

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Sclerosing cholangitis includes a spectrum of chronic, variably progressive cholestatic liver disease characterized by inflammation, fibrosis, and stricture of the intrahepatic 38and extrahepatic bile ducts (1). Sclerosing cholangitis can be divided into primary sclerosing cholangitis (PSC) of unidentified etiology and secondary sclerosing cholangitis caused by various identifiable etiologies, including immunoglobulin G4-related sclerosing cholangitis (IgG4-SC), recurrent pyogenic cholangitis (RPC), ischemic cholangitis, acquired immunodeficiency syndrome (AIDS)-related cholangitis, and eosinophilic cholangitis. The diagnosis of PSC requires the exclusion of secondary causes of sclerosing cholangitis. Furthermore, contrary to PSC in which liver transplantation is recommended as a curative treatment option, secondary sclerosing cholangitis can respond favorably to treatment for related causes. Therefore, awareness of the imaging features of primary and secondary sclerosing cholangitis and the clinical setting are important for accurate diagnosis in patients with sclerosing cholangitis.
In this article, we describe the imaging findings of the various spectrums of sclerosing cholangitis with an emphasis on a systemic approach in differential diagnosis. We also discuss the clinical significance of and therapeutic options for treating sclerosing cholangitis.
Primary Sclerosing Cholangitis
Primary sclerosing cholangitis is a chronic, progressive liver disease with inflammation and fibrosis of the bile ducts of unidentified etiology, which finally progresses to biliary cirrhosis and portal hypertension (23).
The prevalence of PSC is approximately 10/100000 in Northern Europe (45) and the USA, while it is far less common in Southern Europe and Asia (67). PSC affects men twice as often as women, and generally young patients with an age of onset of 30-40 years. PSC has a strong association with inflammatory bowel diseases. Approximately 60 to 80% of patients with PSC present with inflammatory bowel disease of which, 87% have ulcerative colitis and 13% have Crohn's disease (89). The clinical presentation can vary, including cholestatic laboratory findings and nonspecific symptoms including right upper quadrant pain or jaundice.
Although the pathogenesis remains to be elucidated, many experts accept an autoimmune component (101112). A typical histopathologic feature of PSC is substantial periductal ("onion-skin") fibrosis with minimal inflammatory cells (Fig. 1). However, this finding is observed in < 20% of cases and may also be found in secondary sclerosing cholangitis (13). Therefore, a liver biopsy is not recommended for the diagnosis of PSC in patients with typical cholangiographic findings (14).
Diagnosis of PSC can be made by typical cholangiographic findings and the exclusion of secondary causes. Both the American Association for the Study of Liver Diseases and the European Association of the Study of the Liver guidelines recommend magnetic resonance (MR) cholangiography as the first option for cholangiography in cases of suspected PSC, and endoscopic cholangiography for non-diagnostic cases (1415). The typical MR cholangiographic features include diffuse, multifocal short segmental strictures and mild dilatation in the intrahepatic and extrahepatic bile ducts alternating with normal ducts, which sometimes produce "beaded" appearance (Figs. 2, 3). As the fibrosis progresses and strictures worsen, the peripheral bile ducts are obliterated and become poorly visualized on MR cholangiography showing a "pruned tree" appearance (Fig. 3) (16). Diverticular outpouching of bile ducts is another characteristic finding that occurs in up to 27% of the patients with PSC (Fig. 2) (17). Almost half of patients with PSC have some degree of mural irregularity causing a shaggy or nodular appearance of the bile ducts (18). PSC commonly involves both intrahepatic and extrahepatic ducts in 75% of patients, whereas involvement of only the extrahepatic bile duct is uncommon (10% of patients) and isolated involvement of the intrahepatic bile ducts is reported in 15% of patients (3). Bile duct stones are detected in 8% of these patients (16).
Abdominal ultrasonography (US) is generally non-diagnostic, although thickened or focal dilated bile ducts are observed in PSC patients. Computed tomography (CT) demonstrates alternating narrowing and dilatation of the bile ducts with contrast enhancement in PSC (19). CT and MR imaging also show associated parenchymal changes of the liver, as well as ductal changes in PSC. A rounded liver appearance is observed due to hypertrophy of the caudate lobe and atrophy of the left lateral and right posterior segments in PSC (9). In PSC, T2-weighted MR images show a wedge-shaped or reticular heterogeneous area of high-signal intensity with peripheral distribution (20).
Patients with PSC have a 10 to 15% risk of developing cholangiocarcinomas, and a 7 to 9% chance of a 10-year cumulative incidence of cholangiocarcinomas (1621). Diagnostic evaluation of suspected cholangiocarcinoma includes serum cancer antigen 19-9, imaging studies such as MR, CT and endoscopic cholangiography with brushing or cytology (14). Of the imaging findings, malignant appearing mass compatible with cholangiocarcinoma is the most direct finding, although masses are uncommon in the early stage of cholangiocarcinoma. Progressive ductal dilatation seen in follow-up studies, marked ductal dilatation, severe ductal narrowing, mural thickening, and intraductal polypoid lesions in PSC are also highly suggestive of cholangiocarcinoma (916).
Medical therapy such as the use of ursodeoxycholic acid, corticosteroids or other immunosuppressive agents have shown only limited success in patients with PSC (22). In patients with advanced liver disease, liver transplantation is recommended as a curative treatment option (14). Recurrence of PSC after liver transplantation occurs in 20 to 25% of patients 5 to 10 years after the liver transplantation (23).
Secondary Sclerosing Cholangitis
IgG4-Related Sclerosing Cholangitis
Immunoglobulin G4-SC is bile duct involvement of IgG4-related systemic disease (IgG4-RD) (24). After the pancreas, bile ducts are the second most common organ, involved with IgG4-RD. Patients with IgG4-SC are predominantly males in their 60s (mean age, 63 years) (25). Patients with IgG4-SC commonly present with obstructive jaundice. Like other IgG4-related diseases, the serum IgG4 is frequently elevated.
Immunoglobulin G4-SC shares the immunohistopathologic features of other IgG4-RD, including autoimmune pancreatitis, which is characterized by lymphoplasmacytic infiltration with abundant IgG4-positive plasma cells, storiform interstitial fibrosis, and obliterative phlebitis (Fig. 4) (26).
Abdominal US has limited value for diagnosing IgG4-SC, although it may show thickening of the bile duct and gallbladder. In cases of IgG4-SC, cross-sectional imaging, such as CT or MR imaging, demonstrates long-segmental, symmetrical, circumferential wall thickening and delayed contrast enhancement of the involved bile ducts (Fig. 5) (27). In approximately half of these patients, the involved bile duct lumens are narrowed, although visible (28). The most commonly involved location is the intrapancreatic segment of the common bile duct (CBD) followed by the hilar bile ducts in IgG4-SC (Fig. 5) (29). Multifocal involvement of both intrahepatic and extrahepatic bile ducts can occur, similar to PSC, while isolated stricture of the distal CBD can also be observed in IgG4-SC. The cholangiographic findings of IgG4-SC include long and continuous stricture of the bile ducts with prestenotic dilatation (Fig. 5) (30). Lymphadenopathy is not uncommon in patients with IgG4-SC (24). In particular, extrabiliary findings associated with IgG4-RD involvement, including the pancreas, kidney or retroperitoneal fibrosis, strongly suggest IgG4-SC (27).
Differentiation of IgG4-SC from other types of sclerosing cholangitis, especially from PSC, is clinically important as IgG4-SC shows a dramatic response to steroid therapy (Table 1) (31). Patients with PSC are generally younger and less symptomatic than those with IgG4-related disease. Multifocal intrahepatic duct involvement with short segmental strictures as well as a beaded, pruned-tree, and diverticulum-like appearance are imaging features suggestive of PSC. As IgG4-SC sometimes presents with prominent wall thickening in the bile duct, cholangiocarcinoma can be included as a differential diagnosis. Imaging features more suggestive of cholangiocarcinoma than of IgG4-SC include solitary lesion with irregular margins, eccentric wall thickening, invisible bile duct lumen in the involved segment, more prominent wall thickening (> 3 mm) and contrast enhancement, and an abrupt transition between the normal and involved bile duct (32). In patients with an inconclusive diagnosis, a steroid trial could be considered for the diagnosis of IgG4-SC in selected patients (33).
Recurrent Pyogenic Cholangitis
Recurrent pyogenic cholangitis is a progressive biliary disease characterized by recurrent episodes of cholangitis and intrahepatic pigmented stones (34). RPC is prevalent in Asian countries (35) and equally affects patients of both sexes (3637). Patients with RPC are commonly in the sixth and seventh decades of life and of rural and low socioeconomic status (3637). These patients typically present with abdominal pain, fever, and jaundice (the Charcot triad) and often have a history of recurrent episodes. The laboratory tests in RPC may demonstrate leukocytosis and elevated serum bilirubin.
Although the exact pathogenesis of RPC is unknown, strong associations with parasitic infestation such as Clonorchis sinensis or Ascaris lumbriocoides, portal bacteremia, and malnutrition are suggested (3638). Chronic recurrent infection of the bile ducts is thought to induce biliary stricture, bile stasis, and pigmented biliary stones. Approximately 30 to 80% of the stones in RPC are calcium bilirubinate stones commonly found in the intrahepatic bile duct (39). Histologically, bile ducts and periductal tissue show fibrous mural thickening, as well as acute and chronic inflammatory changes in RPC (38). The hepatic segments containing stones demonstrate parenchymal atrophy and scarring (38).
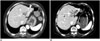
The diagnosis of RPC is based on the demographic background, as well as the clinical and imaging features. Abdominal US in RPC shows bile duct dilatation with increased periportal echogenicity. The intrahepatic bile duct stones can show various degrees of echogenicity and posterior shadowing (40). CT in RPC demonstrates disproportional dilatation of central intrahepatic ducts and extrahepatic bile ducts with nondilated or minimally dilated peripheral ducts, leading to decreased arborization and abrupt tapering of bile ducts (Fig. 6). Up to 90% of hepatolithiasis show hyperattenuation on unenhanced CT images, as compared to normal liver parenchyma (Fig. 6) (3641). Parenchymal atrophy occurs most frequently in the left lateral segment and the right posterior segment, while hypertrophy occurs in the caudate lobe and left medial segment, thus producing a round liver appearance in RPC. Heterogeneous parenchymal enhancement and periductal enhancement are often seen during acute exacerbations (42). For evaluation of patients with RPC, MR cholangiography is preferred to endoscopic cholangiography, since it can evaluate the bile ducts proximal to an obstruction and has no risk for biliary sepsis (40). However, endoscopic cholangiography has advantages for allowing therapeutic intervention. Cholangiography in RPC demonstrates dilatation of the central bile ducts and rapid tapering in the peripheral bile ducts, known as the arrowhead appearance (Fig. 6) (43). Strictures usually occur in the intrahepatic bile ducts (43). MR is more sensitive than CT for detecting radiolucent stones, which can appear hypointense on T2-weighted images and isointense to hyperintense on T1-weighted images (44). On the other hand, pneumobilia, which is commonly seen in RPC, can often mimic intrahepatic stones on MR or US, while it is more easily diagnosed with CT. In cases of Clonorchis sinensis infestation, cholangiography shows diffuse uniform dilatation of the peripheral intrahepatic bile ducts without a focal obstructive lesion. Flukes are occasionally visualized in the dilated bile ducts as filling defects (Fig. 7) (45).
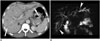
The complications of RPC include biloma, hepatic abscess, inflammatory pseudotumor, thrombophlebitis of portal or hepatic veins, and cholangiocarcinoma (38). Hepatic abscesses can develop in up to 20% of these patients (43). The most threatening complication is cholangiocarcinoma, which is detected in 2 to 6% of patients with RPC (46). Cholangiocarcinoma most commonly occurs in atrophic hepatic segments or segments harboring many stones (Fig. 8) (35). Recurrent bacterial infection, bile stasis, and chronic irritation by stones are suggested as carcinogenic factors (47). Accurate diagnosis of cholangiocarcinoma in patients with RPC can be more difficult than in the general population, because biliary and parenchymal changes in underlying RPC can hinder the early detection of cholangiocarcinoma.
Recurrent pyogenic cholangitis sometimes mimics the imaging findings of PSC, which can also be accompanied by multifocal biliary strictures and hepatolithiasis. However, the involvement of both intrahepatic and extrahepatic bile ducts, a beaded appearance, and biliary diverticulum suggest PSC rather than RPC (Table 1) (38). Intraductal papillary neoplasm of the bile ducts can sometimes resemble RPC, as both present as nodular lesions in a dilated bile duct. The presence of contrast enhancement is suggestive of intraductal papillary neoplasm (38).
The treatment goals in RPC are complete removal of bile duct stone and bile stasis for the prevention of acute episodes of cholangitis and further stone formation (48). Therapeutic options include antibiotics for acute cholangitis, endoscopic procedures such as stricture dilatation or stone removal, biliary drainage, and surgical procedures such as biliary bypass, segmental hepatic resection or liver transplantation (40). A multidisciplinary approach is useful for proper management in patients with RPC. When a malignancy is suspected, biopsy or fine needle aspiration should be considered.
Ischemic Cholangitis
Ischemic cholangitis is defined as ischemia-induced bile duct injuries due to various causes. The bile ducts are vulnerable to ischemic injuries as the blood supply to the bile ducts depends completely on the arterial supply in contrast to the hepatic parenchyma, which has a dual blood supply from the hepatic artery and the portal vein (49). Among the various conditions that compromise the arterial supply and can cause ischemic cholangitis, iatrogenic causes including liver transplantation, hepatic arterial infusion of chemotherapeutic agents, and vessel injury during biliary or pancreatic surgery constitute the most common etiology (15051). Ischemic cholangitis can exist in patients with hereditary hemorrhagic telangiectasia or polyarteritis nodosa (151).
Pathological features of ischemic cholangitis vary depending on the degree and extent of hepatic arterial insufficiency and the stages of ischemic cholangitis (51). In the acute stage of ischemic cholangitis, desquamated ischemic biliary epithelium with other bile components forms biliary casts. Dilatation of the bile ducts is commonly seen at this stage, probably due to obstruction by the casts and a reaction to ischemic injury (51). When ischemic insult is more severe, necrosis involving the full thickness of the bile ducts occurs and spilled bile in the hepatic parenchyma creates biloma (51). As the disease progresses, focal or diffuse fibrous strictures may develop at a later stage of ischemic cholangitis (51).
Diagnosis can be made according to the imaging features compatible with ischemic injury and evidence of a compromised arterial supply (51). The clinical and imaging features are closely related to the stage of the ischemic cholangitis. At the acute stage of ischemic cholangitis, the patients usually present with fever, abdominal pain, jaundice, and biliary sepsis. At this stage, the radiologic findings of biliary casts include intraductal filling defects in the dilated bile duct showing high signal intensity on nonenhanced T1-weighed MR images (Fig. 9) (52). At the acute stage of ischemic cholangitis, biliary casts appear similar to intraductal stones. However, they usually differ in their shapes, as biliary casts appear linear or have a branching pattern, whereas stones are usually oval or round (52). In severe ischemic injury, bile duct necrosis presents as tubular low density or intensity structures along the portal tracts on enhanced CT or MR images (Fig. 10) (51). Cholangiography in ischemic cholangitis shows dilated bile ducts with irregular margins and intraluminal filling defects (51). Bilomas can appear as an intrahepatic fluid collection usually located in the vicinity of the injured bile ducts (Figs. 9, 10) (53). At the chronic stage of ischemic cholangitis, the clinical symptoms and laboratory profile include progressive or fluctuating cholestasis. As the disease progresses, focal or diffuse strictures may develop at a later stage. Cholangiographic findings of ischemic cholangitis at this stage include multifocal biliary strictures and dilatation, both of which can mimic the findings of PSC (Fig. 10) (51). The clinical context and predominant location of ischemic strictures, i.e., the middle third of the CBD and the hilar bile duct, are suggestive of ischemic cholangitis rather than PSC (51).
Appropriate treatment option in ischemic cholangitis should be based on the individual patient's clinical setting. In the transplanted patients with large artery occlusion, restoration of arterial flow can be attempted using thrombolytic agents, balloon angioplasty or stenting and surgical revision. On the other hand, in patients with small artery ischemic injuries, management of complications caused by bile duct injury may be more important as there is no specific curative method. Endoscopic procedures allow removal of biliary casts, and percutaneous drainage is useful for biloma drainage and decompressing dilated bile ducts in ischemic cholangitis. Biliary bypass surgery can be performed for bile duct reconstruction in ischemic cholangitis (51).
AIDS-Related Cholangitis
Acquired immunodeficiency syndrome-related cholangitis is a form of secondary sclerosing cholangitis occurring in patients with human immunodeficiency virus (HIV) infection. AIDS-related cholangitis typically affects advanced HIV-infected patients with markedly decreased immune function (CD4 count < 100/mm3) (5455). The suggested mechanisms of AIDS-related cholangitis include randomly occurring infections involving the bile ducts, ischemia, autonomic nerve injury, and direct invasion of bile duct epithelium by the HIV itself (5657). The most common pathogens in AIDS-related cholangitis are cytomegalovirus, Cryptosporidium parvum, Mycobacterium avium complex, and herpes simplex virus, although no definite pathogen is identified in almost 50% of these patients (34). The typical clinical manifestations in AIDS-related cholangitis include right upper abdominal pain, as well as elevated alkaline phosphatase and transaminase levels. Associated papillary stenosis may result in more intense abdominal pain (58).
On CT and MR imaging, enhanced wall thickening of the extrahepatic bile duct and the intrahepatic bile ducts can be seen in AIDS-related cholangitis (Fig. 11) (5960). Cholangiographic findings in AIDS-related cholangitis include multifocal strictures and dilatation of intrahepatic and extrahepatic bile ducts resembling those seen in patients with PSC (Fig. 11) (3459). In AIDS-related cholangitis, endoscopic cholangiography features of papillary stricture include tapered narrowing in the terminal portion of dilated CBD and marked and delayed contrast retention (Fig. 11) (5961). The patient's clinical history, as well as some imaging features including papillary stenosis and a long extrahepatic bile duct stricture, can also help to differentiate AIDS-related cholangitis from PSC (5859).
Although antimicrobial therapy could be used for opportunistic infections in AIDS-related cholangitis, it is reported to be mostly ineffective (62). Sphincterotomy is the primary therapy for patients with papillary stenosis (58). For biliary stricture in AIDS-related cholangitis, endoscopic balloon dilatation and stent placement may be performed (63).
Eosinophilic Cholangitis
Eosinophilic cholangitis is defined as eosinophilic infiltration of the biliary system. Although there have been anecdotal case series in the English literature (646566), patients with eosinophilic cholangitis generally present with jaundice, which is often associated with eosinophilic gastroenteritis (64). Peripheral eosinophilia is the most helpful laboratory finding, even though it is reported in only approximately half of the patients with eosinophilic cholangitis (64). Histopathologically, eosinophilic cholangitis is characterized by dense transmural eosinophilic infiltration associated with other inflammatory cell infiltration in the bile ducts (65). A thickened fibromuscular layer and slight fibrosis in the subserosal layer are also present with eosinophilic cholangitis (65).
Imaging findings in eosinophilic cholangitis mentioned in previous reports include: wall thickening of the CBD, cystic duct, and gallbladder; diffuse bile duct stricture from the hepatic hilum to the intrahepatic duct; focal stricture of the common hepatic duct at the cystic duct insertion level; and mild smooth narrowing of the proximal common duct (Fig. 12) (116646567). Although a preoperative diagnosis of eosinophilic cholangitis is challenging due to its nonspecific imaging features, it should be considered when bile duct wall thickening is present with involvement of the cystic duct, the gallbladder, and peripheral eosinophilia. Patients with eosinophilic cholangitis show a favorable response to corticosteroids and often show a self-limited disease course without treatment (16666869).
Systemic Approach for Sclerosing Cholangitis
Before arriving at the differential diagnosis of sclerosing cholangitis, it is critical to exclude malignant bile duct strictures, especially when a single segmental bile duct wall thickening and/or stricture is detected. The following image features favor malignant biliary strictures rather than sclerosing cholangitis: a narrowed segment with hyperenhancement relative to the liver seen during the portal-venous phase; long length involved (> 12 mm); prominent bile duct thickening (> 3 mm); an indistinct outer margin; luminal irregularity; and asymmetry (70). After excluding malignant biliary strictures, the next step is to distinguish between PSC and secondary sclerosing cholangitis. Figure 13 summarizes the characteristic imaging features of sclerosing cholangitis according to the underlying etiologies. It is often challenging to differentiate the underlying etiologies of sclerosing cholangitis based solely on the morphological features. Therefore, the demographics, laboratory profiles, and patient's past medical history should be considered together with the imaging features. A systematic approach (Fig. 14) combined with the appropriate clinical settings and imaging findings, can be helpful for differentiating the various causes of sclerosing cholangitis. Pathologic confirmation, such as biopsy, is necessary in patients with an inconclusive diagnosis. In cases suspected of IgG4-SC, steroid therapy can be attempted for diagnostic and therapeutic purposes in a selected patient group.
CONCLUSIONS
There is a wide spectrum of causes of sclerosing cholangitis, including PSC and secondary sclerosing cholangitis caused by various conditions including IgG4-SC, RPC, ischemic cholangitis, AIDS-related cholangitis, and eosinophilic cholangitis. Several characteristic imaging features are suggestive of the underlying causes of sclerosing cholangitis, however, these imaging features substantially overlap. A systematic approach combined with appropriate clinical settings and imaging findings, may help to differentiate various causes of sclerosing cholangitis and ultimately to guide the appropriate patient management.













 XML Download
XML Download