

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Ischemic stroke is one of the leading causes of death in elderly patients. Intravenous tissue plasminogen activator present within three hours of the onset of an event has been proven to improve clinical outcome (1). However, thrombolytic agents are associated with symptomatic intracerebral hemorrhage (ICH) (23). Many efforts have been made to identify and predict the hemorrhagic transformation. Among the many independent risk factors of symptomatic ICH, hypodensity on computed tomography has been reported to be an image-based risk factor (34567). There have also been studies using diffusion- or perfusion-weighted magnetic resonance images (891011121314). The studies have showen that the area with decreased perfusion, decreased apparent diffusion coefficient, and later reperfusion is associated with hemorrhagic transformation. Although the studies showed promising results for predicting hemorrhagic transformation, their observations are not directly targeted to the blood-brain interface. Permeability imaging using dynamic contrast-enhanced MRI (DCE-MRI) can measure the integrity of the blood-brain barrier (BBB) (1516171819202122). Because microvascular permeability plays an important role in the pathologic process of a stroke, disruption of the BBB is not only associated with hemorrhagic transformation but also with the evolution of the stroke (232425). Small animal models are indispensable for pre-clinical research. However, because institutes with dedicated in-vivo animal MR systems and coils are limited, few studies have investigated permeability imaging using an animal model. Therefore, the purpose of this study was to correlate permeability parameters measured with DCE-MRI using a clinical 3-T scanner with extravasation of Evans blue in a rat transient cerebral ischemic model.
MATERIALS AND METHODS
Middle Cerebral Artery Occlusion Model
This animal study was approved by and performed in accordance with the institutional guidelines of the Association for Assessment and Accreditation of Laboratory Animal Care International. Thirteen male Sprague-Dawley rats, 300-400 grams, were housed in an appropriate manner. The middle cerebral artery (MCA) occlusion model was generated as described elsewhere with modifications (2627). In short, rats were anesthetized with an intramuscular injection of a mixture of Zoletil (15 mg/kg) and Rompun (10 mg/kg). Rectal temperature, respiration, and heart rate were monitored and maintained in the physiological range throughout the procedure. The right common, internal, and external carotid arteries were exposed through a midline cervical incision. After ligation of the right common and external carotid arteries, a 4-0 nylon monofilament with a tip rounded by gentle heating was introduced via the right internal carotid artery to occlude the proximal MCA, distal internal cerebral artery, and anterior communicating artery. After an hour of transient occlusion of the MCA, the 4-0 nylon monofilament was removed to restore cerebral blood flow. A total of thirteen rats were included in this study.
MRI Acquisition
Animal MR imaging was performed using a 3-T system (Achieva, Philips, Best, the Netherlands) and an 8-channel SENSE wrist coil. Rats were anesthetized with an intramuscular injection of a mixture of Zoletil (15 mg/kg) and Rompun (10 mg/kg).
Dynamic Contrast-Enhanced MRI
MRI acquisition was set at 12 hours, 18 hours, and 36 hours after reperfusion to observe permeability parameters. Rats were imaged 12 hours after reperfusion (n = 3); 18 hours after reperfusion (n = 7); and 36 hours after reperfusion (n = 3). The tail vein was accessed and prepared for the intravenous injection of contrast media before obtaining the MR images. For DCE-MRI, precontrast 3-dimensional T1-weighted images were obtained with the following parameters: field of view (FOV), 60 × 60 mm2; matrix, 112 × 112; slice thickness, 4.4 mm; slice increment, 2.2 mm; and flip angle of 5°. After the precontrast scan, 60-dynamic contrast-enhanced T1-weighted images were taken with the same MR parameters except the flip angle was altered to 15° after a bolus injection of 0.2 mmol/kg gadolinium (gadobutrol, Gadovist; Bayer, Berlin, Germany) with a temporal resolution of 5 seconds. The total scan time for DCE-MRI was 4 minutes and 30 seconds.
Evans Blue Injection and Brain Extraction
Evans blue extravasation has been used as a method of evaluating the integrity of BBB (282930). Evans blue was injected immediately after the last MR acquisition. Using the tail vein, 4 mL/kg of 2% Evans blue (Sigma-Aldrich, St. Louis, MO, USA) in normal saline was injected. A lethal dose of anesthesia was administered 10 hours after the Evans blue injection. The rat brain was transcardially perfused with 4% paraformaldehyde. After brain extraction, the specimen was cooled on ice and then cut into 2-mm coronal sections. The posterior surface of each section was photographed by a digital camera.
Analysis of MRI
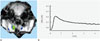
Permeability parameters were calculated by off-line PRIDE tools provided by Philips Medical Systems (Best, The Netherlands), which is based on the pharmacokinetic model of Tofts et al. (31). The two compartment model of Tofts assumes intravascular and extravascular extracellular spaces, which are divided by the BBB. The degree of contrast leakage from the intravascular space to the extravascular extracellular space is referred to as Ktrans. The volume fraction of the extravascular extracellular space is referred to as ve. The volume fraction of plasma space is referred to as vp. Those permeability parameters were calculated by means of iteration between time-intensity curves of the artery and tissue in assumption of the Tofts model (2731). Arterial input function was measured at the area of left internal carotid artery (Fig. 1A) and its time-concentration curve was checked (Fig. 1B). Because extravasation of Evans blue was prominent near the slices of Bregma-1.60 mm, they were targeted for analysis. Briefly, post-processing consisted of motion correction of pixels from dynamic images, T1-mapping using different flip angles (5° and 15°), co-registration of pixels on the T1-map, arterial input function estimation, and pharmacokinetic modeling. All these processes were automatically performed by PRIDE tools. Different regions of interest (ROIs) were placed in the cortex and basal ganglia in the ipsilateral and contralateral hemispheres of transient MCA occlusion. Therefore, four different ROIs were drawn per rat. Then, the three types of permeability parameters (Ktrans, ve, and vp) were calculated on each ROI.
Analysis of Specimen
The posterior surface of each section was photographed (Fig. 2A). Photographs of the posterior surface of Bregma-1.60 mm were loaded on Image J (32). The photography of the specimen was split into three color channels: red, green, and blue. Because red-channel images showed good contrast between the normal appearing brain and leakage of Evans blue, red-channel images were used for the analysis of optical density. Mean optical density was measured by ROIs in the ipsilateral cortex (Fig. 2B) and basal ganglia (Fig. 2C) along with contralateral cortex and basal ganglia. Optical density of the corpus callosum was used for normalization of those ROIs. Normalized optical densities were calculated with the following equation: (optical density of corpus callosum - optical density of ROI) / optical density of corpus callosum.
Statistical Analysis
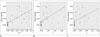
Optical density was taken as the dependent variable and permeability parameters were considered as the independent variables. Scatter plots were drawn between optical densities and permeability parameters of each ROI (n = 52) and fitted linear correlation lines were calculated for each permeability parameter. Pearson correlation analysis was performed. The correlation coefficient and the coefficient of determination were calculated. Durbin-Watson statistic was calculated to assess normality and independence of residuals. For the statistical analysis, we used the statistical software package, SPSS (version 20, SPSS Inc., Chicago, IL, USA). Statistical significance was set at p < 0.05.
RESULTS
Thirteen rats showed acute infarct in right basal ganglia or cortex on diffusion-weighted images. There were no cases showing hemorrhagic transformation on T2*-weighted gradient echo images. DCE-MRI showed an increase in permeability parameters in the ipsilateral hemisphere of the MCA occlusion (Fig. 3). There were no cases with a positive value of any permeability parameter in the contralateral normal-appearing hemisphere on DCE-MRI. All the permeability parameters showed a linear correlation with optical density (Table 1, Fig. 4). Among those permeability parameters, Ktrans showed the highest values of correlation coefficient and coefficient of determination (0.687 and 0.473 respectively, p < 0.001). Durbin-Watson statistics for analysis of residuals showed 2.072, which was suggestive of normality and independence of residuals.
DISCUSSION
Dynamic contrast-enhanced MRI is a method of quantification of BBB permeability. In this study, we successfully acquired DCE-MRI in a rat model and analyzed permeability parameters using the pharmacokinetic two compartment model of Tofts. Ktrans was consistent regarding the prediction of the later extravasation of Evans blue in this study. Previous research about permeability mainly focused on Ktrans, but this study also showed other permeability parameters (ve and vp) in terms of their correlation with the extravasation of Evans blue. Previous results in animal models were typically performed using 4.7-T, 7-T, or higher tesla animal-dedicated MR systems and coils (303334353637). In this study, we applied 3-T MRI and an 8-channel wrist coil to evaluate permeability in a rat stroke model. Compared with previous studies with higher tesla MRI, our permeability images were inferior in voxel size and temporal resolution. However, all DCE-MRI in our series were interpretable by means of the pharmacokinetic model of Tofts and correlated with later extravasation of Evans blue.
Our data showed that the measured permeability parameters were correlated with a later extravasation of Evans blue. The most correlative parameter among them was Ktrans. This result is consistent with those of previous studies, even though there was little difference in the methodology of analysis (3435). Increased Ktrans detected 3 hours after embolic infarct has been associated with progression in fibrin leakage (34). Permeability parameters were sensitive to the prediction of later hemorrhage as early as three hours after the embolic infarct and Ktrans was more sensitive than ve (35). We thought Ktrans showed highest correlation with Evans blue leakage because Ktrans is a targeted quantitative parameter of the BBB between the intravascular and extracellular spaces. However, our results also showed positive correlations between both ve and vp and the extravasation of Evans blue. Those two values are related to the concentration of extravasated gadolinium in extracellular and intravascular spaces respectively. Compared with neuro-oncologic DCE-MRI studies, those parameters have been rarely investigated in stroke research. Because our study cannot sufficiently explain about the extracelluar and intravascular spaces in a transient cerebral ischemic model, further research should be performed to examine correlations with cellular integrity (i.e., infarct core and penumbra), cerebral blood volume, and blood flow.
Permeability parameters are quantifiable data which can be candidates for imaging biomarkers in stroke treatment. Compared with histology-based methods, MRI-based methods are better for use in longitudinal studies. MRI enables the repeated scanning of a rat without sacrifice. Serial imaging throughout the entire experiment can eliminate inter-group variance, and therefore offer higher statistical power. Further research using DCE-MRI is necessary to provide information about BBB leakage which is related to post-ischemic edema, hemorrhagic transformation, and neurotoxicity. This can be potentially applied to the clinical management of stroke and the development of neuro-protective agents.
Our study has several limitations. We did not consider the status of reperfusion, which can be evaluated by MR angiography of perfusion-weighted MRI, in our evaluation of the permeability parameters. Status of reperfusion, timing of reperfusion, and status of collaterals might affect the result of permeability changes. In the case of failed reperfusion, the gadolinium bolus may not reach the leaky vessels. This might result in an underestimation of Ktrans. Secondly, Evans blue extravasation was considered to be a reference standard to assess altered vascular permeability. However, the extent and density of permeability measured by MRI was different because there were innate differences in tracer characteristics including molecular weight, electric charge, and protein binding between gadolinium and Evans blue. Thirdly, there was a 10-hour interval between the last MR examination time and brain extraction time. The time interval between the Evans blue injection and brain extraction was usually an hour or two in previous studies. However, some of the previous studies used longer time intervals, such as 24 hours (28). In our study, the permeability parameters from DCE-MRI could be predictive of Evans blue extravasation after 10 hours. Finally, we could not evaluate the permeability parameters for the prediction of later hemorrhage, because no case showed a later hemorrhagic transformation. This may be due to an insufficient BBB injury during the MCA occlusion periods or because there was no injection of thrombolytic agents.
In conclusion, permeability parameters (Ktrans, ve, and vp) obtained with DCE-MRI at 3-T are well-correlated with later Evans blue extravasation, which was evaluated in a rat transient cerebral ischemic model, and Ktrans shows the strongest correlation among the parameters measured.



 XML Download
XML Download