

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Thoracolumbar spine trauma is very common and accounts for 75-90% of all spine fractures (12). Various classification systems have been proposed and revised extensively based on anatomic location (e.g., the Denis three-column system) or injury mechanism (e.g., American Orthopedic [AO] classification), but these have limitations in that they cannot explain the patient's neurological state, they overlook the importance of posterior ligamentous complex integrity (PLC) as a prognostic factor, or show poor inter-reader or intra-reader reliabilities (34567891011). To overcome these shortcomings, the Spine Trauma Study Group (STSG) introduced a new thoracolumbar injury classification system, specifically the thoracolumbar injury classification system and severity score (TLICS), in which the type of injury morphology, integrity of PLC, and neurological status are scored (12). Although reliability of the TLICS is only fair in early studies (131415), many authors have demonstrated better reliability of the TLICS to shed light on its usefulness in daily practice (161718192021222324). However, these studies were carried out by clinicians, such as neurosurgeons, orthopedic surgeons, or trauma surgeons, who have the patient's clinical information, whereas radiologists actually read the majority of images in many hospitals. Therefore, we were curious about the reliability of TLICS among radiologists, based on magnetic resonance imaging (MRI), as MRI may be the most useful imaging modality for evaluating spine trauma, particularly PLC (2526). No study has reported on the TLICS from the radiologist's perspective; thus, the aim of this retrospective study was to evaluate inter-reader and intra-reader reliabilities of MRI in the TLICS for assessing thoracolumbar spinal injuries and to analyze the effect of reader experience on the reliability and the possible reasons for discordant interpretations.
MATERIALS AND METHODS
Patients
This retrospective study was approved by the Institutional Review Board of our hospital, and informed consent was waived. Sample size was estimated as follows. If the expected lower boundary for a kappa one-sided 95% confidence interval (CI) was 0.35 and the expected preliminary kappa value was 0.5, a minimum of 100 subjects was required for this study of inter-reader agreement by six raters, with prevalence of 0.1. We estimated sample size using the kappaSize library statistical program in R-project (R Core Team [2012]. R: A language and environment for statistical computing; R Foundation for Statistical Computing, Vienna, Austria. http://www.R-project.org/) (27). We included patients who had visited the emergency room of our hospital for suspected thoracolumbar traumatic injury from July 2010 to July 2011 and underwent thoracolumbar MRI within 24 hours after their trauma. Exclusion criteria were 1) history of thoracolumbar spine surgical history and 2) poor image quality. After searching our picture archiving and communication system, 100 consecutive thoracolumbar spine MRI examinations were enrolled in the study. There were 45 males and 55 females with a mean age of 57.6 years (range, 11-89 years). Among the 100 patients, 79 received conservative management, including vertebroplasty and 21 underwent surgery.
MRI Examinations
Of the 100 MRI examinations, 15 performed were outside of the hospital before visiting our emergency room. Eighty-five MRI examinations were performed in our hospital, of which 50 involved contrast enhancement (gadodiamide [Omniscan]; GE Healthcare, Princeton, NJ, USA). Seventy-five patients were scanned in the lumbar spine area and 22 had their thoracolumbar spine investigated by MRI. Three patients underwent whole spine MRI scanning from the skull base to the sacrococcygeal junction on the sagittal plane, and contrast enhancement was used in two. T2-weighted short time inversion recovery (STIR) sagittal scanning was also performed in 89 patients. Ninety-eight MRI examinations including all 15 outside hospital examinations were performed using 1.5 T MRI (83 examinations in our hospital with an Integra 1.5 T, Philips, Best, the Netherlands) and two were done using a 3 T MRI (Achieva 3T, Philips). The MRI parameters are listed in Table 1.
Image Interpretation
All MRI images were reviewed independently by six radiologists (two senior radiologists; one specializing in spine radiology with 11 years experience and one with 4 years experience), two junior radiologists (both specializing in spine radiology with 1 year experience), and two residents (one fourth-year and one third-year). Before the image evaluation, all six radiologists were asked to read two articles about TLICS (1225) to understand the use of TLICS in terms of reading spine MRI examinations, without a consensus meeting. The six radiologists evaluated the 100 MRI images independently and scored injury morphology using four scales of compression fracture, burst fracture, translation/rotation injury, and distraction injury, as well as PLC integrity using three 3 scales of intact, suspected/indeterminate, and injured based on the TLICS. All readers re-evaluated the images 6 months later to determine intra-reader reliability.
Statistical Analysis
Inter-reader agreement between the six readers on the TLICS scores related to injury morphology and PLC integrity was calculated using the Fleiss kappa (k) value. Fleiss' k was used instead of Cohen's k, as it allows comparing multiple readers using multiple scoring, as required in this study (28). The 95% CIs for the k statistic were calculated using the bootstrap method. Inter-reader agreement for the TLICS scores between two readers, such as the two senior radiologists, the two junior radiologists, and the two residents, as well as intra-reader agreement were estimated using Cohen's k. The k value was defined as slight (0-0.20), fair (0.21-0.40), moderate (0.41-0.60), substantial (0.61-0.80), and almost perfect (0.81-1.00). The statistical analysis was performed using Stata 10.0 (StataCorp, College Station, TX, USA). The relationship between injury morphology and PLC integrity was evaluated using Spearman's coefficient analysis and the treatment option (non-surgical vs. surgical treatment) according to the total injury morphology and PLC integrity scores of each reader using the chi-square test and PASW ver. 17.0 software (SPSS Inc., Chicago, IL, USA). The chi-square test was used to compare the TLICS scores for injury morphology and PLC integrity between patients who were treated operatively and non-operatively. A p value < 0.05 was considered significant.
RESULTS
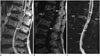
Inter-reader agreement between the six readers was moderate for the TLICS score for injury morphology (k = 0.538 for the first and 0.537 for the second review) and fair to moderate for PLC integrity (k = 0.440 for the first and 0.389 for the second review). After grouping the readers according to experience, the inter-reader agreement between two readers was spread widely, such as moderate to substantial agreement for injury morphology (k = 0.509-0.664) and fair to substantial for PLC integrity (k = 0.349-0.618) regardless of the radiologist's years of experience (Table 2). No difference in inter-reader agreement was detected over time. Intra-reader agreements were moderate to almost perfect for injury morphology (k = 0.538-0.822) and moderate to substantial for PLC integrity (k = 0.423-0.646) without a difference according to years of experience (Table 3). The majority of the 100 patients had a compression or burst injury (injury morphology scores 1-2) (Figs. 1, 2). All readers agreed that 44 patients in the first and 45 in the second reviews had the same injury morphology (Table 4). However, the readers failed to agree on the injury morphology of > 50% of the patients after the first and second reviews, in which the majority had compression vs. burst injuries (Table 4). The readers had difficulties distinguishing between burst and distraction injury in nine patients on the first and seven patients on the second review (Fig. 3). Two patients in the first review and six in the second review received various scores for all injury morphology types by the six readers, including the compression, burst, translation/rotation, and distraction injury patterns.
Forty-one patients in the first review and 38 in the second review were regarded as having PLC status by all readers. Among the cases of disagreement, 27 patients in the first review and 29 in the second review were thought to be "intact" or "indeterminate", and nine in the first review and five in the second review were considered "indeterminate" or "injured". Moreover, four patients in the first review and six in the second review were regarded as "intact" or "injured" with disagreement. Unlike injury morphology, in which only two in the first review and six in the second review had various injury morphology scores, 19 cases in the first review and 22 in the second review showed a wide range of PLC integrity scores (Table 4, Figs. 1, 4). Disrupted PLC was the agreed condition by all readers for four of 14 patients in the first review and three of 18 in the second review with a suspected distraction injury by any reader.
A positive correlation was detected between injury morphology score and PLC integrity, indicating that a higher injury morphology score resulted in a higher PLC integrity score, and vice versa, although there was a variable degree of correlation (Spearman's coefficient, 0.365-0.635 for the first review and 0.249-0.614 for the second) (Table 5).
No difference was observed between non-surgical and surgical treatment according to the total injury morphology and PLC integrity scores (total sum of injury morphology and PLC integrity scores < 5 vs. ≥ 5) by all six readers in the first review. The total score was not different among the four readers on the second review, except two (p = 0.004 and 0.012).
The TLICS scores of injury morphology and PLC integrity were significant different between patients who received non-operative or operative management by all six radiologists during the first and second reviews (p < 0.000), except for the injury morphology score during the second review by one radiologist with borderline significance (p = 0.006).
DISCUSSION
Many classification systems have been proposed, but the Denis and AO classification systems have been widely accepted for spinal instability and recognition of the importance of PLC (293031). However, these systems have been criticized for their complexity (e.g., AO classification) or their inability to represent future spinal instability. Therefore, the STSG proposed a new TLICS classification system in 2005 (12) and its clinical usefulness has been suggested (222324). However, reliability studies on the TLICS system have been performed exclusively by neurosurgeons or orthopedic surgeons (131415161718192021222324), and the reliability of the TLICS has not been evaluated by radiologists.
Inter-reader reliability for injury morphology and PLC integrity of TLICS was only fair in several initial studies but was moderate to almost perfect for neurologic state and management decisions (131415), which may have influenced their study design, as all readers were neurosurgeons or orthopedic surgeons and were informed about patient clinical neurological status. Later authors demonstrated better inter-reader reliabilities of moderate to substantial (161718). In our study, conducted exclusively by radiologists, inter-reader agreement of the six radiologists was moderate for injury morphology and fair to moderate for PLC integrity, which was relatively low, and similar to those previous studies. Intra-reader agreement was also relatively low, particularly for PLC integrity with a moderate to substantial k value.
Some authors have evaluated whether reliability differs over time or according to a clinician's experience (1920). However, time-dependent improvement in reliability was not explained, because the readers were different in the second session of the study (19) and the difference in k was too minimal to show a significant difference between junior and senior groups (20). In our study, inter-reader agreement between thee sets of two readers revealed no differences regardless of the radiologist's experience.
A previous study reported some confusion regarding injury morphology (32). All readers agreed about the injury morphology of some patients, but the readers had difficulties distinguishing between compression and burst injuries in many patients. Only one case was suspected of suffering a translation/rotation or distraction injury with a disrupted PLC. This result suggests difficulty distinguishing between translation/rotation or distraction injury with definite disruption of the PLC and facet joint dislocation/subluxation.
The usefulness of MRI, particularly T2-weighted fat-suppressed images, for assessing PLC integrity has been suggested (3334353637383940). However, there is no consensus about which finding is most diagnostic when evaluating PLC integrity (41). Two studies have revealed that the reliability of PLC integrity is poor or moderate (4243). In contrast, some authors have questioned the role of MRI for assessing PLC integrity, as there are concerns about over- or understanding PLC disruption using MRI findings alone (4445). Our readers could not agree about PLC status in > 50% of patients, which may be due, in part, because the most useful MRI findings to diagnose PLC disruption have not been determined, resulting in the ambiguity of "indeterminate" PLC status on MRI (46). PLC integrity may tend to be determined as disrupted PLC if there is a fracture or marrow edema in the posterior bony compartment. Moreover, the TLICS system scores only the most severe injured level but some problems may occur clinically in cases with discordant features between injury morphology and PLC integrity.
We found that injury morphology severity and PLC integrity were correlated. The TLICS was designed to focus on PLC integrity; thus, radiologists tend to be hyper aware of PLC status on MRI, resulting in assigning more severe injury morphology in cases of suspicious disruption of the PLC.
However, although the intra-reader and inter-reader agreements were relatively low in this study and there was a concern about over-estimating injury morphology and PLC integrity, which may be dependant on each other, a significant difference was detected in injury morphology and PLC integrity between patients who received non-operative or operative management, suggesting that the TLICS system can be used to clinically determine the surgical option and is well-correlated with clinical manifestations.
Our study included 15 MRIs taken at other hospitals with different MRI parameters including T2-weighted STIR sagittal scans, which were appropriate for evaluating PLC integrity. Thus, including outside MRIs was helpful for the TLICS evaluation in an actual clinical setting.
Several limitations of this study should be mentioned. First, the gold standard for accurately assessing injury morphology and PLC integrity was not defined because only 21 patients underwent surgery. Second, we could not define the diagnostic MRI findings for the injury morphology and PLC status of individual cases. Third, only one case of suspected transitional/rotational injury was included, and the majority of cases were compression/burst injuries. Fourth, we could not compare the long-term clinical outcomes according to the TLICS score to determine its clinical and radiological usefulness. Fifth, heterogeneous MRI parameters were used for outside hospital examinations, and a very small number of MRI examinations were performed using 3 T MRI, which may caused heterogeneity in the enrolled cases. Sixth, we did not exclude elderly patients with underlying osteoporosis.
In conclusion, the reliability of MRI for radiologists, who were blinded to clinical information, such as physical examination findings, to evaluate thoracolumbar spinal injury was moderate for injury morphology and fair to moderate for PLC integrity and did not differ based on the experience of the radiologist.








 XML Download
XML Download