

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Fluid-attenuated inversion recovery (FLAIR) is a special inversion recovery pulse sequence with a long repetition time (TR) and echo time (TE), and an inversion time (TI) that effectively nulls signals from the cerebrospinal fluid (CSF) (123). Although FLAIR images are heavily T2-weighted images (T2WI), contrast enhancement on FLAIR imaging is the result of a mild T1 effect that is produced by the long TI; thus, lesions that show enhancement on contrast-enhanced T1-weighted imaging (CE-T1WI) also show enhancement on contrast-enhanced FLAIR (CE-FLAIR) images.
Many clinical studies have shown that CE-FLAIR offers more information than CE-T1WI alone. This article describes the diagnostic importance of CE-FLAIR imaging for various intracranial pathologic conditions, as well as normally enhancing structures on CE-FLAIR imaging. Additionally, some distinctive conditions detected following gadolinium (Gd) administration such as the hyperintense acute reperfusion marker (HARM) and Gd encephalopathy related to renal failure will be discussed.
Underlying Mechanism of Gadolinium Enhancement
Intravenous magnetic resonance (MR) contrast agents are frequently used to improve lesion detection and characterization of central nervous system (CNS) disorders. The commonly used contrast agent, Gd, shortens both the T1 and T2 relaxation times of tissues in which it has accumulated. However, lesion contrast enhancement is caused predominantly by the T1-shortening effect at clinical doses (4567). Contrast enhancement in the CNS is the result of a combination of 3 processes: for intra-axial brain lesions, the blood brain barrier (BBB) must be disrupted for Gd to enter the extracellular space; for extra-axial lesions, enhancement is observed in lesions with relatively high vascularity; and for leptomeningeal regions, contrast leakage occurs from vessels into the CSF (891011). Although T1WI is typically used for post contrast examinations, CE-FLAIR is increasingly used currently.
The differences in enhancement characteristics between CE-T1WI and CE-FLAIR images have been shown in previous studies, and can be explained by a combination of a different T1-shortening effect at a certain concentration of Gd and a different T2 effect according to the vascularity of a lesion (5101213). Although Gd concentration alone cannot explain all the phenomena of intracranial enhancement in vivo, our phantom study (Fig. 1) showed that, the FLAIR sequence was more sensitive to T1 shortening than T1WI at lower concentrations of Gd, while the FLAIR sequence was sensitive to T2 effects at high Gd concentrations. This indicates that faintly enhancing lesions on CE-T1WI might be depicted more clearly on CE-FLAIR images, but marked enhancing lesions with large Gd accumulation show no enhancement on FLAIR images because the signal-reducing T2 effects obscure the signal-enhancing T1 effects. In addition, unlike CE-T1WI, CE-FLAIR images do not show contrast enhancement in normal vascular structures and normal meninges (4514). Therefore, CE-FLAIR images are highly effective in the detection of sulcal or meningeal infection, inflammation and metastases that abut the border of the CSF. However, in CE-FLAIR imaging alone, the observed hyperintensity lesion may be due to either T2 lengthening or T1 shortening, thus limiting the usefulness of the FLAIR sequence. Therefore, the FLAIR sequence should be performed with both pre- and post-contrast scans (456).
Contrast Enhanced MRI Protocol
In our study, contrast agent (gadobutrol [Gadovist]; Bayer Healthcare, Berlin, Germany) was administered at the standard dose of 0.1 mmol/kg of body weight. Postcontrast images were obtained shortly after contrast material administration. For each patient, the MR imaging was performed using 1.5T scanner (Avanto; Siemens Medical Solution, Erlangen, Germany) or 3T scanner (Skyra; Siemens Medical Solution, Erlangen, Germany). The MR imaging parameters for the FLAIR images were 4780-9000/93-124/1745-2497 ms/150°/320-384 × 196-235 (TR/TE/TI/flip angle/matrix). The other parameters were as follows: section thickness of 5 mm with a 2 mm gap, field of view of 193 × 220 mm, number of excitations of 2; and the acquisition time was 2 minutes 33 seconds and 2 minutes 42 seconds, respectively. Axial CE-FLAIR imaging in all patients was performed immediately after the routine CE-coronal and axial T1WI. Scanning of axial CE-T1WI and axial CE-FLAIR imaging was started at 2 minutes 40 seconds, and 5 minutes after the injection of contrast material, respectively. Although previous studies suggested some benefits of delayed CE imaging (151617), we did not acquire additional delayed FLAIR images.
Normal Enhancement on CE-FLAIR Imaging
Understanding the normally enhancing structures on CE-FLAIR imaging can provide a reference point for routine interpretation (18). However, literature on the evaluation of the normal pattern of enhancement on CE-FLAIR imaging in the adult brain is rare.
According to our experience and previous reports in children, the choroid plexus, pituitary infundibulum and cavernous sinus show relatively intense enhancement, and the pituitary gland, pineal gland and nasal mucosa/turbinates are mildly enhanced (Fig. 2). However, unlike CE-T1WI, FLAIR enhancement in the pineal gland, pituitary gland and nasal mucosa/turbinates can be difficult to recognize, or show subtle changes due to intrinsic T2 prolongation on pre-contrast FLAIR images. On CE-FLAIR imaging, most blood vessels do not show enhancement, probably due to a T2 effect of the FLAIR sequence. Additionally, the degree of enhancement in normal intracranial structures on CE-FLAIR imaging appears less intense than that on CE-T1WI, probably because of a mild T1 effect of FLAIR imaging.
Parenchymal Lesions
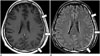
Contrast-enhanced-FLAIR imaging has several advantages for the detection of superficial parenchymal lesions and brain metastasis. Suppression of the CSF signal, no or minimal enhancement of blood vessels, reduction of phase-shift artifacts derived from enhanced blood vessels or dural sinuses, and better detection of peritumoral edema make lesions more conspicuous, and these features can be exploited in the detection of superficial lesions and metastatic tumors over CE-T1WI (519202122).
However, the potential pitfall of CE-FLAIR imaging in enhancing parenchymal tumors includes the difficulty to differentiate lesion enhancement versus hyperintense lesions with long T2 relaxation times. On CE-T1WI, it is easier to detect enhancing lesions surrounded by a hypointense edematous area. In addition, large Gd accumulated lesion may not demonstrate enhancement on CE-FLAIR images because the signal-reducing T2 effects obscure the signal-enhancing T1 effects. Hence, for intraparenchymal tumors, CE-T1WI can be superior to CE-FLAIR imaging for detecting the breakdown of the BBB (Fig. 3) (561220232425).
Leptomeningeal Lesions
Infection
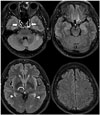
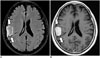
Infectious meningitis is the most common form of CNS infection. Although the diagnosis of infectious meningitis is still based on CSF examination, imaging studies such as magnetic resonance imaging (MRI) have been used increasingly not only for imaging diagnosis but also for monitoring the associated complications. CE-FLAIR imaging is more effective than CE-T1WI because it does not demonstrate enhancement in the normal vascular structures or normal meninges that can be confused with abnormal meningeal enhancement on CE-T1WI. Additionally, CE-FLAIR is more sensitive to lower Gd concentrations due to its extreme sensitivity to minimal modification of the CSF composition (Fig. 4) (51018262728293031).
Neoplastic Spread into the Subarachnoid Space (Primary and Metastatic Tumors)
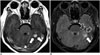
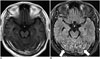
Likewise, the most specific diagnostic test for leptomeningeal carcinomatosis has been cytologic examination of CSF. However, this test often produces false-negative results. MRI, particularly CE-T1WI, has been used as a reliable technique for confirming diagnoses and assessing the extent of a lesion and its response to therapy. However, CE-FLAIR images show superiority for the detection of leptomeningeal disease (Figs. 5, 6). Therefore, the combination of unenhanced FLAIR and CE-FLAIR images can be a useful adjunct to CE-T1WI for the evaluation of leptomeningeal carcinomatosis (5101415182332).
Sturge-Weber Syndrome
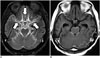
Contrast-enhanced-FLAIR imaging is helpful in depicting leptomeningeal angiomatosis in patients with Sturge-Weber syndrome. The major advantage of CE-FLAIR imaging over CE-T1WI is the lack of enhancement in the normal vascular structures. CE-FLAIR imaging also provides better visualization of the lesion in Sturge-Weber syndrome with more extensive leptomeningeal enhancement than CE-T1WI on the clinically suspected side (Fig. 7). Furthermore, CE-FLAIR imaging is helpful in detecting mild disease and unexpected bilateral disease (1833).
Rheumatoid Arthritis-Associated Leptomeningeal Disease
Rheumatoid leptomeningitis is a rare but serious complication of rheumatoid arthritis. Characteristic MRI findings are high signal intensity lesions in the subarachnoid spaces on FLAIR images or diffusion-weighted images (DWIs) and meningeal thickening with enhancement (Fig. 8). Leptomeningeal abnormalities are relatively focal in most cases. The basal cisterns are usually not affected in previously reported cases. CE-FLAIR imaging aids in the early diagnosis of leptomeningeal abnormalities in rheumatoid arthritis patients with CNS involvement because it shows more prominent enhancement than CE-T1WI. Additionally, the presence of serum anti-cyclic citrullinated peptide antibodies may be helpful in making the diagnosis (343536).
Pachymeningeal Lesions
Normal dura mater shows subtle thin and discontinuous enhancement that is prominent at the parasagittal location on CE-T1WI due to the lack of sufficient water to generate the T1 shortening required for avid enhancement. Abnormal meningeal enhancement is usually asymmetrical, thick, nodular and continuous, and extends deep into the sulcal bases (93738).
Postoperative Changes
Patients who have undergone intracranial surgery show postoperative dural enhancement. The enhancement is smooth and linear and can be seen as soon as 9 hours after surgery (Fig. 9). Moderate or marked dural enhancement was noted in all patients within 3 months after surgery with approximately 50% decrease in enhancement 1-2 years thereafter (93940). CE-FLAIR images demonstrate more extensive and persistent dural enhancement than CE-T1WI.
Trauma
Post-traumatic dural enhancement implies considerable head injury, although there is no obvious traumatic brain lesion on routine sequences. CE-FLAIR images are highly effective for detection of dural enhancement in patients with acute or chronic head injury, as compared with CE-T1WI. Even minor lacerations that cause bleeding into the CSF are sufficient to induce contrast enhancement on CE-FLAIR images (Fig. 10). Radiologists should focus on detecting traumatic brain lesions such as a small amount of subdural hemorrhage or subarachnoid hemorrhage, in cases with abnormal dural enhancement on CE-FLAIR imaging. Additionally, this finding could be more important in cases of suspected intracranial injury caused by child abuse because subdural hemorrhage is the most frequently detected form of intracranial abnormality in these patients (184142).
Dural Metastatic Lesions
The cancers associated with dural metastases are breast cancer, lung cancer, prostate cancer, and lymphoma. Dural metastases usually occur as an extension of the tumor to the dura from the adjacent calvarial metastases. Isolated dural metastases are relatively rare (434445). Imaging findings of dural metastases appear as focal nodular or diffuse enhancing dural masses. CE-FLAIR imaging has diagnostic potential equivalent to that of conventional CE-T1WI (Fig. 11) (46).
Meningioma
Meningiomas are the most common extra-axial tumors in the brain. CE-FLAIR imaging demonstrates a typical peripheral enhancement pattern related to the dual vascular supply of the tumor that is more commonly seen in larger meningiomas (> 2 cm in diameter). The highly vascular central part of the meningioma, supplied by meningeal arteries, enhances strongly on CE-T1WI, while a high concentration of Gd in the central part induces signal loss on CE-FLAIR imaging. The less vascular capsule, supplied by pial arteries, may have a lower concentration of Gd, resulting in peripheral contrast enhancement on CE-FLAIR imaging (Fig. 12). However, in tumors less than 2 cm in diameter, this effect is masked and only homogeneous enhancement is shown (474849).
Cranial Nerve Lesions
Diagnosis of Facial Neuritis
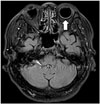
Contrast-enhanced T1WI plays a limited role in the evaluation of facial neuritis due to prominent normal facial nerve enhancement. The geniculate ganglion, greater superficial petrosal nerve, and proximal tympanic and mastoid segments of the normal facial nerve can be enhanced due to the flux of contrast material in the arteriovenous plexus (AVP) along the facial nerve (5051). Thus, evaluation of the pathologic enhancement of the nerves from the breakdown of the blood nerve barrier can be inhibited. CE-FLAIR imaging has an advantage over the CE-T1WI in the evaluation of the pathologic enhancement of the facial nerve because prominent enhancing AVP surrounding the normal facial nerve is no longer visible on CE-FLAIR imaging due to flow-related signal loss and high Gd concentrations in the AVP. Therefore, enhancement of the canalicular and anterior genu segments are significantly correlated with the presence of facial palsy on CE-FLAIR images (Fig. 13) (5253).
Hyperintense Acute Reperfusion Marker (HARM)
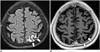
Hyperintense acute reperfusion marker describes an imaging phenomenon of enhancement of the subarachnoid CSF space, not enhancement of the parenchyma, on FLAIR imaging, and is caused by leakage of Gd through a disrupted BBB. It has been described in various clinical conditions, including acute ischemic stroke, endovascular treatment for severe carotid artery stenosis and cardiac surgery.
HARM Sign after Acute Ischemic Stroke
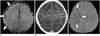
Hyperintense acute reperfusion marker was found in 30-40% of patients with acute stroke and approximately 20% of patients with transient ischemic attack without DWI lesions (Fig. 14). It is reportedly associated with age, reperfusion, thrombolysis, endovascular procedures, increased matrix metalloproteinases, higher Gd dosage and reduced kidney function (135455565758596061). While some studies show an increased risk of hemorrhagic transformation in patients with HARM (5456), recent studies do not show this association (6162).
HARM after Carotid Stent Insertion
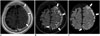
Hyperintense acute reperfusion marker was found in approximately 60% of patients after carotid artery stenting (CAS) (Fig. 15). The physiologic mechanism of delayed CSF enhancement after CAS is not obvious. However, previous studies have suggested that changes in BBB integrity due to sudden poststenting hemodynamic changes or reperfusion injury resulting from ischemic intolerance may be related to BBB disruption and the development of delayed CSF space enhancement after CAS. The majority of HARM after CAS is transient and not associated with the sudden development of neurological symptoms (636465).
HARM after Cardiac Surgery
Hyperintense acute reperfusion marker was found in approximately 50% of patients after cardiac surgery, and 75% of the patients have acute lesions on DWI. The proposed mechanisms for BBB disruption after cardiac surgery are ischemia due to hypoperfusion, activation of inflammatory cascades and proteolytic enzymes. The incidence of HARM was higher in patients who received Gd during the first 24 hours after surgery (6667).
Diabetic Retinopathy
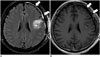
Contrast-enhanced FLAIR images can demonstrate ocular enhancement that is most commonly associated with diabetes. In patients with diabetic retinopathy, blood vessels in the retina may swell and leak fluid, presumably inducing contrast enhancement (Fig. 16). Despite the few studies on the clinical importance of this ocular enhancement, it might correspond to the development of diabetic retinopathy (5).
Hyperglycemia-Induced Seizures
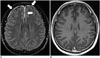
Patients with seizures in nonketotic hyperglycemia may have transient MRI abnormalities that are characterized by subcortical T2 hypointensity with overlying cortical or leptomeningeal enhancement in addition to cortical swelling. Enhancement of the leptomeninges likely occurs due to seizure-induced dilatation of leptomeningeal vasculatures, and cortical enhancement is believed to be the result of seizure-induced hypoxia and acidosis with alteration of vascular permeability and breakdown of the BBB (6869). CE-FLAIR is superior to CE-T1WI for the detection of focal cortical or leptomeningeal enhancement because CE-FLAIR images do not show contrast enhancement in normal vascular structures and normal meninges (Fig. 17).
Gd Encephalopathy Related to Renal Failure
Following Gd administration, patients with renal insufficiency can show CSF hyperintensity on FLAIR imaging due to diffusion of Gd into the CSF. Gd chelates are excreted mainly by glomerular filtration. In patients with renal impairment, the mean elimination half-life increases in relation to the degree of renal compromise. Because free Gd is a potent toxin, commercial MR contrast agents use Gd complexed with chelates to minimize free Gd levels in the serum. However, complexes undergo dissociation to release free Gd if they are retained for a prolonged duration in the circulation. Therefore, if renal function is compromised, Gd can accumulate to toxic levels and produce neurotoxicity (seizures or headache), although the reported rate of Gd neurotoxicity in patients with renal failure is < 1%. The recognition that patients with renal failure can show increased signal intensity in the CSF may prevent diagnostic errors such as subarachnoid hemorrhage, meningitis, meningeal carcinomatosis or leptomeningeal metastasis (707172737475).





 XML Download
XML Download