

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Radiculopathy from nerve root irritation is frequently encountered in degenerative lumbar spine disease, most commonly as a result of disc herniation. Ozone is an unstable, strongly oxidizing gas with anti-septic, immunomodulating, analgesic, and anti-inflammatory properties (12). Oxygen-Ozone (O2-O3) nucleolysis is a minimally invasive therapy for the treatment of disc herniation that is often combined with periradicular administration of steroids and local anesthesia (3,45). Many studies, along with the evaluation of the morphology changes in lumbar disc herniation, have investigated the prognostic value of magnetic resonance imaging (MRI) in the patients treated conservatively. Using MR imaging, Komori et al. (6) reported that large sequestered or extruded disc herniation were frequently decreased in size after conservative treatment. As previously described, examining the prognostic value of post-contrast MR imaging enhancement in lumbar discs, in addition to its high diagnostic value, offers predictive information about disc-herniation evolution (7). A recent study has also demonstrated that a significant reduction in the apparent diffusion coefficient (ADC) of the treated discs was shown around the second month, and herniation volume reductions were shown around the sixth month of follow-up after O2-O3 diskolysis (8). However, these data could not predict the response of herniated discs treated with O2-O3 injection.
Diffusion weighted imaging (DWI) based on MR imaging can provide valuable information regarding the microstructure of tissues, by applying a motion probing gradient (MPG) in some directions to monitor the random movement of water molecules, which is restricted in tissues (9,10,11). Recently, it has been reported that DWI is useful for the evaluation of peripheral nerve compression disorders, such as carpal tunnel syndrome (12,13,14). Chen et al. (15) demonstrated that the functional MR imaging can potentially be used to assess the symptomatic cervical nerve root entrapment syndromes.
Even though several studies have investigated the relationship between MR findings and clinical outcomes after the injection therapy, it is still difficult to predict the clinical outcomes of the injection therapy. Besides, if DWI is able to demonstrate these inflammatory changes after O2-O3 injection, it may then be possible to establish an objective diagnostic method. Our purpose was to determine whether a change in ADC value could predict early response to CT-guided O2-O3 injection therapy in patients with unilateral mono-radiculopathy due to lumbar disc herniation.
MATERIALS AND METHODS
Written informed consents were obtained from all of the patients who participated in this study, and this protocol was approved by our ethics committee.
Patients
This was a prospective study conducted to evaluate the effect of O2-O3 therapy on patients with lumbar disc herniation. From August 2009 to March 2013, a total of 52 consecutive patients (22 women, 30 men; age range, 22-77 years; average age, 50.1 ± 14.8 years) with single level lumbar disc herniation (L3-4, 3 patients; L4-5, 12 patients; L5-S1, 37 patients) and radicular pain were included in this study. The mean duration of radicular pain at the time of treatment was 18 weeks. Preliminary clinical evaluation was performed by one experienced neurosurgeon.
Patient inclusion criteria were as follows: 1) mono-radicular pain, 2) lumbar disk herniation on CT or MR images, 3) herniation site congruous with the neurologic level, 4) complaint of pain for at least 8 weeks, which was shown in all patients, and 5) having received conservative therapy (physiotherapy and/or nonsteroidal anti-inflammatory drugs and/or intramuscular steroids) for 2-4 weeks with no or poor clinical improvement.
Patient exclusion criteria were as follows: 1) pregnancy, 2) recorded allergy to proposed drugs, 3) major neurologic deficits, 4) hemorrhagic diathesis, 5) suspected spondylodiscitis, and 6) previous spine surgery.
Procedure
The disc level to be treated was decided by comparing morphological data, patient's history, MR imaging, and clinical examination in consensus with an experienced neurosurgeon. Computed tomographic (CT) (MX 16, Philips Medical Systems, Eindhoven, the Netherlands) sections for planning were obtained in 3-mm slice thickness, parallel to the edge of the vertebra, with the patient in prone position. Next, a CT-guided discography was performed under local anesthesia, according to the path and angle determined by the CT scan (Fig. 1). All interventions were performed by a single interventionist with more than 8 years of experience in spine interventions. Under CT guidance, all patients received an identical intradiscal (3 mL) and periganglionic (5 mL) injection of O2-O3 mixture (ratio = 3:97; ozone concentration of 30 g/mL) followed by a periganglionic injection of corticosteroid (1 mL triamcinolone acetonide; Lisapharma, Vio Licinio, Italy) and anesthetic agent (2 mL lidocaine hydrochloride 0.25%; Southwest Pharmaceutical Co., Ltd., Chongqing, China) in the same session (Fig. 1). Intradiscal and periganglionic injection was performed by the means of an extraspinal lateral approach with a 19-gauge, 14-cm puncture needle (Monopty 2016B, Bard Inc., Covington, GA, USA) from the same side as the main location of symptoms. In the present study, we treated a single lumbar disc level with a single session of O2-O3 injection. The access side corresponded to the site of pain, in the case of unilateral pain. After the nucleolysis procedure, the patients were asked to take a bed rest for 12 hours and to avoid strenuous activities for 3 days. All patients were discharged on the following day.
MRI Protocol
A 3.0-T MR imaging scanner (Discovery MR750; GE Healthcare, Milwaukee, WI, USA) was used in this study. Subjects were scanned in a supine position, by using a Sense XL Torso coil. DWI was performed using single shot-spin echo planar imaging sequence with a free breathing scanning technique. The following imaging parameters were set: parallel imaging technique, array spatial sensitivity encoding technique (ASSET); b value, 0 and 1000 s/mm2; MPG direction phase; 2300/66 ms for repetition time/echo time, respectively; axial section orientation, 25 slices, 3-mm section thickness, no gap; 320 × 256 mm field-of-view; 128 × 128 matrix; 2.8 × 2.8 × 3.0 mm3 voxel size; 12 excitations; 2 minutes 14 seconds scan time. Scanning was performed at and around the affected roots level.
Image Analysis
After transferring DWI data to GE advantage workstation 4.4 (GE Healthcare), circular regions of interest (ROIs) were placed in anatomical locations on the most significant levels for spinal disorders, by using b = 0 and b = 1000 images. The mean values from the ROI were measured in each nerve root (Fig. 2). To assess inter-observer variability, two neuroradiologists, each with more than 5 years of experience (7 and 8 years of experience, respectively), independently reviewed the initial and repeat MRI datasets. For both datasets, each rater was instructed to select the image slices that provided maximal transverse cross-sectional area of each nerve root to be measured. ADC was calculated from the mean value of the appropriate ROI using the following formula: ADC = (SIb = 1000 - SIb = 0) / 1000 (SIb = 1000, SIb = 0: mean value in ROI, respectively, indicates b = 1000 and b = 0). The index of the involved side to the intact side of ADC (ADC index) was calculated using the following formula: ADC index = ([ADC involved side - ADC intact side] / ADC intact side) × 100.
Clinical Outcome Measurement
Patients were followed-up after 1 month to determine the effectiveness of the procedure. We provided the Oswestry Low Back Pain Disability Questionnaire (16) for every patient on the day of the procedure and after 1 month. The response to treatment was considered binary, which was categorized as successful (responders) if the Oswestry Disability Index (ODI) was no greater than 20% at follow-up, and unsuccessful (non-responders) if otherwise (17). Patients who did not return the questionnaire were contacted and verbally questioned on telephone. The recovery rate of the ODI score is the degree of recovery after the procedure, which was calculated at 1 month follow-up by using the following formula: ODI recovery ratio = ([ODI preop - ODI postop] / ODI preop) × 100.
Statistical Analysis
Reproducibility of ADC values were then evaluated using intraclass correlation coefficients (ICC). ICC values greater than 0.75 were considered to demonstrate excellent reliability, values between 0.40 and 0.75 indicated fair to good reliability, and below 0.40 showed poor reliability (18). The Mann-Whitney U-test was used to determine the differences between the responder and non-responder groups in terms of ADC index. Spearman's rank correlation was used for evaluation of the relationship between the ADC index and clinical parameters, such as ODI × 100 and ODI recovery ratio. For receiver-operating characteristic (ROC) curve analysis, successful outcomes (responders) were considered as positive test result, and unsuccessful outcomes (non-responders) indicated negative test result. The area under the ROC curve (AUC) was calculated, and the cut-off values with the largest Youden index (the sum of sensitivity and specificity) was calculated from the ROC curve. All statistical analyses were performed using SPSS version 17.0 for Windows (SPSS Inc., Chicago, IL, USA). The p value below 0.05 was considered to be significant.
RESULTS
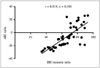
Inter-observer agreement of confidence levels for each reader was adequate for ADC measurement (ICC = 0.834, 95% confidence interval [CI] = 0.776 to 0.917). Thirty-six patients out of 52 had successful outcomes (responders), whereas sixteen patients showed unsatisfactory outcomes (non-responders) during the follow-up period of first month. The mean ADC index of responders was 13.022 ± 9.946, which was higher than the -14.484 ± 12.756 of non-responders (p = 0.012) (Fig. 3). There was no correlation between the ADC index and ODI (r = -0.125, p = 0.093) (Fig. 4). Figure 5 shows the relationship between ADC index and ODI recovery ratio with procedure, where a statistically positive correlation was observed (r = 0.819, p < 0.001).
Diagnostic Accuracy
Using 7.10 as the cut-off value in our study, ADC index obtained sensitivity of 86.3% and specificity of 82.9% for predicting the successful outcomes, and the AUC was 0.86 (95% CI = 0.72-0.94) (Fig. 6).
DISCUSSION
The incidence of nerve root entrapment has been reported to be between 8 and 11% in degenerative lumbar disease (19), but the underlying pathophysiology remains unclear. A higher incidence of foraminal stenosis was found in the lower lumbar segments (20). Jenis and An (21) reported that the most commonly involved roots are the L5 (75%) followed by L4 (15%) and others (4%), which is consistent with our findings. Periganglionic and intradiscal injection of O2-O3 has been proposed, since the late 1990s, as a treatment for lumbar disc herniation (22,23,24). CT-guidance improves precision and safety in spinal injections. Due to improved visualization by CT and a longer lasting effect of O2-O3, CT-guided injection has been found to be superior to fluoroscopy-guided injections (25). In our study, 36 out of 52 patients (approximately 70%) had successful outcomes (the responders), whereas 16 patients showed unsatisfactory results (the non-responders) after a follow-up period of one month, which is within the range similar to that of prior studies (12224).
Our study found no correlation between ODI and ADC index. These results are consistent with the results reported by Takashima et al. (26). Studies that focused on diffusion MRI of the affected nerve, such as Mac Donald et al. (27), used a mouse brain injury model with a time span of 1 to 4 weeks after trauma. The study reported that within 6 hours to 4 days after trauma, relative axial diffusivity corresponding to axonal injury was reduced, whereas radial diffusivity corresponding to demyelination, edema, and persistent axonal injury was increased. By using a rat sciatic nerve crush injury model, Morisaki et al. (28) showed decreased fractional anisotropy (FA) in the degenerative phase and a late increase in FA during the regenerative phase. The changes in ADC and the eigenvalues occur by various factors including membrane integrity, axonal swelling, and axonal flow (2930). Therefore, our results suggest that it is difficult to assess the degree of nerve root compression from ADC. In contrast, a positive correlation was observed between ADC index and ODI recovery ratio. Improvement in clinical outcomes after the CT-guided injection therapy showed a decreasing trend in the subjects with reduced ADC of the affected nerve root, compared to the unaffected side.
Many studies have investigated the prognostic value of MR imaging in the patients treated with different procedures; and MR imaging was utilized to evaluate the morphology changes in lumbar disc herniation and the degree of nerve root compression (7). However, these data could not predict the responses of radiculopathy treated with CT-guided O2-O3 injection. To our knowledge, the only study on predicting the outcome using DWI-ADC was performed by Takashima et al. (26). In comparison to his study, we used a 3.0-T scanner in our research for a better signal-to-noise ratio which should theoretically be double when compared with a 1.5-T scanner (31). In this study, a parallel imaging technique (ASSET) was also applied in DWI, since a higher magnetic field is more sensitive to the susceptibility artifacts. Parallel imaging techniques can limit the susceptibility artifacts by shortening time of echo and overall imaging time (3233). A decreased ADC of the affected nerve root in this study suggested a decrease in axonal flow and stagnation of water molecules in cellular edema. This suggests that there is a connection between the recovery of nerve function in the compressed nerve root and improved intraneural blood flow (34). Furthermore, it has been reported that axonal flow in dorsal root nerve fibers is disturbed as a result of nerve root compression, and this disturbance is considered to reduce the recovery of nerve function (35). Therefore, our findings demonstrate that the high ADC index may be correlated with a good outcome after the procedure. To the best of our knowledge, this is the first article regarding the predictive value of DWI-ADC in predicting the outcomes of patients with radiculopathy, who received CT-guided O2-O3 injection therapy. Using 7.10 as the cut-off value, ROC analysis revealed that ADC index could predict early response to CT-guided injection therapy in radiculopathy, with 86.3% sensitivity, 82.9% specificity, and 86% accuracy.
We acknowledge that our study has several limitations. The first is that a small number of subjects were investigated. Further studies are needed to investigate whether our findings remain valid in a larger population. Secondly, we did not evaluate post-interventional ADC in this study, as ADC could not be measured accurately due to adhesions of the surrounding tissue developing in the post-interventional nerve root. Thirdly, ADC maps were limited, because the tissue contrast between the nerve and surrounding tissue was poor.
In conclusion, our results indicate that the patients with decreased ADC index tend to show poor improvement of clinical symptoms. The ADC index may be a useful indicator to predict early response to CT-guided O2-O3 injection therapy in the patients with unilateral mono-radiculopathy due to lumbar disc herniation.





 XML Download
XML Download