohorts with and without IDH-mutation as measured by LC-MS. In contrast to these findings, Choi et al. (17) report reduced Glu and elevated Gln levels in IDH-MT gliomas relative to IDH-WT gliomas, but with no correlations with 2HG levels. Several other studies also report altered Glu and/or Gln levels in IDH-MT glioma patients (e.g., significantly lower Glu + Gln (18) and a trend of lower Glu (21)) and animal models (e.g., lowered Glu/Cho ratio (20)).
Significantly lowered GSH concentrations (1418) as well as a trend of lower GSH (21) are also reported in IDH-MT glioma patients. This may be due to reduced nicotinamide adenine dinucleotide phosphate hydrate as a result of IDH-mutation, which is involved in the regeneration of the reduced form of GSH, and therefore may potentially be associated with the pathogenesis and progression of the IDH-MT gliomas (14). In an animal study, however, there is no difference in GSH concentrations normalized to Cho between the animal groups with and without IDH-mutation (20). Pope et al. (14) also report high Cho/Cr ratios in IDH-MT gliomas relative to those in IDH-WT gliomas, and suggest increased cell density from IDH-mutation-mediated cell proliferation as a probable cause. In addition, Emir et al. (21) report trends of lower citrate, mI, Cho and Cr, and higher Lac, NAA + NAAG and glucose + taurine in IDH-MT glioma patients than in IDH-WT glioma patients.
Data Inclusion/Exclusion Criteria and Presentation of 2HG Concentrations
Depending on their quality, spectra may need to be excluded prior to metabolite quantification. For instance, de la Fuente et al. (19) estimate the full-width-at-half-maximum (FWHM) of Cr signal, and those spectra with FWHM of Cr ≥ 0.08 ppm (~10 Hz at 3T) are excluded. However, even after such data screening, indeterminate diagnostic cases frequently occur after spectral fitting if the resulting CRLBs of 2HG are larger than a cutoff CRLB for successful fitting (e.g., CRLB ≤ 20%). To address this issue, various data inclusion/exclusion criteria are reported in terms of a detectable limit of 2HG concentrations in combination with a cutoff CRLB. For instance, Choi et al. (16) use 2HG concentrations ≥ 1.5 mM with CRLB < 18% as the inclusion criteria for 2HG-positive cases. Natsumeda et al. (18) use different criteria for different metabolites in consideration of their different concentrations and thus different SNR in the spectra. The experimental settings in the previous studies are quite diverse (Table 1), and consequently the reported detection limits of 2HG concentrations are also quite different (151619), indicating the need for experimental setting-specific data inclusion/exclusion criteria.
Water signal is most widely used as an internal reference for the normalization of the 1H-MRS-measured concentrations of 2HG and other metabolites (14161718192122). Water-normalized metabolite content can be further converted into absolute concentrations using a priori knowledge (161719). Depending on the TE used for acquiring water-unsuppressed spectra, the water signal needs to be corrected for T2 relaxation (21). Alternatively, water-unsuppressed data need to be acquired using a STEAM sequence (17) which provides a shorter TE than a PRESS sequence. For spectra acquired at a long TE, T2 of metabolites can also be corrected based on the published data (161719). In this procedure, however, care must be taken as different tumor types and grades can result in different T2 of water and other metabolites (2147). By using water content as a reference, the reported ranges of 2HG concentrations in IDH-MT glioma voxels in patients are: 1.7–8.9 mM (16), 2–15 mM (18), and 2–10 umol/g (21). In addition to water, Glu + Gln (15), Cr (14), and Cho (20) are also used as an internal reference. In particular, Andronesi et al. (15) propose normalization of 2HG by Glu + Gln based on their potential inter-relationship (1258), and report that a 2HG/(Glu + Gln) ratio of > 1 could be specific for IDH1-mutations.
CONCLUSION
In this review, we focused on technical aspects of previous in-vivo 1H-MRS studies of 2HG. Given that different experimental protocols were used with different data inclusion/exclusion criteria in the previous studies, and that there was a large inter-patient variability in reported 2HG content, the relative performance of the different 1H-MRS methods may be best compared in the same study cohort with established procedures for screening, post-processing, interpretation and presentation of the data. 1H-MRS methods have individual pros and cons; hence, further technical development may be necessary in order to accurately quantify the target metabolite and better depict biochemical effects of mutation-dependent IDH activities as a consumer or producer of α-KG. However, as far as 'detection' of 2HG is concerned, these previous pioneering studies are in support of the diagnostic and prognostic potential of 1H-MRS in IDH-MT glioma patients. IDH-mutations and/or 2HG accumulations are recently identified in other cancers and disorders (5960616263646566). Therefore, the efficacy of 2HG as a 1H-MRS biomarker of IDH-MT gliomas should also be investigated thoroughly (18).




 XML Download
XML Download