

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
18F-fluorodeoxyglucose (FDG) positron emission tomography (PET) imaging for lesions in the brain often yields false-negative results, because the physiological uptake of 18F-FDG associated with high glucose metabolism in the brain can mask brain lesions. To overcome these difficulties, many PET tracers, including amino acid compounds that are hard to partition into the brain, have been developed. Among the various amino acid compounds for PET, 11C-methionine (Met) is one of the most commonly used PET tracers (1). Amino acids have special roles in the brain, which contributes to cerebral protein synthesis, intermediary metabolism, and interneuronal synaptic transmission. In addition, the essential amino acids, including Met, must be obtained from diets through intestinal absorption and released into the blood supply. Cerebrovascular endothelial cells express specific carriers that mediate the entry and efflux of amino acids across the luminal membranes of the blood-brain barrier (BBB) (2). The clinical use of 11C-Met PET for the imaging of brain tumors that has been reported is as follows: diagnostic accuracy, lesion extension or tumor grading assessment, biopsy or treatment planning, and prognosis or therapeutic response prediction (3). However, ideal methods for the assessment of 11C-Met PET images remain controversial, although many reports have described the use of visual assessment, tumor-to-normal (T/N) ratio, or the mean and/or maximum standardized uptake value (SUV) (3). Additionally, 11C-Met is not an ideal tracer because non-tumor lesions reportedly show increased uptake. It is important for nuclear medicine physicians/radiologists to be familiar with the imaging features and pitfalls of 11C-Met PET images. In this study, we describe the tips and pitfalls of 11C-Met PET imaging for intracranial lesions.
Physiological Uptake and Normal Variants
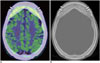
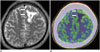
The pituitary gland, choroid plexus, and confluence of sinuses frequently appear in areas of physiological uptake. Lesions in these regions are occasionally overlooked or misinterpreted because these regions show relatively higher uptake than those in surrounding tissues. In particular, the pituitary uptake may depend on the hormonal status in female patients. Normal variants, such as hyperostosis or fibrous dysplasia, also show relatively high 11C-Met uptake, although the underlying mechanism remains unknown (Fig. 1). On the other hand, pineal cysts, choroid plexuses cysts, parahippocampal cysts, and Rathke's cleft cysts (Fig. 2) show no or low 11C-Met uptake. Magnetic resonance imaging (MRI) should precede 11C-Met PET to check the morphological anatomy of the central nervous system (CNS). The effect of aging on physiological uptake in the brain is limited, although SUV in the normal brains of children is slightly different from that in the normal brains of adults (4). Whether or not the patients should be in the fasting state before 11C-Met PET is also controversial. In patients with head and neck cancer, one study reported that food intake before 11C-Met PET can decrease the tumor SUV, although there is no robust evidence showing that the fasted state affects visual interpretation (5). In typical PET/computed tomography (CT), CT scans can be helpful for identifying lesions and detecting calcification. Additionally, PET/CT can be safely performed in patients with implanted electronic devices, patients for whom MRI is contraindicated, or patients who are allergic to contrast media.
Glioma
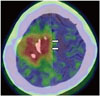
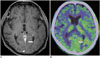
Typical high-grade glioma is easily diagnosed by MRI. However, edema or a destroyed BBB in the boundary zone of tumors frequently modifies MRI findings. 11C-Met PET, as information complementary to that of MRI, is helpful for the delineation of tumors and estimation of histopathological components or cellular activity. The overall sensitivity of 11C-Met PET for gliomas, including both high- or low-grade gliomas, is estimated to be approximately 76–100% in various studies (3). In addition, the studies of only low-grade gliomas reported a sensitivity ranging from 65–85% (2). For assessment of the histopathological grade of cerebral glioma, 11C-Met PET does not show clear predictive value through semi-quantitative or visual analyses to date, because of a significant degree of overlap among tumors of several grades (3). However, 11C-Met uptake is usually higher in high-grade gliomas than in low-grade gliomas (Fig. 3). As an exception, gliomatosis cerebri, a high-grade glioma, is occasionally difficult to detect using 11C-Met PET because of infiltrative invasion into the white matter (Fig. 4). Additionally, CT images during PET/CT examination may provide clues for diagnosis, e.g., calcification of oligodendroglioma and oligoastrocytoma (Fig. 5). The diagnosis of rare low-grade glioma is problematic because of its slow growth and the difficulties in histological confirmation. Few reports describe occasional high 11C-Met uptake of pilocytic astrocytoma or pleomorphic xanthoastrocytoma, which may be pitfalls in the diagnosis of these tumors (6). 11C-Met PET for evaluating ependymomas is reported mainly for spinal lesions, and the ependymomas could be detected to a certain degree except for some small lesions (7).
Assessment of Biopsy Planning
The assessment of biopsy sites using 11C-Met PET is compared with that using MRI because brain tumors are histologically heterogeneous with different cancer grades and necrosis. Biopsy planning depending only on MRI can lead to inaccurate diagnosis. Various studies suggest an advantage of 11C-Met PET for identifying the best target for biopsy or for estimation of the tumor volume.
Differentiation between Tumor Recurrence and Radiation Necrosis
Several studies show that 11C-Met PET has advantages for distinguishing radiation necrosis from focal recurrence after radiotherapy (3). The mechanism of 11C-Met uptake in radiation necrosis is different from that in recurrence. Radiation injury leads to passive diffusion across the broken BBB. Theoretically, uptake by recurrent tumors should exceed the uptake after radiation injury; however, the possibility of overlap between these uptakes exists. Actually, different T/N cutoff ratios (1.27–1.9) are also used for this indication. Previous studies report sensitivities ranging from 75–100% and specificities from 60–100% (3).
Other Brain Tumors
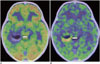
Apparently, 11C-Met PET is not useful for the diagnosis of brain metastasis in baseline surveys. Fine nodular metastases are difficult to detect using 11C-Met PET because of the resolution limits and lesion sizes. Primary CNS lymphoma (PCNSL) usually presents with various types of 18F-FDG uptakes and a wide range of appearances from massive lesions to faint abnormal signals on MRI. 11C-MET PET reportedly shows a higher sensitivity similar to that of 18F-FDG PET, for the detection of primary lesions in patients with PCNSL (8). However, some cases of PCNSL are more clearly detected using 11C-Met PET and contrast-enhanced MRI than using 18F-FDG PET (Fig. 6). In our experience, malignancies under an immunosuppressive state, such as in acquired immunodeficiency syndrome (AIDS) or post-chemotherapy, occasionally present low 11C-Met uptake of the tumor (Fig. 7). In patients with CNS germinoma, the tumor-contouring ability of 11C-Met PET for some malignant tumors is higher than that of 18F-FDG PET. Importantly, the visual appearance of CNS germinomas differs depending on their location. Suprasellar and pineal lesions are clearly shown to have higher uptakes than those of surrounding structures. On the other hand, lesions at the basal ganglia show higher asymmetrical uptakes (Fig. 8) (9). The 11C-Met uptake of several rare low-grade brain tumors has a confusing appearance similar to the images of high-grade gliomas. Therefore, morphological imaging, such as MRI, is required. Biological factors that affect 11C-Met uptake in these benign tumors that can provide fundamental information for interpreting 11C-Met PET are not fully examined. Mixed neuronal and glial tumors, such as gangliogliomas and dysembryoplastic neuroepithelial tumors (DNTs), are common brain tumors accompanied by epileptogenic foci. Previous studies show that gangliogliomas (Fig. 9), including gangliocytoma of Lhermitte-Duclos disease, show higher 11C-Met uptake than DNTs (Fig. 10), although their uptakes slightly overlap (10). Meningiomas, which are the most common primary brain tumors, also show high 11C-Met uptake. 11C-Met PET can be used to evaluate recurrent or residual meningiomas post-resection. However, according to a previous study, 11C-Met uptake of meningiomas is correlated with tumor volume and location, e.g., skull-base tumors have higher uptakes than tumors at other locations but are not correlated with tumor aggressiveness, such as MIB-1 index, tumor-doubling time, or tumor grade (11). Central neurocytoma, which is a representative benign tumor, is described as having a markedly higher 11C-Met uptake (Fig. 11) (12). 11C-Met PET in patients with pituitary adenoma, particularly in hormone-secreting adenomas, is used to detect recurrent lesions. Craniopharyngioma also is also reported to show mild 11C-Met uptake. Although the evidence of 11C-Met uptake for benign tumors is limited, it should be obtained to enable efficient management.
Vascular Diseases
11C-Met PET imaging for vascular lesions in the brain often yields false-negative results. Increased 11C-Met uptake in the perivascular mononuclear infiltrate and gliotic reaction in the collagen capsule surrounding hematomas (Fig. 12), BBB breakdown of infarction, and plugged venous flow of malformation (Fig. 13) are potential mechanisms for positive 11C-Met findings (1314). To prevent misdiagnosis and unnecessary surgical intervention, MRI or CT should precede any PET examinations for evaluating cranial lesions.
Inflammation and Infection
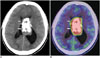
Several reports speculate that the mechanism of 11C-Met uptake in inflammation involves increased metabolism and active amino acid transport as a result of the increased density of inflammatory cells, as well as disruption of BBB. Tumefactive demyelination is a representative disease that shows various uptake patterns depending on the disease activity. In addition, 11C-Met uptake patterns may not necessarily correspond to the enhanced patterns of the lesions (Fig. 14). Encephalitis exhibits various uptake patterns and degrees even in the same pathogens. 11C-Met uptake in encephalitis is relatively dependent on the disease activity, although the mechanisms of increased 11C-Met uptake remain unknown. Sarcoidosis, brain abscess, progressive multifocal leukoencephalopathy, and tuberculoma are also reported as causes of false positives in 11C-Met PET (15). In patients with AIDS, 11C-Met uptake may help distinguish lymphoma from toxoplasmosis. However, several cases of toxoplasmosis show high uptake similar to that of tumors (Fig. 15) (15). Current evidence cannot support the usefulness of 11C-Met PET for inflammation diseases.
Dysplasia and Hamartoma
Focal cortical dysplasia (FCD) or cortical tubers are representative dysplasias having epileptogenic foci. In general, MRI and 18F-FDG PET usually precede 11C-Met PET to detect epileptogenic focus. 11C-Met uptake of FCD is similar to the uptake of other gray matter, a finding that can be helpful for distinguishing FCD from ganglioglioma prior to surgery (10). However, we occasionally encounter FCD lesions with slightly higher uptake than that of the surrounding cortex (Fig. 16) (16). Modification of amino acid transporters, such as by gliotic reaction or hyperperfusion, is a proposed mechanism for positive 11C-Met uptake in FCD, although a concrete evidence of the mechanism remains unclear. Hamartoma, which is a benign neoplastic heterotrophic lesion, shows uptake similar to that of white matter, a finding that may contribute to accurate diagnosis (Fig. 17).
CONCLUSIONS
Intracranial lesions show a wide spectrum of 11C-Met PET/CT imaging features. Interpretation of 11C-Met PET images requires a high degree of suspicion for the presence of brain tumors. Familiarity with the characteristics and pitfalls of 11C-Met PET/CT imaging will contribute to better interpretation of findings by radiologists.











 XML Download
XML Download