

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The most common malignant renal tumors are renal cell carcinomas (RCC). However, unusual types of renal tumors may occur in the renal parenchyma and mimic RCC on cross-sectional imaging studies. Awareness of the imaging findings of these tumors helps radiologists with diagnosis and treatment. In this pictorial essay, we present the computed tomography (CT) and magnetic resonance imaging (MRI) features of unusual solid renal tumors, such as a primitive neuroectodermal tumor (PNET), primary liposarcoma, primary malignant neuroendocrine tumor, leiomyosarcoma (LMS), synovial sarcoma, malignant fibrous histiocytoma (MFH), sclerosing fibrosarcoma, and metastatic osteosarcoma.
Primitive Neuroectodermal Tumor of the Kidney
A PNET is a malignant small round cell tumor characterized by aggressive biological behavior with frequent recurrence and metastatic potential (1). These tumors are most frequently encountered in adolescents and young adults. The imaging features of a PNET are indistinguishable from RCC. PNET of the kidney is mostly reported as a large mass with near-total replacement of the renal parenchyma (Fig. 1) (2). These renal lesions appear as a heterogeneous mass on CT. MRI reveals a low signal-intensity solid mass with lobulated contours on T1-weighted images and heterogeneous signal intensity on T2-weighted images. PNET of the kidney may extend to the renal veins and inferior vena cava (3).
Primary Liposarcoma of the Kidney
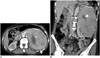
Sarcomas of the genitourinary tract are most commonly LMSs and can be detected in prostate, urinary bladder, kidney, and paratesticular areas (45). Liposarcomas account for 20% of all soft-tissue sarcomas in adults, and they are most commonly detected at 50-65 years of age with male predominance (6). Primary renal capsule malignancies are uncommon. Primary liposarcoma of the renal capsule is an extremely rare disease with only about 20 cases reported (6).
Liposarcomas are classified into five histological subtypes, including well-differentiated, dedifferentiated, myxoid, round cell, and pleomorphic. The histological grade is the most important prognostic factor (7). The most important clinical entity in the differential diagnosis is macroscopic fat-containing angiomyolipoma. However, it may be difficult to make a confident imaging diagnosis of any kind of lipomatous tumor when the lesion does not contain macroscopic fat, as in the case presented in Figure 2.
Primary surgical resection of the mass is the only potentially curative approach. It is difficult to provide any reliable information on the long-term results of this rare tumor, given the small number of patients.
Primary Malignant Neuroendocrine Tumor of the Kidney
Neuroendocrine carcinomas are found in different tissues and organs, including those that do not normally contain neuroendocrine cells (8). Neuroendocrine tumors of the kidney are extremely rare neoplasms and include carcinoids, atypical carcinoids, and small cell carcinomas (9). The prognosis differs according to disease stage. Another interesting point in patients with neuroendocrine tumors is the high incidence of a horseshoe kidney (10).
The peak incidence of neuroendocrine tumors occurs in patients in their 50s and 60s but patients as young as 12 years and those in their 70s have also been reported. Older age at the time of diagnosis (> 40 years) is correlated with an advanced disease stage and a worse prognosis (9). Surgical resection is the only known curative treatment, and the prognosis may be good even in patients with local lymph node involvement (10). Metastatic disease to the liver constitutes a grave finding; however, due to the rarity of the disease, no standard treatment protocol has gained universal acceptance (11).
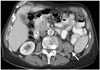
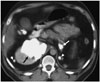
Among the most common radiological features of all neuroendocrine tumors is calcification (Fig. 3) (10). Although lesions may be heterogeneous on ultrasound (US) and CT, carcinoids of the kidney have a characteristic tendency to show minimal or poor enhancement on contrast-enhanced CT, corresponding to hypovascular or avascular lesions on renal angiography. Octreotide scanning has been recently proposed as a sensitive imaging modality for diagnosing and evaluating the extent of disease (10).
Renal Leiomyosarcoma
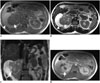
Renal LMS accounts for only 0.1% of all invasive renal tumors and 50-60% of all cases of renal sarcoma (12). These tumors most frequently arise from the renal capsule, smooth muscle fibers of the renal pelvis, sphincter ring around the renal papilla, and internal blood vessels (13). Spontaneous rupture of the kidney has been reported in patients with renal LMS (14). Renal LMSs appear as expansile, heterogeneously-enhancing, and well-circumscribed solid masses that usually project exophytically from the kidney (131516). Not surprisingly, the fibrous stroma of the tumor accounts for the T1- and T2-hypointensity and demonstrates delayed enhancement after intravenous injection of contrast agent (Fig. 4) (13). Large renal LMS may present as multilocular cystic masses with peripheral enhancement. A histopathological diagnosis is necessary, as these tumors cannot be distinguished from RCC and other renal malignancies.
Renal Synovial Sarcoma
Primary synovial sarcoma of the kidney is an extremely rare tumor. They tend to be large masses with a mean size of 8 cm (17). Renal synovial sarcomas manifest as a hypoechoic mass arising from the kidney on US. Synovial sarcoma of the kidney presents as a soft tissue mass with multiple cystic areas (Fig. 5) (3). They are usually well-demarcated, and cross-sectional imaging studies demonstrate an oval shaped, well-defined heterogeneously enhancing mass (1718). Small synovial sarcomas of the kidney usually have homogeneous signal intensity, similar to that of skeletal muscle on T1-weighted images. Synovial sarcomas > 5 cm can show heterogeneous signal intensity due to intralesional hemorrhage and necrosis (Fig. 5) (19). The cystic components of synovial sarcoma often have smooth walls unlike cystic RCCs, which usually have a mural nodule. Subcapsular hematoma secondary to tumor rupture may occur in patients with synovial sarcoma of the kidney (18).
Malignant Fibrous Histiocytoma of the Kidney
Malignant fibrous histiocytoma of the kidney is a rare tumor, and < 100 cases have been reported. MFH arises from the kidney capsule or renal parenchyma and represents 6% of renal sarcomas (2021). Most MFHs manifest as bulky tumors with extra-renal extension (22). They tend to recur locally and can be detected in 51% of cases during the disease course (2023).
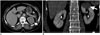
Malignant fibrous histiocytoma of the kidney presents as a well-defined soft tissue mass with inhomogeneous minimal enhancement with slightly higher attenuation than the skeletal muscle on contrast-enhanced CT (Fig. 6) (24). Decreased attenuation corresponding to regions of myxomatous tissue, cystic degeneration, hemorrhage, or necrosis is observed on CT.
Malignant fibrous histiocytomas of the kidney usually appear hypointense to kidney parenchyma on T1-weighted images, whereas they appear iso- or hyperintense on T2-weighted images (24). Hypointense areas on T1- and T2-weighted images reflect the fibrous components of the tumor and are a potentially useful clue for an imaging diagnosis of the lesion. Gradual and heterogeneous enhancement may be seen after intravenous gadolinium administration, reflecting the tumor's fibrous content (1624). Other sarcomas, sarcomatoid RCC, and malakoplakia should be considered in the differential diagnosis of renal MFH (2526).
Sclerosing Fibrosarcoma of the Kidney
Sclerosing fibrosarcoma of the kidney is a very rare subtype of renal sarcoma. Fibrosarcoma of the kidney usually arises from fibrous and connective tissue of the renal capsule (27). Fibrosarcomas appear as large heterogeneously enhancing soft-tissue masses on CT and MRI (Fig. 7) (13). The prognosis of this tumor is very poor, as the tumor presents with a rapid growth rate and aggressive behavior and the only potentially curative treatment is surgery (13).
Metastatic Osteosarcoma of the Kidney
Metastatic disease of the kidney is not common and is mostly seen in patients with a neoplasm of the lung, breast, gastrointestinal tract, or melanoma (28). Osteosarcoma of the kidney may be primary or more commonly metastatic. It is often bilateral, as in our case, and clinically silent (29). These lesions may show extensive calcification on radiographs, occasionally in a sunburst pattern, and may even be detectable on plain radiography (Fig. 8). Nuclear medicine scans with technetium-99 may demonstrate diffuse uptake (2). Clinically occult metastatic renal osteosarcoma is not rare and can be seen in 10% of autopsies of patients who die from osteosarcoma (30).
CONCLUSIONS
Solid renal masses without macroscopic fat on imaging studies are usually presumed to represent RCC. However, several malignant neoplasms may arise from the kidney. Familiarity with the imaging findings of these unusual malignant renal tumors is helpful to the practicing radiologist for a better diagnosis of these lesions.
Image-guided percutaneous renal biopsy has been increasingly used to characterize solid renal masses and may prevent unnecessary surgical intervention (31). Any lesion in the kidney can now be safely sampled with increased experience in percutaneous biopsy techniques. Percutaneous tract seeding has been a relatively common complication during biopsy of renal malignancies; however, several recent studies have demonstrated that percutaneous biopsy can be safely performed in these patients without any significant risk of tract seeding (313233).



 XML Download
XML Download