

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
A quadricuspid aortic valve (QAV) is a very rare congenital cardiac anomaly with an estimated prevalence of 0.008–0.033% by autopsy and 0.013–0.043% by echocardiography (12). It is rarely detected incidentally but is a well-recognized cause of significant aortic regurgitation (AR) requiring surgical treatment (3456). In addition, QAV is often associated with other congenital cardiovascular malformations (78). Therefore, accurate knowledge of QAV morphology, significant valve-related complications, and other associated congenital cardiovascular malformations would be helpful for proper management, including the surgical approach.
Transthoracic echocardiography (TTE) is now widely used for anatomical and functional evaluations of aortic valvular heart diseases (9). Retrospective electrocardiography (ECG)-gated multidetector computed tomography (MDCT) allows for high spatial resolution anatomy-based image reconstruction of the aortic valve during the entire cardiac cycle. Accordingly, ECG-gated MDCT has been expanded to a comprehensive evaluation of aortic valve diseases by providing morphological assessments and functional cine imaging while measuring stenotic aortic valve area and regurgitant orifice area (ROA) (101112). In addition, dual-source CT with improved temporal resolution provides simultaneous morphological assessments of the aortic valve, coronary artery, and ascending aorta simultaneously (13). More cases of QAV have been identified as a result of multi-imaging applications to aortic valve disease (1415). However, most QAV studies have been isolated case reports or review articles based on surgical results or echocardiography findings because of its rarity (3456). Furthermore, QAV classification based on the sizes of the four cusps is dependent on echocardiography or intraoperative findings. Until now, there are no published studies on the morphological and functional evaluation of QAV using cardiac computed tomography (CCT). Therefore, we hypothesized that CCT would be useful to characterize QAV morphology and function based on planimetric measurements. The aim of the present study was to identify the morphological and functional features of QAVs on CCT in 11 patients.
Go to : 
MATERIALS AND METHODS
Patients
The Konkuk University Medical Center database was queried for patients diagnosed with QAV by TTE, CCT, or surgery between June 2008 and January 2014. Patient sex, age, body habitus, race, and medical history were retrieved from the database. CCT was performed to evaluate coronary artery anomalies and stenosis, aortic valve morphology, the presence and extent of aortic valve cusp calcification, and the dimensions of the ascending aorta. This retrospective study was approved by our Institutional Review Board, and the requirement for patient informed consent was waived due to its retrospective nature.
Image Acquisition and Analysis
CCT Studies
All CT examinations were performed using a first-generation dual-source CT scanner (Somatom Definition, Siemens Medical Solutions, Forchheim, Germany) and the following scanning parameters: collimation, 32 x 0.6 mm; slice acquisition, 64 x 0.6 mm, using the z-flying focal spot technique; gantry rotation time, 330 msec; pitch, 0.20–0.43, adapted to the heart rate (HR); tube voltage, 100 or 120 kV; and tube current-time product, 320 mAs per rotation. A non-enhanced, prospective ECG-triggered CT scan was performed before the helical scan. ECG-based tube current modulation was implemented for CCT, except for patients with a mean HR > 80 beats per min (bpm) or those with an arrhythmia.
Patients with a pre-scan HR > 65 bpm were administered 50–100 mg metoprolol per oral, and all patients received 0.6 mg nitroglycerin sublingually. Contrast material was administrated at a rate of 4.5 mL/s via a dual-head power injector using bolus tracking and a three-phase injection protocol. First, 70–80 mL iopromide (Ultravist 370®, Bayer Healthcare, Berlin, Germany) was administered. Then, 45 mL of a 70-to-30% blend of contrast media and saline was administered. Finally, 45 mL of saline was given.
Cardiac computed tomography images were reconstructed with a slice thickness of 1.0 mm, and the reconstruction increment was set to 0.5 mm. Images were reconstructed with a section thickness of 3 mm and a reconstruction increment of 1.5 mm to quantify the coronary artery and aortic valve calcium score such as the Agatston score. The CCT datasets reconstructed at the optimal mid-diastolic-and end-systolic phases and at every 10% of the cardiac cycle were transferred to an external workstation (Vitrea 2, Vital Images, Plymouth, MN, USA) and reviewed by applying multiplanar reformation and a four-dimensional cine technique. Post-processing included both static and cine images of the aortic valve in double-oblique short-axis planes. Several cross-sectional transverse images during early systole (10–20% of the R-R interval) and mid-diastole (60–70% of the R-R interval) were reconstructed for the morphological and functional aspects of the aortic valve.
Aortic valve calcium volume score and coronary artery calcium score were evaluated using CaScore software (Siemens Medical Solutions). The aortic valve calcification grade was categorized as absent, mild, moderate, or severe as described by Willmann et al. (16). ROA and stenotic aortic valve area were measured using CT planimetry at mid-diastole and early systole, respectively. Individual valvular cusp area was also planimetrically measured by drawing region of interest along the outline of cusps at mid-diastole (Fig. 1). QAVs were diagnosed if the "4-leaf clover" was present during diastole (14). QAV was classified according to the Hurwitz and Robert's classification (2), using CT planimetry of the valve cusp area at mid-diastole, which was adopted by an echocardiographic study: type A (four equal cusps), type B (three equal cusps and one smaller cusp), type C (two equal larger cusps and two equal smaller cusps), type D (one large, two intermediate, and one small cusp), type E (three equal cusps and one larger cusp), type F (two equal larger cusps and two unequal smaller cusps), and type G (four unequal cusps) (Fig. 2). Mean cusp area was calculated with similar cusps except for the smallest or largest one. We considered the cusps to be roughly equal in size when the difference was within 10% of the mean value because no reference has defined cusp equality. In addition, the definition of accessory cusp has not been accurately specified in previous reports; thus, we arbitrarily defined it as the smaller one of the two remaining cusps, except for the right coronary cusp (RCC) and left coronary cusp (LCC). We also measured the diameter of the ascending aorta at four different levels during early systole: level 1, aortic annulus, defined as the hinge points of the aortic valve cusps; level 2, mid-point of the aortic sinuses of Valsalva; level 3, sinotubular junction; and level 4, tubular portion of the ascending aorta at the maximum dimension level (Fig. 3). The quality of the aortic valve CCT images was determined using a 4-point subjective ranking scale as follows: 1, poor; 2, fair; 3, good; 4, excellent. Poor image quality; non-diagnostic image quality with poor delineation of the aortic valve, fair image quality; diagnostic image quality with suboptimal image quality of the aortic valvular anatomy, good image quality; diagnostic image quality with good valvular anatomy visibility, excellent image quality; diagnostic image quality with clear delineation of the valvular structure (17). All measurements were performed in consensus by two independent experienced readers (with 12 and 4 years of experience in cardiovascular imaging) who were blinded to the clinical data and surgical reports of the patients.
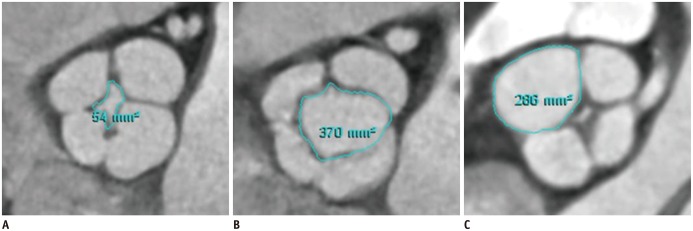 | Fig. 1Measurement of regurgitant orifice area (A) at mid-diastole, opening area (B) at early-systole, and individual valve cusp area (C) at mid-diastole in patient with quadricuspid aortic valve assessed by planimetry on cardiac computed tomography.
|
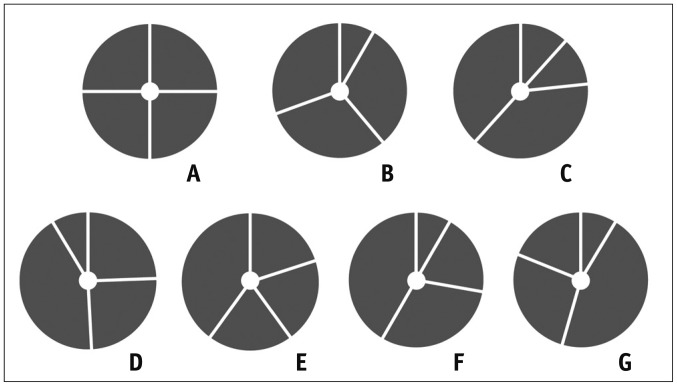 | Fig. 2Classification of quadricuspid aortic valve according to Hurwitz and Robert's classification.
A. Four equal cusps. B. Three equal cusps and one smaller cusp. C. Two equal larger cusps and two equal smaller cusps. D. One large, two intermediate, and one small cusp. E. Three equal cusps and one larger cusp. F. Two equal larger cusps and two unequal smaller cusps. G. Four unequal cusps. Adapted from Hurwitz and Roberts. Am J Cardiol 1973;31:623-626 (2).
|
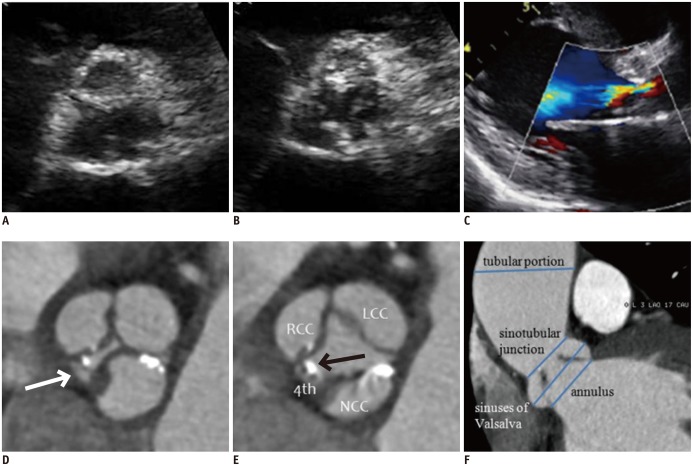 | Fig. 352-year-old man with Hurwitz and Robert's type F quadricuspid aortic valve combined with dilatation of ascending aorta.
A, B. Parasternal short-axis transthoracic echocardiographic images during diastole (A) and systole (B) show aortic valve. C. Parasternal long-axis color Doppler image during diastole shows moderate aortic regurgitation and moderate degree of aortic stenosis (mean pressure gradient = 38 mm Hg, not shown). D, E. Short-axis cardiac computed tomography (CCT) images of aortic valve during diastole (D) and systole (E) show thickened and calcified quadricuspid aortic valve with two equal larger cusps and two unequal smaller cusps. Areas of right cusp, left cusp, noncoronary cusp, and accessory cusp (arrows) are 2.44, 3.03, 2.92, and 0.31 cm2, respectively. Lack of coaptation of aortic valve (regurgitant orifice area = 0.1 cm2) was detected during diastole (D). F. Oblique coronal CCT image shows measurement of ascending aorta diameter at four different levels during early systole (annulus, 27 mm; sinuses of Valsalva, 36.7 mm; sinotubular junction, 26.7 mm; tubular portion, 51 mm). Patient underwent combined aortic valvuloplasty and ascending aorta wrapping. LCC = left coronary cusp, NCC = noncoronary cusp, RCC = right coronary cusp, 4th = accessory cusp
|
CMR Studies
All cardiovascular magnetic resonance (CMR) studies were conducted with a 1.5T whole-body system (Signa Excited HD, GE Medical Systems, Milwaukee, WI, USA) using an eight-element phased array surface coil (Cardiac coil, GE Medical Systems). Cine images were acquired with a gradient echo FIESTA sequence (echo time, 1.54 ms; repetition time, 3.54 ms; flip angle, 45°; slice thickness, 5 mm without interslice gaps; field of view, 36 x 36 cm; matrix, 224 x 224; pixel size, 0.16 x 0.16 cm). The aortic valve imaging plane was defined by acquiring a three-chamber view and an oblique coronal view of the aortic valve and proximal aorta. Subsequent slices were defined parallel to the valvular plane. At least five slices (range, 5–7) of the aortic valve were acquired.
Aortic regurgitant volume and antegrade stroke volume were quantified by phase-contrast CMR (echo time, 4.4 ms; repetition time, 11.9 ms; flip angle, 20°; slice thickness, 10 mm; field of view, 40 x 30 cm; matrix, 256 x 128) during breath-hold to cover the entire cardiac cycle. Aortic velocity mapping slice position was just below the aortic valve annulus. The regurgitant fraction (RF) by phase-contrast CMR was calculated by: regurgitant volume/forward volume x 100%. AR was graded as mild (RF < 20%), moderate (20% ≤ RF < 40%), or severe (RF ≥ 40%) (18). CMR image quality was assessed similarly to CCT using a 4-point subjective ranking scale as follows: 1, poor; 2, fair; 3, good; 4, excellent.
TTE Studies
We referred to each patient's electronic medical records for echocardiographic results. The presence and severity of aortic stenosis (AS)/AR were recorded by cardiologists. Two-dimensional TTE was performed with a Vivid 7 device (GE Healthcare) and an Acuson Sequoia C512 apparatus (Siemens Medical Solutions) with a 2.5–3.5 MHz imaging transducer. AS/AR severity was determined as mild, moderate, or severe by including some or all of the parameters according to American College of Cardiology/American Heart Association guidelines (9).
Statistical Analysis
Continuous variables were expressed as means ± standard deviations. Categorical variables were expressed as frequencies or percentages. Spearman's correlation coefficient analysis was used to assess the correlations between aortic ROA by CCT, RF by CMR, and regurgitation severity by TTE. A p < 0.05 was considered significant. The statistical analysis was performed using MedCalc ver. 10.4.8 (MedCalc Software, Mariakerke, Belgium).
Go to :
RESULTS
Patient Population
Eleven patients (5 women and 6 men; mean age, 50.7 ± 15.1 years; range 19–71 years) were identified. Ten patients were diagnosed by both TTE and CCT and 1 patient was diagnosed by CCT alone. CCT was performed to assess coronary artery disease before elective heart valve surgery in 9 patients with aortic valvular heart disease and in 2 patients with chest pain. The QAV classification and functional status and the associated conditions were provided in Table 1. Nine patients with moderate to severe AR and New York Heart Association functional classification II–III symptoms underwent aortic valve surgery. Two of 9 patients underwent concomitant ascending aorta wrapping because the diameter of the aortic sinuses of Valsalva or ascending aorta was ≥ 4.5 cm. Two patients who had trivial to mild degrees of AR and did not undergo surgery came from the cardiology clinic and health check-up center, respectively. TTE, CCT, and CMR were performed within 1 month.
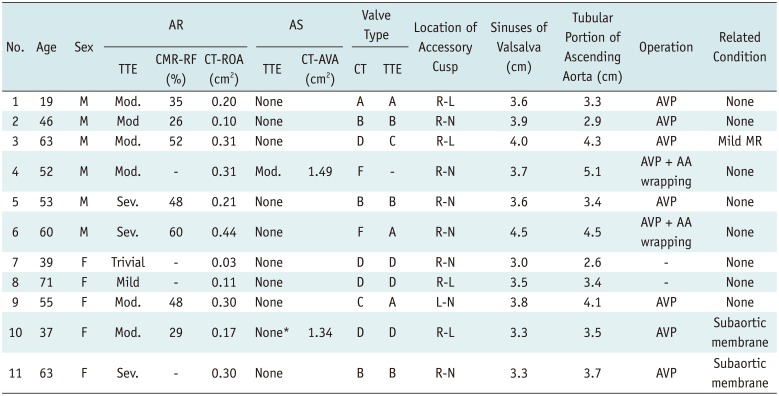
Table 1
Classification, Functional Status, and Associated Condition in 11 Patients with Quadricuspid Aortic Valve
*TTE reveals severe subaortic stenosis with subaortic membrane without AS at valve level. AA = ascending aorta, AR = aortic regurgitation, AS = aortic stenosis, AVA = aortic valve area, AVP = aortic valvuloplasty, CMR = cardiovascular magnetic resonance, CT = computed tomography, L-N = left-noncoronary cusps, Mod. = moderate, MR = mitral regurgitation, R-L = right-left coronary cusps, R-N = right-noncoronary cusps, RF = regurgitant fraction, ROA = regurgitant orifice area, Sev. = severe, TTE = transthoracic echocardiography
![]()
TTE
All of the patients had AR. Nine patients had pure AR (3 severe, 4 moderate, and 2 trivial to mild) and 2 patients had concomitant AR and AS (1 moderate AR and moderate valvular AS, 1 moderate AR and severe subvalvular AS due to a subaortic membrane). One QAV was misdiagnosed as a tricuspid aortic valve on TTE (Fig. 3). Table 1 showed the distribution of QAV types determined by TTE and CCT.
CCT
All patients were in stable sinus rhythm, and the mean HR during the CT scan was 62 ± 7 bpm. Mean radiation exposure including coronary calcium scan and CCT was 8.0 ± 1.6 mSv. CCT image quality was classified as grade 3 or 4, corresponding to diagnostic image quality. Three patients had valvular calcification; 2 patients (case 6 and 9) had pure AR and grade 2 valvular calcification (calcium volume score of 72 and 94) and 1 patient (case 4) had combined AS and AR and grade 3 valvular calcification (calcium volume score of 671). The median calcium volume score of aortic valve was 0 (interquartile range, 0–67). Both readers reached a consensus on the diagnosis of QAV in all 11 patients.
Using the Hurwitz and Robert's classification (2), type A was observed in 1 patient (Fig. 4), type B in 3 patients (Fig. 5), type C in 1 patient, type D in 4 patients, and type F in 2 patients (Fig. 3). Four patients had dilated aortic sinuses of Valsalva or > 4.0 cm diameter tubular portion of the ascending aorta. Nine patients were free of other cardiac anomalies but 2 patients had a subaortic membrane (Fig. 5). The location of the accessory cusp was between the RCC and LCC in 4 patients, between the RCC and noncoronary cusp (NCC) in 5 patients and between the LCC and NCC in 1 patient.
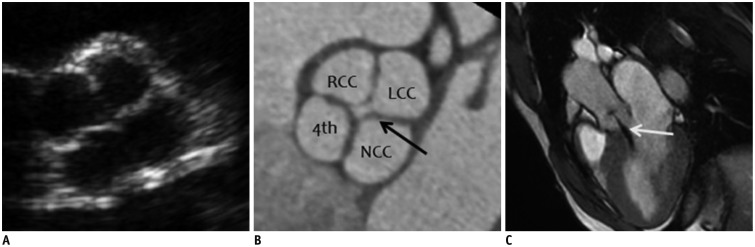 | Fig. 419-year-old man with Hurwitz and Robert's type A quadricuspid aortic valve (QAV) with four equal-sized cusps shown on transthoracic echocardiography (TTE), cardiac computed tomography (CCT), and cardiac magnetic resonance (CMR) imaging.
A. Parasternal short-axis TTE image of aortic valve during diastole shows QAV with four-leaf clover appearance. B. Short-axis CCT image of aortic valve during diastole demonstrates four equal aortic valve cusps. Areas of right cusp, left cusp, noncoronary cusp, and accessory cusp are 2.01, 2.13, 2.20, and 1.94 cm2, respectively. Lack of coaptation of aortic valve (arrow, regurgitant orifice area = 0.2 cm2) was detected during diastole, indicating aortic regurgitation. C. Oblique sagittal cine CMR image during diastole demonstrates central regurgitant jet (arrow) into left ventricular cavity. Quantitative analysis by phase-contrast CMR (not shown) yields regurgitant fraction of 35%, corresponding to moderate degree of aortic regurgitation (AR). LCC = left coronary cusp, NCC = noncoronary cusp, RCC = right coronary cusp, 4th = accessory cusp
|
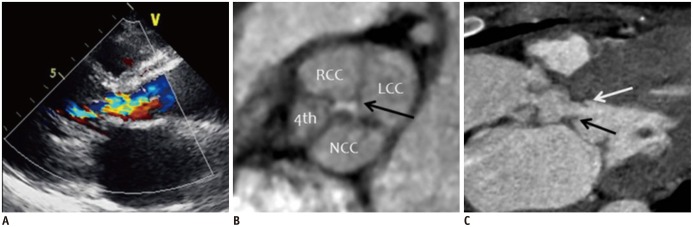 | Fig. 537-year-old woman with Hurwitz and Robert's type B quadricuspid aortic valve (QAV) combined with aortic regurgitation (AR) and subaortic stenosis due to subaortic membrane.
A. Parasternal long-axis color Doppler image during diastole shows moderate AR. B. Short-axis cardiac computed tomography (CCT) image of aortic valve during diastole demonstrates QAV with three equal-sized cusps and one smaller cusp. Areas of right cusp, left cusp, noncoronary cusp, and accessory cusp are 1.62, 2.13, 1.77, and 0.80 cm2, respectively. Lack of coaptation of aortic valve was detected (arrow, regurgitant orifice area = 0.17 cm2) during diastole. C. Oblique sagittal CCT image shows subaortic membrane (black and white arrows) with left ventricular outflow tract obstruction. Patient underwent aortic valvuloplasty and resection of subaortic membrane. LCC = left coronary cusp, NCC = noncoronary cusp, RCC = right coronary cusp, 4th = accessory cusp
|
CMR
Seven patients underwent CMR. All CMRs were of diagnostic image quality (good or excellent), and all CMRs detected QAVs. According to RF of CMR, 3 had moderate AR and 4 had severe AR.
Comparison of AR Severity among Modalities
An excellent correlation (r = 0.99, p = 0.015) existed between the CCT planimetric measurements of ROA (mean, 0.23 ± 0.12 cm2; range, 0.03–0.44 cm2) and RF determined by phase-contrast CMR (mean, 43 ± 13%; range, 26–60%). A good correlation was observed between ROA measured by CCT and regurgitant severity assessed by TTE (r = 0.62, p = 0.051).
Go to :
DISCUSSION
This is the first study to report multimodality imaging findings of 11 QAV cases. Our main findings were: 1) QAV had various morphological patterns and functional abnormalities, particularly AR; 2) dilatation or aneurysm of the ascending aorta (> 4.5 cm in diameter) was present in some patients with QAV; 3) CCT helped classify QAV based on planimetric measurements of the cusp area; 4) CCT may be used to quantitatively evaluate the severity of AR by measuring ROA.
In the present study, one QAV was misclassified as a tricuspid aortic valve on TTE because the accessory cusp was too small to be detected as a separate cusp. TTE is the typical standard diagnostic modality for assessing aortic valve morphology and function. However, echocardiography is an operator-dependent method and poor acoustic windows and suboptimal patient body habitus can compromise image quality, leading to an inaccurate diagnosis (1920). Furthermore, severe calcification can obscure acoustic windows and a very small cusp could be overlooked. Some reports indicate that intraoperative transesophageal echocardiography (TEE) discovered a QAV that was not identified by previous TTE (82122). In contrast, CCT allows for accurate visualization of cusp number, morphology, and motion, even in patients with severe valvular calcification or prosthetic valve (192324). Therefore, CCT could be helpful when the TTE evaluation is limited and could be used as an alternative to TEE.
Hurwitz and Roberts (2) classified QAV into seven types based on the relative size of the four cusps in autopsy cases. Type B was reported previously to be the most prevalent form of QAV (22025). However, a recent review analyzing 186 QAV cases showed that the most common type was A, which was present in 51 cases (3). In the present study, consensus on the QAV classification was reached between the CCT and TTE findings in 7 of 10 patients. This discrepancy was primarily caused by the small number of cases in our study and the different methods used to measure the areas of the four cusps. Even though there are several case reports of QAV with a planimetric evaluation of the four cusps using TTE (2122), no reports are available on QAV planimetric measurements using CCT.
A QAV frequently functions abnormally. Stenosis is unusual, and regurgitation is the most prevalent abnormality (2627). Although stenosis is a congenital anomaly, most cases appear to be competent in childhood. Sievers et al. (28) suggested that disproportionate cusp sizes may result in abnormal valve motion leading to fibrous thickening of the valve; thus, aggravating incomplete coaptation of the cusps. Most patients will require valve replacement in their 50s or 60s (18). In our study, all of the patients had AR, and 1 had concomitant valvular AS with moderate degree of valve calcification. A good correlation was detected between aortic ROA using CCT and RF using CMR and between ROA using CCT and regurgitant severity using TTE.
We found 2 cases of QAV with a subaortic membrane. One was diagnosed with QAV with a subaortic membrane before aortic valve surgery, which caused severe subvalvular AS, as determined by TTE, CCT, and CMR. The subaortic membrane in the other patient was discovered during surgery. QAV is often associated with other congenital heart defects (3). An additional malformation was found in approximately 18% of the cases reviewed, including anomalies of the coronary arteries, ventricular septal defects, patent ductus arteriosus, and subaortic fibromuscular stenosis (3). A QAV associated with an ascending aortic dilatation or aneurysm is extremely rare, but there are a few case reports (2930). In this study, all patients were free of a coronary arterial anomaly. However, 4 patients had a > 4.0 cm aortic root or ascending aorta diameter. In particular, 2 patients with > 4.5 cm diameter aortic sinus of Valsalva or ascending aorta underwent combined ascending aorta wrapping and aortic valvuloplasty.
The important reasons to classify QAV and the clinical significance of a QAV classification are as follows. Cho et al. (31) reported a correlation between valve function and valve type according to cusp size or the position of the accessory cusp. However, considering that the QAV classification is based on the operator's naked eye and not on a subjective measurement as in previous studies, there is a possibility of misclassification. In this study, 3 of 10 patients showed a discrepancy between CCT and TTE when assessing the QAV classification. Furthermore, there was an attempt to simplify the classification, which can be applied to clinical practice and patient management. Jagannath et al. (4) proposed a modified QAV classification scheme of 4 types considering clinical management. In this simplified classification, QAV types A, B, and C are types I, II, and III and QAV types D, E, F, and G are classified as type IV. They concluded that types II and III were prone to moderate to severe AR compared to that of the other two types; thus, this revised classification improves communication and clinical and surgical decision-making in patients with QAV. Surgical decision making is related to either: 1) severity of AR; 2) symptoms; 3) left ventricular dilation/dysfunction; or 4) associated aortopathy with aneurysm, etc. (32). CCT enables an accurate assessment of QAV morphology and may help cardiologists and surgeons create further management plans.
Based on the results of this study, CCT may provide useful information regarding the morphological and functional characteristics of the QAV, QAV-related cardiovascular abnormalities, and measurements of the ascending aorta. In the clinical setting, CCT can be used for comprehensive evaluation of coronary arteries, valvular morphology and function, and associated cardiovascular abnormalities in patients with aortic valvular heart disease before elective heart valve surgery.
This study had limitations. First, it was subject to the limitations inherent in a single-institution and retrospective analysis of observational data. Lower reliability of results occurs in a retrospective study when comparing techniques, particularly TTE. In addition, the number of cases was too small because QAV is a very rare disease. Accordingly, this small number might be insufficient for the statistical analysis of comparison of AR severity among modalities. Second, this study was not designed for a direct comparison of CMR. Therefore, CMR was not performed in 4 patients. Furthermore, cardiac surgeons only reported QAV without mention of classification of subtype. Therefore, we could not correlate CT findings of subtypes with those of intraoperative findings.
In conclusion, our results suggested that QAV has various morphological patterns and is associated with valvular dysfunction, particularly AR. In addition, dilatation or an aneurysm of the ascending aorta is common in patients with QAV. CCT is a useful imaging modality for comprehensively assessing QAV, including detection, classification, QAV-related cardiovascular abnormalities, AR severity, and dimensions of the ascending aorta.
Go to :
 XML Download
XML Download