

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Contrast-enhanced computed tomography colonography (CE-CTC) is the best technique for colorectal cancer sites and staging (12), as well as to diagnose synchronous colonic lesions (3) in patients with obstructing cancers. CE-CTC is also useful to preoperatively evaluate others colorectal diseases, such as diverticular disease and inflammatory bowel disease (45). The laparoscopic approach for colonic surgery has become common and widely used because of the multiple advantages compared to conventional laparotomy. Laparoscopic surgery produces smaller surgical incisions, less intraoperative blood loss, faster recovery of normal bowel function, and shorter hospitalization (67). Nevertheless, the disadvantages to this approach include lack of a panoramic view of the operative field and tactile sensation, leading to potential inaccurate localization of a colonic lesion and difficulties with vessel ligation and lymph node dissection (8). Only a few studies have analysed the vascular anatomy of the colon using multidetector CT (91011) and only one used CT colonography (12).
Contrast-Enhanced CT Colonography Protocol
Bowel preparation consisted of a low-fiber diet and a mild laxative (macrogol solution) the day before CT. Faeces were tagged by administering 60-90 mL amidotrizoate meglumine and 500 mL water at least 3 hours before the examination. The colon was distended by insufflating at least 3 L of carbon dioxide using an automatic insufflator. A vial of hyoscine N-butylbromide was intravenously injected just prior to insufflation. We performed a pre-contrast scan with the patient in the prone position using low mAs and different post-contrast scans in the supine position after injecting 500-600 mgI/kg/body weight. Post-contrast scans may have included arterial (obtained using bolus-tracking monitoring technique), portal venous, and delayed phases depending on the disease.
Vascular Mapping
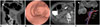
Comprehending the complex three-dimensional (3D) anatomy of the colon and branching vessels is difficult on axial images, particularly for inexperienced readers. 3D imaging provides surgeons with a precise and immediate understanding of the patient's anatomy, including colonic loop shapes, colonic lesion sites, and the courses and relationships of the branching vessels. We obtained 3D fused images using a dedicated workstation (Advantage Workstation 4, General Electric Healthcare, Waukesha, WI, USA) by processing the CT dataset from the arterial and portal-venous phases. Three reformations with different settings (3D colon map and two different 3D vascular presets) were prepared separately and fused together into a single volume, which included the 3D colon map, a 3D arteriogram, and a 3D venogram, with the mesenteric arteries colored in red and relevant venous branches colored in blue. This resulted in a colon map that overlapped with the vascular map and showed the mesenteric branching pattern and the relationships between the colonic lesions, arteries and veins. The 3D images could be tilted and rotated to obtain the view that best simulates the intraoperative field of view.
Benefits for the Laparoscopic Surgeon
CT colonography allows for an accurate pre-operative assessment of colonic anatomy, and the locations of the colonic lesions and lymph nodes. Post-contrast acquisition and the vascular map allow for a precise evaluation of mesenteric artery branching patterns and the relationships between arterial and venous vessels. Although the laparoscopic approach has many obvious benefits compared to laparotomy, it suffers from a restricted operative field of view and an inability to manipulate tissues, which can result in time-consuming dissections when searching for anatomical landmarks, lymph nodes, or vessels. Intraoperative conversion rates to laparotomy from laparoscopic colectomy are 10-20% (713) and is often due to difficulties identifying mesenteric vessels, synchronous tumors, intraoperative bleeding or procedure length (7). Complications, such as bleeding and bowel ischemia, can occur because of vascular injury while dissecting nodes or ligating a vessel. Previous knowledge of the patient's mesenteric vascular anatomy, including arterial branching variants and relationships with adjacent veins, reduces operative time and the incidence of intraoperative complications (11).
Main Vascular Variants Related to Colonic Laparoscopic Surgery
The branching pattern of the superior mesenteric artery (SMA) must be assessed before a right hemicolectomy and right transverse colon surgery. The middle colic artery (MCA) and the ileocolic artery (ICA) are present in almost all patients, whereas the right colic artery (RCA) is present in about 50% of cases (Figs. 1, 2). The inconsistency in the presence of the accessory left colic artery (ALCA), known as the artery of Riolan, originates from the SMA or MCA and anastomoses with the left colic artery (LCA), feeding the transverse colon (Figs. 3, 4). The common origin of the MCA, RCA, and ICA (Fig. 5) has been described (89). The most significant variant to be considered during laparoscopic right hemicolectomy is the relationship between the colic arteries and the superior mesenteric vein (SMV); arteries cross anterior to the SMV in most patients, but a posterior crossing pattern of the ICA, MCA, or RCA is also common (Figs. 5, 6). The ICA runs posteriorly to the SMV in 67% of cases (8). It is important to locate the ALCA and the branching pattern of the inferior mesenteric artery (IMA) when planning left transverse colon surgery and left hemicolectomy. The LCA is absent in 12% of individuals (Fig. 7) (14). The same considerations can be applied to sigmoid colon and rectal surgery. Moreover, pre-operative planning for sigmoidectomy should include an evaluation of the sigmoid artery (SA) branching pattern because the IMA can be preserved if the SAs are selectively ligated. The number of SAs varies and they can either originate from the IMA or LCA (Figs. 2, 4, 7) (15). The relationship between arteries and the inferior mesenteric vein (IMV) can also vary: LCA and SAs can either cross anteriorly or posteriorly to the IMV (Figs. 8, 9). Because of their close proximity, the relationships between the LCA, SAs, and the left gonadic vein and ureter must be assessed. The origins of other splanchnic arteries from the SMA or IMA must also be considered be. For example, right hepatic artery frequently branches from the SMA (Fig. 7) (15). Variants in mesenteric vein drainage should also be evaluated (Fig. 8).








 XML Download
XML Download