

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Hepatocellular carcinoma (HCC) is the most common primary liver cancer and is the second most common cause of death from cancer worldwide, with an estimated 745000 deaths in 2012 (1). It is the fifth most common cancer among men (554000 cases) and the ninth most common cancer in women (228000) (1). The age-adjusted worldwide incidence rates per 100000 for men and women are 15.3 and 5.3, respectively (1). In men, the incidence rates are highest in Eastern and South-Eastern Asia (31.9 and 22.22, respectively), intermediate in Southern Europe (9.5) and Northern America (9.3), and the lowest in Northern Europe (4.6) and South-Central Asia (3.7) (1). In women, the rates are generally lower than those in men with the highest rates in Eastern Asia and Western Africa (10.2 and 8.1, respectively) and the lowest in Northern Europe and Micronesia/Polynesia (1.9 and 1.4, respectively) (1). In the United States, an estimated 23000 deaths from liver cancer occurred in 2014 (2). In this same year, an estimated 33190 new cases of liver cancer were expected (2). From 2006 to 2010, the rates of liver cancer increased by 3.7% per year in men and by 2.9% per year in women (2).
Hepatocellular carcinoma has a poor prognosis with an overall 5-year relative survival rate of 16% and survival decreases as patients are diagnosed with regional and distant stages of the disease (2). Only 41% of liver cancer patients are diagnosed at an early stage, while the majority of patients present with advanced disease. Curative treatments indicated for early HCC include resection, liver transplantation, and percutaneous ablation (34). Patients with early HCC can achieve a survival rate of 50–70% at 5 years after undergoing resection, liver transplantation, or percutaneous ablation (5). Non-curative treatments to improve survival in patients with unresectable HCC include locoregional therapies such as transarterial chemoembolization (TACE) and selective internal radiation therapy (SIRT) for intermediate HCC and sorafenib for advanced HCC (34).
Methods
A systematic literature search for yttrium-90 (Y90)-SIRT with glass microsphere studies (published, unpublished and ongoing) was carried out from August 19, 2014 to July 19, 2015, and it was updated on August 30, 2015. Two investigators developed and conducted the literature search. Studies were identified using database searches and citation searches of selected articles. The electronic database searched was PubMed (1965-present). Only articles in English were selected for the review and no date restrictions were applied to the search. The search was conducted using free-text terms and standardized subject terms appropriate for the specific database. Combinations of the following search terms were used: HCC, hepatocellular carcinoma, radioembolization, TARE, SIRT, Yttrium-90, Y90-SIRT, TheraSphere®, glass microspheres, therapy/treatment, safety, efficacy, and Sorafenib (Table 1). Ongoing and completed clinical trials were identified through searches of clinical trial databases (6). Study eligibility was assessed by a single investigator in an un-blinded manner. Studies were retained if they met the following criteria: 1) TheraSphere® or glass microspheres use in the treatment for HCC, 2) effect of Y90-SIRT with glass microspheres on early, intermediate or advanced HCC, or 3) safety and/or efficacy of Y90-SIRT with glass microspheres or Sorafenib for HCC. All study designs were accepted. Studies were excluded if their aim was to evaluate: 1) SIR-Spheres® or 2) resin-based microspheres as our main focus in this literature review was the treatment of HCC with glass microspheres which is currently approved by the Food and Drug Administration (FDA) under an humanitarian device exemption (HDE).
Yttrium-90 Selective Internal Radiation Therapy (Y90-SIRT)
The technique uses Y90 impregnated glass or resin microspheres, which are delivered through a catheter directly into the hepatic arteries (78). It takes advantage of the fact that primary and secondary hepatic tumors are vascularized mostly by arterial blood flow in comparison to healthy liver parenchyma which obtains its blood supply mainly from portal venous blood (7). The diameters of the glass and resin microspheres (20–30 microns versus 20–60 microns, respectively) allow them to become permanently embolized in the terminal arterioles of tumor (9). Y90 is a pure beta-emitter that disintegrates into stable zirconium-90 and has a half-life of 64.24 ± 0.30 hours (7810). The average β-emission is 0.9367 MeV, with a mean tissue penetration of 2.5 mm and a maximum tissue penetration of 10 mm (78). This allows delivery of high radiation doses to hepatic tumors while minimally affecting the healthy surrounding liver parenchyma unlike external radiation (3711).
There are two commercially available microspheres: TheraSphere® (MDS Nordion, Ottawa, Canada) and SIR-Spheres® (Sirtex Medical Ltd., Lane Cove, Australia) (8). In 1999, the United States FDA approved the glass microspheres (TheraSphere®), under an HDE, for radiation treatment or as a neo-adjuvant to surgery or transplantation in patients with unresectable HCC who could have placement of appropriately positioned hepatic arterial catheters, and later it approved the use of TheraSphere® in patients with portal vein thrombosis (12). The FDA approved the use of resin microspheres (SIR-Spheres®) in 2002 via a premarket approval for its use in the treatment of unresectable metastatic colorectal cancer to the liver with adjuvant chemotherapy with floxuridine (13).
Pre-Treatment Evaluation
Prior to undergoing Y90-SIRT, patients must undergo pre-treatment evaluation to ensure that the therapy is successful (1415). This pre-treatment evaluation is performed 1–2 weeks prior to the procedure and it consists of the following studies: clinical studies, laboratory tests, and imaging (triphasic liver CT or MRI, angiography, and a technetium-99m labeled macroaggregated albumin [99mTc-MAA] scan) (1416).
Clinical Evaluation
The clinical evaluation is performed by a multidisciplinary team which determines a patient's candidacy for Y90-SIRT. The multidisciplinary team may consist of the following specialists depending on the local practices in the institution involved: surgical/medical oncologists, transplant surgeons, hepatologists, radiologists, and interventional radiologists (14). During the clinic visit, evaluation of a patient's performance status per the The Eastern Cooperative Oncology Group (ECOG) is completed (14). Patients with elevated baseline bilirubin (> 2 mg/dL), a Child-Pugh class C (score ≥ 10), an ECOG performance status ≤ 2, and an estimated radiation dose to the lungs > 30 Gy in a single treatment or 50 Gy in multiple treatments are not considered ideal candidates for Y90-SIRT (914).
Laboratory Tests
Patients with HCC undergo laboratory tests that include liver function tests, tumor markers, serum bilirubin, serum albumin, and the prothrombin time (PT)/the international normalized ratio (14). Patients with cirrhosis are classified based on the commonly used Child-Pugh classification which includes an assessment of encephalopathy and ascites in addition to the laboratory tests.
Imaging Evaluation
Triphasic Liver CT or MRI
The imaging evaluation consists of triphasic liver CT or MRI to evaluate variant vascular anatomy and to assess the extent and location of the hepatic tumor and its hypervascularity (714). CT scans may identify several characteristics of primary HCC that are associated with a favorable response to Y90-SIRT such as well-defined tumor margins, central hypervascularity pattern, and hepatopulmonary fraction (17).
Angiography
Angiography is useful for arterial mapping as it provides the interventional radiologist with an assessment of the hepatic arterial anatomy, variant vasculature, and patency of the portal vein (14). It is also helpful for the occlusion of extrahepatic arteries, which supply the liver, with coil embolization (714). Some extrahepatic arterial branches that may be coil embolized prior to therapy are: GDA, RGA, accessory left gastric artery, cystic artery, falciform ligament artery, phrenic arteries, inferior esophageal artery, supraduodenal artery, and retroduodenal artery (7141819). These extrahepatic arterial branches are occluded prior to radioembolization to reduce extrahepatic diffusion of the microspheres which can result in significant side effects and/or to minimize delivery of only partial treatment during administration of the microspheres via the main hepatic vessel (714). Between 17% to 30.8% of liver tumors and, in particular HCC, receive their blood supply from extrahepatic arterial branches (7). Development of extrahepatic branches can result from a history of chemoembolization, exophytic tumors, and occlusion of the main arterial pedicle and size of the tumor volume. In 63% of the tumors with development of extrahepatic branches, tumor size was larger than 6 cm (7).
Two commonly occluded extrahepatic arteries are the GDA and the RGA (720). The GDA which branches off the common hepatic artery can be identified on CT and arteriography and is occluded by coiling (hydrocoils or metal coils) prior to the treatment as reflux carries a risk of pancreatitis and gastroduodenal ulceration (7). The study by Vesselle et al. (7) recommends that the GDA should be occluded as proximal as possible as extrahepatic branches may arise very early and that collateral branches should also be occluded. However, occlusion of the GDA is contraindicated in the presence of a retrograde flow as there is no benefit and it may prove harmful to the patient (7). Another commonly occluded artery is the RGA, which arises from the main hepatic artery in 45–57% of patients (7). Catheterization of the RGA can prove to be technically difficult due to its narrow diameter, tight anatomical angle, and anatomical variants (7). In addition to using a microcatheter, a detachable hydrocoil or remodeling balloon can be used (7).
Technetium-99m Labeled Macroaggregated Albumin (99mTc-MAA) Scan
Prior to treatment, the patient must also undergo a 99MTc-MAA scan to assess pulmonary and splanchnic shunting and to confirm that there is no extrahepatic uptake (714). A mixture of albumin particles similar to the size of the glass microspheres (25–35 microns) are bound to the gamma-emitting radioisotope 99mTc (21). The albumin particles are then imaged via single photon emission computed tomography gamma camera scintigraphy to detect shunting and determine the lung shunt fraction (LSF) (21). The LSF is used to calculate the appropriate dose that should be delivered to the lungs in an attempt to minimize the risk of radiation pneumonitis (9).
Dose Calculation for TheraSphere® (222324)
To determine the liver volume for which the Y90 glass microspheres are delivered (i.e., volume of distribution) a 3-dimensional reconstruction of the target site is performed using CT or MR imaging. To calculate the mass of infused liver tissue (in kg), a conversion factor of 1.03 g/cm3 is used. The required activity for injection and the dose delivered to the target are calculated by the following formula:
Where A is the net TheraSphere® activity delivered to the liver, D is the dose administered to the target liver mass, and M is the target liver mass.
When the LSF and residual activity (R) in the vial after treatment are taken into account, the actual dose delivered to the target mass (Gy) is calculated by the following formula:
Procedure
After pre-treatment evaluation, the patient will undergo Y90-SIRT which is done on an outpatient basis (21). Under fluoroscopic guidance, glass microspheres (about 1–8 million glass spheres) are delivered to the liver via a catheter placed into the femoral artery, which is then guided into the hepatic artery and eventually positioned into the diseased lobe/segment of the liver by following the branch of the hepatic artery (21). Once the catheter is properly positioned, the microspheres are infused at a rate similar to that of the hepatic arterial flow over a period of 3–5 minutes (9). Delivery of the glass microspheres is dependent on the hepatic arterial flow distal to the catheter tip. It is necessary to ensure that the catheter does not occlude the vessel in which it is positioned in order to prevent reflux secondary to vessel spasm (9).
Post-Treatment Assessment
After patients receive their treatment, they undergo post-treatment imaging and laboratory evaluation to assess the response to treatment or lack thereof. Y90-SIRT is associated with low toxicity and patients who receive an administered activity of less than 3 GBq can be released without contact restrictions according to the Nuclear Regulatory Commission contact scenario (25). The time interval for obtaining post-treatment imaging and laboratory evaluation varies among authors and clinical institutions (20). The study by Riaz, Awais, and Salem obtained triphasic CT or MRI at 1 month following treatment and at 3 month intervals following the first post-treatment as it may take 3–6 months for the optimal response (size reduction) to occur (14). Laboratory studies obtained 1 month following Y90-SIRT include liver function studies, complete blood count and tumor markers (alpha-fetoprotein for HCC) (14).
Tumor Response Assessment Following Y90-SIRT
Tumor response assessment following Y90-SIRT can be performed with conventional cross-sectional imaging such as CT and MRI (917). There is a lack of standardization of functional imaging in HCC and response assessment based on anatomical methods is considered as the standard (2627).
Four commonly used guidelines to assess tumor response following therapy are: World Health Organization (WHO) (28) (bidimensional), Response Evaluation Criteria in Solid Tumors (RECIST) (29) (unidimensional), Modified Response Evaluation Criteria in Solid Tumors (mRECIST) (30) (unidimensional), and the European Association for the Study of the Liver (EASL) (31) (necrosis). The RECIST guideline was amended in 2010 to become the mRECIST (30). The mRECIST adopted the concept of viable tumor, which shows arterial enhancement on contrast-enhanced radiologic imaging techniques, thus enabling an evaluation of the tumor response after therapeutic strategy (30). The EASL guidelines address the limitations of the guidelines of the WHO and RECIST, which based their guidelines on systemic therapies resulting in limitations when applied to locoregional therapies such as Y90-SIRT (31).
The study by Rhee et al. (32) showed that diffusion-weighted imaging (DWI) functional MR may assist in early determination of the response or failure of Y90-SIRT in HCC. Unlike MR anatomic imaging studies which are able to assess tumor response until 3 months after treatment, DWI showed that imaging changes at 1 month preceded anatomic size changes seen at 3 months following Y90-SIRT (32). Earlier detection would allow for repeat treatment or alternative therapy such as TACE to be given sooner to patients rather than waiting 3 months to determine the treatment response (32).
In an effort to better identify the tumor response and therapy-related changes in serum markers after Y90-SIRT, a retrospective single-center study assessed the tumor response by using the RECIST 1.1, mRECIST, and Choi criteria (33). Using these three guidelines in addition to the model for end stage liver disease and the serum C-reactive protein, the study was able to create a prognostic model which could predict survival probability for individual patients as early as one month after treatment (33). However, this prognostic model needs to be validated further by performing larger prospective treatment studies.
Complications
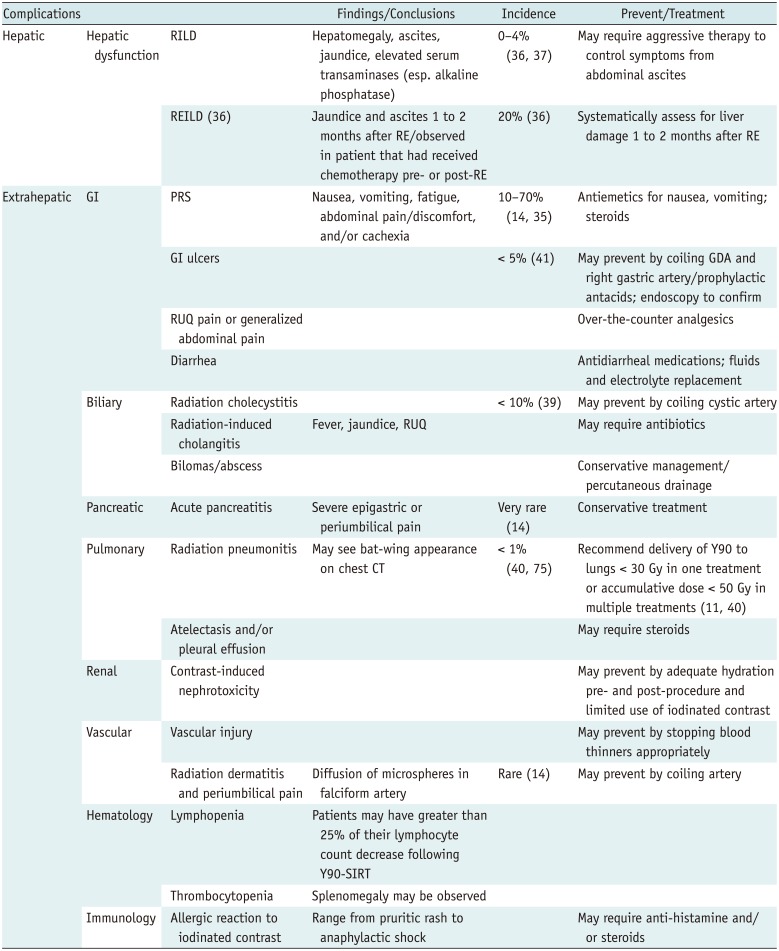
Although studies have shown that Y90-SIRT can be considered a safe and efficacious treatment for HCC, complications associated with the therapy can occur (Table 2) (34). Some patients may experience a post-radioembolization syndrome (PRS) which consists of nausea, vomiting, fatigue, abdominal pain/discomfort, and/or cachexia (14). Hospitalization is rarely required and the incidence of PRS ranges from 10% to 70% (1435). Extrahepatic microsphere delivery or radioactivity affecting surrounding structures can result in hepatic dysfunction, biliary system complications, radiation pneumonitis, gastrointestinal (GI) complications, acute pancreatitis, radiation dermatitis, and lymphopenia (14). Other complications include: thrombocytopenia, vascular injury, contrast-induced nephrotoxicity, and allergic reaction to iodinated contrast media (14).
A serious hepatic complication after Y90-SIRT is radiation-induced liver disease (RILD) (14). The incidence of RILD ranges from 0% to 4% and it occurs due to radiation exposure of healthy hepatic parenchyma (143637). Clinically, patients develop hepatomegaly, ascites, jaundice and elevated serum transaminases, especially alkaline phosphatase (37). Treatment involves aggressive therapy to control symptoms of abdominal ascites (37). Sangro et al. (38) further described radioembolization-induced liver disease (REILD) in 20% of patients who had undergone chemotherapy either before or after radioembolization. Patients with REILD presented clinically with jaundice and ascites as late as 1 to 2 months post-radioembolization. Post-radioembolization biliary complications include radiation cholecystitis (may be prevented by identifying and coiling the cystic artery (1819)), radiation-induced cholangitis, and bilomas/abscess (14). The incidence of post-radioembolization biliary complications is less than 10% and patients with prior surgeries involving the ampulla of Vater have a higher risk (1439). Less than 1% of patients will present with radiation pneumonitis and it is recommended that delivery of Y90 to the lungs should be less than 30 Gy in one treatment or the cumulative dose should be less than 50 Gy in multiple treatments (40). Patients with GI complications may present with diarrhea or ulcers. GI ulcers occur in less than 5% of patients and prophylactic coil embolization of the GDA and the RGA may help prevent sequelae (71441). Acute pancreatitis may present with severe epigastric pain and with elevated serum lipase and amylase levels (14). Although diffusion of microspheres in the extrahepatic arteries such as the falciform artery is rare, it may result in radiation dermatitis with periumbilical pain (714). Patients may have a greater than 25% decrease in their lymphocyte count following Y90-SIRT without an increase in the incidence of opportunistic infections (111434).
Y90-SIRT Outcomes
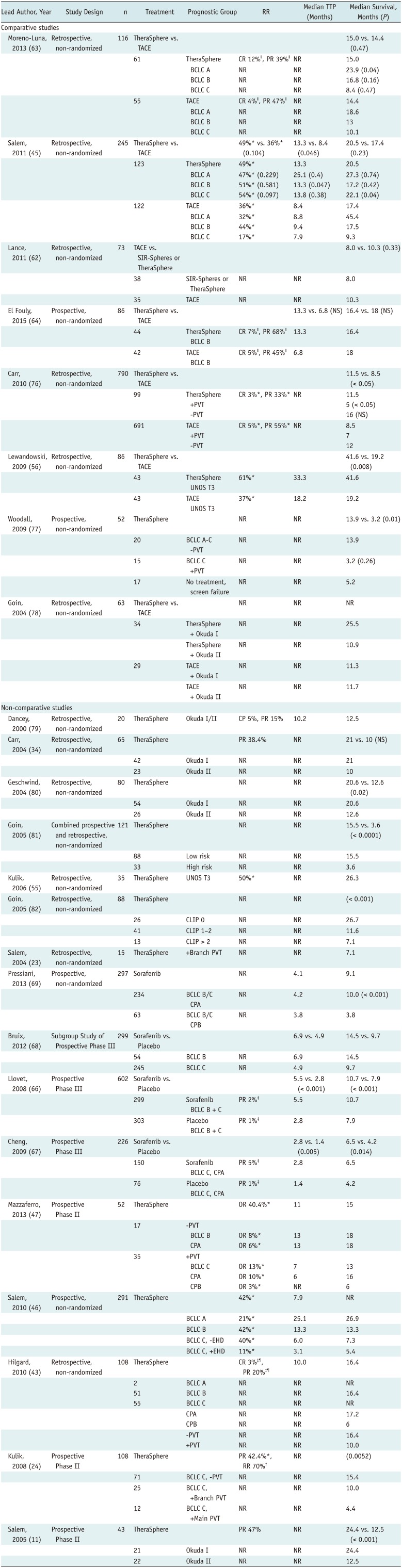
The majority of published studies on the treatment of HCC patients with Y90-SIRT are retrospective or small, non-controlled prospective studies, and therefore, they are only supported by level II-2 and II-3 evidence (42). There is a lack of large, randomized, controlled trials (Table 3). Studies have reported improved median survival in patients with intermediate- to advanced-stage HCC following Y90-SIRT (median 7–41.6 months) (24384344). Objective response rates vary between 35–70% among studies depending on the guideline criteria used (24384445). Approximately 20% of patients present with liver-associated toxicity and treatment-related deaths are estimated to occur in about 3% of patients (46).
Portal Venous Thrombosis (PVT)
A common indication for Y90-SIRT is HCC patients with portal venous thrombosis (PVT), which develops in approximately one third of all patients with unresectable HCC (24). Y90-SIRT causes minimal occlusion of the hepatic arteries, and it is therefore safe in the setting of PVT (16). Kulik et al. (24) conducted the first large-series analysis investigating the use of Y90-SIRT in the setting of PVT. The phase II study analyzed Y90-SIRT in 108 HCC patients with and without PVT (34% versus 66%, respectively) and reported partial response rates of 42.4% (size) and 70% (necrosis) (24). Patient survival varied according to the presence of cirrhosis and location of PVT. A phase II study conducted by Mazzaferro et al. (47), which assessed the efficacy of Y90-SIRT in patients with intermediate or advanced HCC, reported that the median time to progression (TTP) was 11 months with no significant difference between PVT versus no PVT (7 months vs. 13 months, respectively), median overall survival was 15 months with a nonsignificant trend in favor of patients without PVT (18 months) versus with PVT (13 months), objective response was 40.4%, and mortality at 30––90 days was 0–3.8%.
In 2010, the study by Salem et al. (46) confirmed the positive outcomes of Y90-SIRT in the treatment of 291 patients with HCC. This was a single-center, prospective, longitudinal cohort study that investigated long-term outcomes, response rate (size and necrosis), TTP and survival stratified by Child-Pugh, United Network for Organ Sharing (UNOS), and Barcelona Clinic Liver Cancer. Survival times differed between patients: Child-Pugh A (17.2 months), Child-Pugh B (7.7 months), and Child-Pugh B with PVT (5.6 months). The overall TTP was 7.9 months. TTP was longer for Child-Pugh A and B without PVT (15.5 months versus 13 months, respectively) in comparison to those with PVT (5.6 months versus 5.9 months, respectively) (46). The 30-day mortality rate was 3% and the response rates were 57% and 42% based on EASL and WHO criteria, respectively (46). That same year, a European study by Hilgard et al. (43) analyzed Y90-SIRT in 108 patients with advanced HCC and confirmed its safety and efficacy. TTP was 10.0 months with an overall survival of 16.4 months. They observed complete and partial response by necrosis criteria in 3% and 37%, respectively.
Lobar or Segmental Biliary Tract Obstruction
Yttrium-90 Selective Internal Radiation Therapy has been reported to be safe in patients with lobar or segmental biliary tract obstruction and normal bilirubin levels (2 mg/dL or lower) (48). A retrospective study of 12 patients, with a median overall follow-up time of 22.9 months, showed no evidence of therapy-related progressive leukocytosis, bilirubin increase, or biliary complications (infection, sepsis, biliary necrosis/stricture, abscess, or biloma formation) after Y90-SIRT (48).
Novel Concepts
The use of Y90-SIRT has led to the discovery of several novel concepts which may help patients who are undergoing potentially curative resection (4950). One of them is the controversial downstaging as a bridge to liver resection or transplantation in selected candidates (1651525354). Kulik et al. (55) reported that following Y90-SIRT, 19 of 34 (56%) patients were successfully downstaged from UNOS T3 to T2, and of these patients, eight (23%) underwent liver transplantation. Lewandowski et al. (56) concluded that Y90-SIRT outperforms TACE in downstaging HCC in patients from UNOS T3 to T2 (58% versus 31%, respectively). Y90-SIRT has been shown to be a safe and effective treatment for patients with unresectable HCC and transjugular intrahepatic portosystemic shunt (TIPS) who are awaiting liver transplantation. In the study by Donahue et al. (57), six of 12 patients with existing TIPS underwent liver transplantation after Y90-SIRT. Ibrahim et al. (58) reported that Y90-SIRT appears to be a feasible, safe and effective treatment option for patients with unresectable caudate lobe HCC and had the potential to downstage. Eight out of 291 patients were downstaged to within transplantation criteria. Four patients (50%) were downstaged from UNOS T3 to T2, three patients underwent liver transplantation, and one of the patients despite being downstaged was unable to undergo transplantation, given the comorbid conditions. Moreover, downstaging can also be achieved in patients with PVT (59).
A second novel concept termed "radiation lobectomy" is observed in HCC patients whose right-lobe disease is treated with Y90-SIRT (164950). After Y90-SIRT treatment, the irradiated lobe undergoes atrophy and the contralateral lobe undergoes hypertrophy, as opposed to portal vein embolization which can induce hypertrophy but does not treat HCC (1660).
Y90-SIRT with Glass Microspheres versus TACE in Intermediate Stage HCC
Transarterial chemoembolization is the treatment of choice for patients with intermediate stage HCC, but studies have shown that Y90-SIRT may have a role in subgroups of these patients (16). It is difficult to perform randomized controlled trials comparing TACE versus Y90-SIRT.
In comparison to Y90-SIRT, TACE involves premedicating patients (i.e., antibiotics, antiemetics, and narcotics) and hospitalization ranging from 1 to 5 days following treatment for post-embolization syndrome (16). Moreover, prospective data comparing the efficacy with regard to response and/or survival between Y90-SIRT and TACE in patients with intermediate HCC are lacking.
In 2011 Salem et al. (45) published a large comparative effectiveness study. The retrospective study of 245 patients who received either TACE (122 patients) or Y90-SIRT (123 patients), reported that although TTP was longer after Y90-SIRT than after TACE (13.3 months versus 8.4 months, respectively, p = 0.046), median survival times were not statistically different between the two treatment groups in patients with intermediate disease (17.2 months versus 17.5 months, respectively, p = 0.42) (45). Another retrospective study showed there was no significant difference in survival between Y90-SIRT and TACE (median 8 months versus 10.3 months, respectively, p = 0.33) (62). This study further showed that post-embolization syndrome was significantly more severe in patients who underwent TACE resulting in increased total hospitalization rates (62).
The retrospective case-control study by Moreno-Luna et al. (63) in 2013 showed that there was no significant difference in efficacy between Y90-SIRT and TACE. The median survival did not differ between Y90-SIRT (15.0 months) and TACE (14.4 months). The two-year survival was 30% for Y90-SIRT and 24% for TACE. Complete tumor response was more common after Y90-SIRT (12%) than after TACE (4%). However, Y90-SIRT patients reported more fatigue, had less fever and required less hospitalization than patients treated with TACE. The study by El Fouly et al. (64) in 2014 reported similar findings during the comparative analysis between TACE and Y90-SIRT in the treatment of 86 patients with intermediate stage HCC. Both treatments resulted in similar median overall survival rates (18 months for TACE versus 16.4 months for Y90-SIRT) and the TTP was not statistically different between treatments. However, the number of treatment sessions, total hospitalization time, and rate of adverse events were significantly higher in the TACE cohort. Future studies comparing Y90-SIRT and TACE should also assess their cost-effectiveness in therapy for intermediate stage HCC, given the increased hospital stay due to complications from repeated TACE treatments.
Although studies have not shown statistically significant differences in efficacy or survival between Y90-SIRT and TACE, Y90-SIRT seems to be better tolerated with significant differences in length of hospital stay and post-embolization symptoms. In addition, Y90-SIRT outperforms TACE with regard to downstaging and quality of life measures. As discussed previously, the ability to downstage from UNOS T3 to T2 as a bridge to liver transplantation was achieved more frequently with Y90-SIRT (58%) than with TACE (31%) (56). In 2013, the study by Salem et al. (65) demonstrated that Y90-SIRT outperformed TACE by validated quality-of-life (QoL) measures. The prospective study of 56 patients with HCC who underwent Y90-SIRT versus TACE (29 versus 27, respectively) showed that although patients who received Y90-SIRT had a larger tumor burden, they had higher QoL scores in comparison to patients who received TACE.
Y90-SIRT with Glass Microspheres versus Sorafenib in Advanced Stage HCC
The treatment of choice in patients with advanced stage HCC is sorafenib and it is associated with an overall survival of 6.5–14.5 months (4366676869). It is difficult to compare the efficacy of Y90-SIRT with sorafenib in advanced HCC through well-designed randomized controlled studies, given the high probability of crossover among treatment groups as HCC progresses. No study directly comparing sorafenib with Y90-SIRT with glass microspheres is currently available. However, the observational cohort study by Hilgard et al. (43) showed that in comparison to the phase III trial which led to the approval of sorafenib (SHARP trial), the median overall survival in patients with advanced HCC treated with Y90-SIRT was slightly longer (16.4 months) than that in patients with advanced HCC treated with sorafenib (10.7 months) (66). In addition, unlike Y90-SIRT, sorafenib has been shown to have significant side effects, which result in treatment discontinuation (44%), dose reduction, or withdrawal (64%) (6669).
Future Prospects
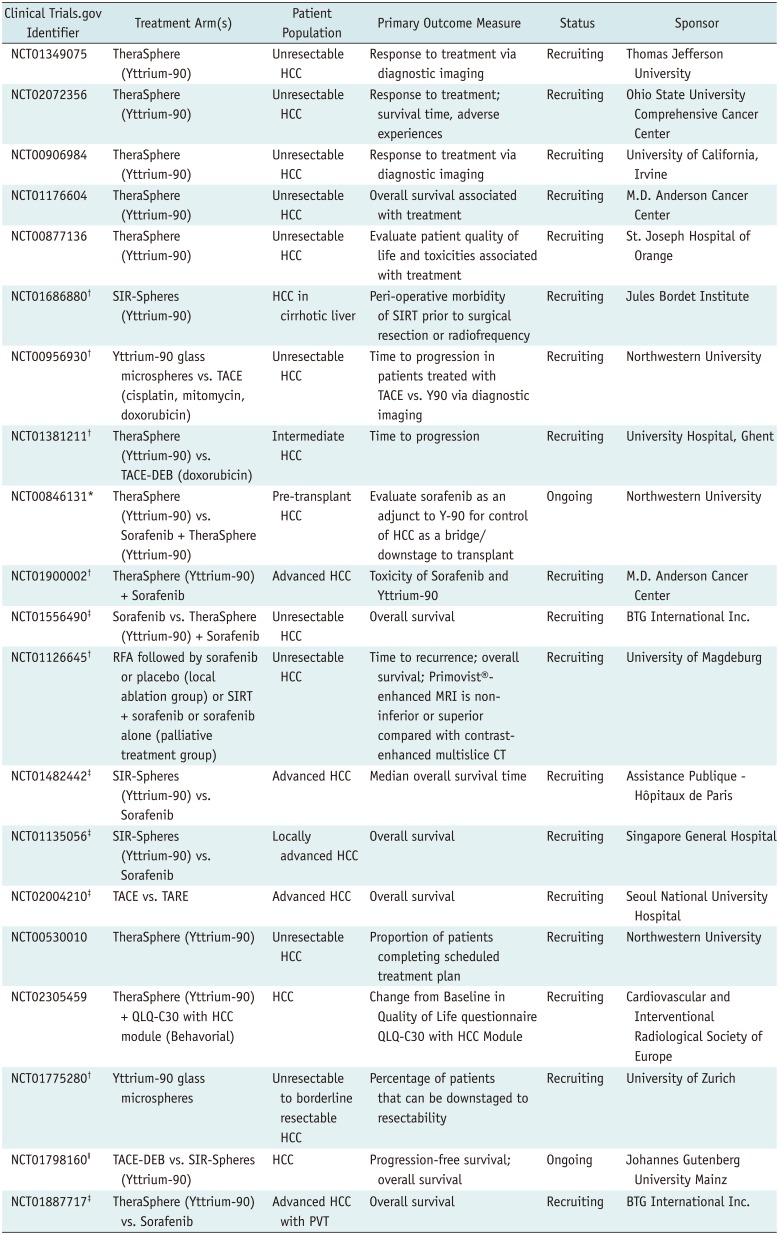
There are currently 16 active clinical trials investigating the use of Y90-SIRT with glass microspheres for treatment of HCC (Table 4) (6). In the United States, there are studies investigating the use of Y90-SIRT for the treatment of unresectable HCC (NCT01349075, NCT02072356, NCT00906984, NCT01176604, and NCT00877136) and assessing the safety of Y90-SIRT compared to radiofrequency prior to surgical resection in patients with HCC (NCT01686880) (6). The PREMIERE trial in the United States is comparing Y90-SIRT with TACE in patients who are not candidates for radiofrequency ablation or in patients with unresectable HCC (NCT00956930) (6). The European TRACE trial is a multicenter randomized control study comparing TARE with TACE for the treatment of HCC (NCT01381211) (6).
The good toxicity profile of Y90-SIRT makes it an alternative or adjunct to treatment with sorafenib (70). In the United States, a prospective randomized trial is studying the role of Y90-SIRT alone or in combination with sorafenib in the treatment of HCC patients who are awaiting liver transplantation (NCT00846131) and a phase II study is investigating the role of Y90-SIRT with sorafenib in advanced HCC (NCT01900002) (6). The STOP-HCC study, which is being conducted in the United States and Europe, is comparing sorafenib with and without Y90-SIRT (NCT01556490) (6). The outcomes of these trials may result in the incorporation of Y90-SIRT with glass microspheres into the treatment guidelines as a standard therapy option for patients with intermediate and advanced stage HCC.
CONCLUSION
Although the use of Y90-SIRT in treating liver malignancies dates back to the 1960s (717273), it has recently begun to gain clinical acceptance as a promising treatment option for patients with intermediate and advanced HCC (8). Multiple studies have provided compelling data which suggest that Y90-SIRT in comparison to TACE, has a higher tumor response, less post-embolization symptoms, better downstaging outcomes, and provides a higher QoL. However, the EASL, the European Organization for Research and Treatment of Cancer, and the American Association for the Study of Liver Diseases do not currently recommend Y90-SIRT as a standard therapy for intermediate or advanced HCC outside clinical trials (70). This clinical lack of enthusiastic approval stems from the fact that there is a lack of research and evidence from large-scale randomized controlled trials. Nonetheless, with the growing body of level 2 and level 3 evidence, Y90-SIRT has found a place in the guidelines adopted by the European Society for Medical Oncology, the European Society of Digestive Oncology, and the National Comprehensive Cancer Network (21). Y90-SIRT may become widely accepted and may be incorporated into the treatment guidelines if further research shows reproducibility, multicenter implementation, and economic feasibility.

 XML Download
XML Download