

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
A clinical prognosis is an estimate of the likely course and outcome of a disease. In general, the type, location, stage, and histologic grade of the tumor are the most important factors that predict the outcome of cancer patients. Among these factors, the prognosis of solid tumors is greatly affected by tumor stage. However, in patients with hepatocellular carcinoma (HCC), prognosis assessment is complicated due to the biological heterogeneity of the disease and the lack of consensus over the best classification system (1, 2). To assess the prognosis of HCC patients, it is recommended that the staging system take into consideration tumor stage, liver function, physical status and treatment efficacy (1, 3). Traditionally, TNM or Okuda classification is used for staging HCC despite some limitations (1, 3). The Barcelona-Clinic Liver Cancer staging system links staging with a specific treatment strategy and with an estimation of life expectancy (4). Currently, there is no agreement on a worldwide recommended staging system.
Biomarkers are especially useful in cancer patients in a number of ways, including measuring the progress of disease, establishing outcome, and evaluating recurrence. Biomarkers are measurable indicators of the severity or presence of some disease state and act as surrogate endpoints (5, 6, 7, 8). Four technological approaches can provide biomarkers such as body fluid, solid tissue samples, physiological measurements, and imaging (8). Among these, imaging biomarkers have the unique benefit in that they distinguish the exact disease focus. They are relatively non-invasive and repeatable. Imaging biomarkers can be classified in 4 ways: diagnostic, monitoring, predictive, and response biomarkers (8). Despite the advances in imaging biomarkers in the areas of diagnosis, monitoring, and response, there are only few predictive or prognostic imaging markers, especially in patients with HCC.
Until now it is widely accepted that tumor size, multifocality, and vascular invasion are the most important prognostic factors of HCC (9, 10, 11). These variables are incorporated into various staging systems, and imaging plays a major role in the assessment of these variables. Therefore, the established roles of imaging include not only screening and surveillance of at-risk patients, but also diagnosis, staging, and prognostication of HCC (12). For these purposes, magnetic resonance imaging (MRI) is advantageous because of its high soft tissue contrast, capacity for multiple parameters, and use of various contrast agents. Furthermore, in addition to the severity of liver disease and tumor characteristics, several other features related to survival have emerged from a large number of studies. Therefore, some magnetic resonance (MR) imaging features may have prognostic, as well as the diagnostic values (Table 1). In this review, we discuss the MRI features of HCC and their implications for prognosis.
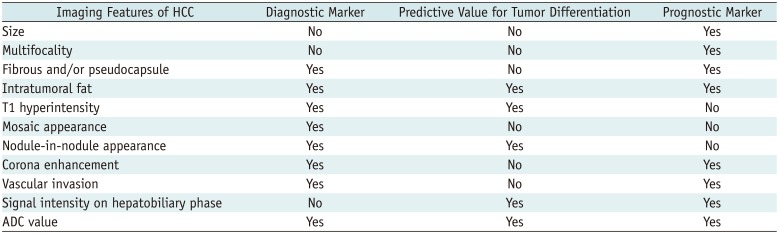
Table 1
Imaging Features of HCCs and Their Values
![]()
Go to : 
Size and Multifocality
The size and number of tumors, which together represent tumor burden, are important prognostic factors for HCC (9, 10); they are included in various radiological staging systems (13). As tumor size increases, HCCs tend to have a higher frequency of vascular invasion, extrahepatic metastasis and a decrease in patient survival. The availability and success of curative treatment options, such as liver resection or transplantation, depends heavily on the size and number of HCCs. Patients with one 2-5-cm HCC nodule or 2 to 3 HCC nodules measuring < 3 cm, who have no macrovascular invasion or extrahepatic metastases, have priority for transplantation (14). Liver resection for HCCs < 3 cm in size improves long-term patient survival (15). However, tumors > 3 cm have a higher incidence of microvascular invasion, especially in tumors of "nodular with extranodular growth" or "confluent multinodular type" (16, 17, 18). For patients with small HCCs, various treatment options are available, and a favorable prognosis is expected.
Small HCCs measuring < 2 cm consist of 2 distinct types: 1) small HCCs with indistinct margins, which are considered "early HCC" or "HCC of vaguely nodular type" and 2) small HCCs with distinct margins, which are considered "small and progressed HCC" or "HCC of distinctly nodular type" (19). Histologically, early HCCs consist of well-differentiated tumor cells (20) invading the fibrous tissue surrounding portal tracts, which is referred to as stromal invasion (21, 22). They grow by replacing the surrounding liver parenchyma unlike the progressed HCC (23, 24). As the early HCCs spread, they do not displace or destroy the surrounding vascular structures but replace the surrounding parenchyma presenting an indistinct margin (23, 24, 25). About 80% of small and progressed HCCs are moderately differentiated, and the other 20% are both well- and moderately-differentiated (20). Although "early HCC" has the least risk of microvascular invasion, "small and progressed HCC" is thought to exhibit vascular invasion and intrahepatic metastasis (26). Therefore, small HCCs of distinctly nodular type represent progressed cancer in spite of their small size. While HCCs of distinctly nodular type frequently show a typical enhancement pattern, HCCs of vaguely nodular type tend to show an atypical enhancement pattern such as a lack of arterial hyperenhancement or venous/delayed washout (27). Early HCCs frequently show hypo- or iso-enhancement on arterial-phase imaging, due to incomplete arterial neovascularization (28), and cannot be detected reliably using extracellular agents (29). However, because organic anion transporting peptide (OATP) 8 expression decreases before the sufficient arterial inflow during multistep hepatocarcinogenesis, early HCCs may appear hypointense in the hepatobiliary phase (30, 31), and some early HCCs are observed only in the hepatobiliary phase (32, 33).
More than one third of patients with HCC have multifocal hepatic nodules (34), which are defined as tumor nodules clearly separated by intervening non-neoplastic liver parenchyma (35). Multifocal tumors may represent either multiple independent HCCs arising simultaneously (multicentric HCC) or intrahepatic metastases from a primary HCC (36). Multicentric tumors may exhibit varying histological grade and other features, while all metastatic tumors of a single HCC are considered progressed lesions with advanced tumor grade. The prognosis of patients with intrahepatic metastasis from HCC tends to be worse than those with multicentric HCCs (37). Intrahepatic metastases develop by 2 different pathways. Small satellite nodules around the primary tumor are formed when tumor cells enter the portal venules that drain from the primary tumor and spread into the surrounding parenchyma (38, 39). Metastatic nodules outside the drainage area, including other segments or the contralateral lobe, develop via systemic circulation of tumor cells (40).
Go to :
Fibrous Capsule and/or Pseudocapsule
The presence of a fibrous capsule is one of the characteristic findings of nodular, progressed HCC (41), and is found in 24-90% of Asians and 12-42% of non-Asians with HCC (11). Since cirrhotic or dysplastic nodules (DNs) usually do not develop a fibrous capsule, the presence of a capsule is an important finding in HCC (23). Although some investigators have found that capsule appearance does not increase the diagnostic accuracy for HCC because it usually coincides with other hallmark imaging features, other investigators assert that capsule appearance is valuable, as it permits diagnosis of HCC without a definite washout appearance (14, 42). Capsule presence is regarded as a major diagnostic criterion for HCC, along with arterial hyperenhancement, according to the liver imaging reporting and data system (43), and Organ Procurement and Transplantation Network.
Histologically, the fibrous capsule consists of an inner layer rich in pure, fibrous tissue and an outer layer containing portal venules (or sinusoids) and newly formed bile ducts (41, 44). The fibrous capsule is a common pathological feature of progressed HCC, but not of early HCC, DNs, or regenerative nodules (23). The fibrous capsule shows a thin rim of hypointensity on T1-weighted images and a hypointense or hyperintense rim on T2-weighted images (Fig. 1). On dynamic MRI, the enhancing rim shown on portal venous or delayed phase images (45) are from the retention of the extracellular contrast agent within the prominent peritumoral sinusoids and/or fibrosis (45, 46). On hepatobiliary contrast agent-enhanced MRI, the relatively high enhancement of the background liver parenchyma may obscure capsular enhancement during the late dynamic or transitional phase. Some HCCs do not have a true fibrous capsule even though the MRI may show a hypointense rim on T1-weighted and T2-weighted imaging (45): an enhancing rim on delayed phase images can mimic the fibrous capsule. Such a false-positive fibrous capsule, i.e., a pseudocapsule, on MRI represents prominent histopathological hepatic sinusoids and/or peritumoral fibrosis (41, 45).
 | Fig. 155-year-old man with encapsulated progressed HCC.
A. T1-weighted three-dimensional gradient echo image with fat suppression (TR/TE/FA = 2.5 ms/1 ms/11°) in late hepatic arterial phase after administration of gadoxetic acid shows hyperenhancing mass with hyperemia of surrounding liver parenchyma (arrow) in segment 8. B. Mass is hypointense on transitional phase with thin capsule appearance (arrow). Note that relatively high enhancement of background parenchyma on transitional phase may obscure capsular enhancement and reduce confidence of reader. C. Fat-suppressed fast spin echo T2-weighted image shows slight hyperintensity and hypointense capsule (arrow). FA = flip angle, HCC = hepatocellular carcinoma, TE = echo time, TR = repetition time
|
Hepatocellular carcinoma with a fibrous capsule is considered a favorable prognostic factor, as it is associated with more effective transarterial chemoembolization (TACE) and lower recurrence rates after resection or ablation (47, 48, 49). This may be due to the barrier effect of the fibrous capsule that inhibits HCC dissemination (50). HCCs with a pseudocapsule may also confer a favorable prognosis because they exhibit similar behavior in terms of vascular invasion and tumor grade compared to a HCC with a true fibrous capsule (41, 45). It is important to note that encapsulated HCC does not have a better prognosis than early-stage or small HCC, because the presence of a capsule indicates progressed HCC (12, 51). In other words, HCCs with intact capsules have a better prognosis than HCCs of similar grade and size without capsules or with disrupted capsules (41, 45, 51).
Go to :
Intratumoral Fat in HCC
Hepatocellular carcinomas sometimes contain an internal fat component (11), which is reportedly found in up to 19.6% of HCCs on light microscopy and in up to 10% of HCCs on MRI (44, 52). In patients with cirrhosis, the presence of intralesional fat raises concern for malignancy or premalignant lesions (53). Since intralesional fat is very rare in hepatic malignancies except for HCC, the detection of fat may help to exclude intrahepatic cholangiocarcinoma (29). Despite potential benefits, the diagnostic value of intralesional fat has not yet been determined. Intralesional fat is shown to be noncontributory in radiological diagnosis of HCC, as the presence of fat coincides with other more discriminatory imaging features, such as arterial hyperenhancement or delayed washout (54, 55). Intralesional fat can be detected by identification of a signal drop on opposed-phase images, compared to in-phase, T1-weighted, chemical-shift gradient-recalled-echo MR images (Fig. 2) (43, 55, 56, 57).
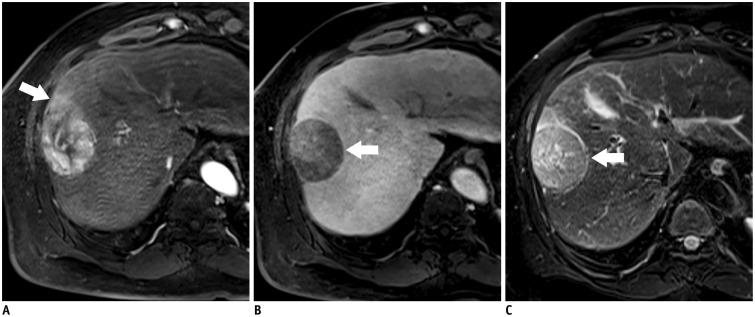
 | Fig. 276-year-old man with fat-containing HCC.
A, B. Axial dual-echo gradient echo images (TR/TE = 4/1.2 ms, in-phase; 2.4 ms, opposed-phase) show mass in dome of liver. Signal loss (arrow) of mass on opposed-phase (B) compared to in-phase (A) indicates intralesional fat. Presence of intralesional fat permits confident diagnosis of HCC. HCC = hepatocellular carcinoma, TE = echo time, TR = repetition time
|
Intralesional fatty change or fatty metamorphosis occasionally occurs during hepatocarcinogenesis (53), and diffuse fatty metamorphosis is considered as one of the characteristics of early-stage HCC (52). Fatty change is most frequently found in HCCs with a diameter of approximately 1.5 cm, and the prevalence decreases incrementally with tumor size and histologic grade. This feature is uncommon in HCCs > 3 cm in diameter and/or in moderately differentiated HCCs (25). Approximately 6% of moderately differentiated HCCs reportedly have fatty change, while no poorly differentiated HCCs exhibit this feature (52). In early-stage HCCs, the blood source gradually shifts from the vessels of the portal tracts to the newly formed non-triadal arteries. At this transitional stage, the lack of blood supply and increased cellular density may cause transient hypoxia, which may lead to intratumoral fatty metamorphosis (19, 52). However, the molecular mechanism of fatty metamorphosis by hypoxia in HCCs is not fully understood.
Patients with fat-containing HCC may have a better clinical outcome than patients without fat-containing HCCs due to longer time to tumor progression and decreased risk of metastasis. This may be due to the fact that intralesional fat is characteristic of early and well-differentiated HCC, not of progressed HCC (58). The prognosis of progressed HCC with intralesional fat has not been established.
Go to :
T1 Hyperintensity
Hepatocellular carcinomas may have variable signal intensity on T1-weighted images. Although most hepatic lesions are hypointense relative to liver parenchyma on T1-weighted images, some HCCs show T1 hyperintensity (59, 60, 61, 62). T1 hyperintensity can be attributed to the presence of T1 shortening substances such as fat, copper, highly-concentrated proteins, glycogen and hemorrhages within the nodules (63).
Hepatocellular carcinomas are more commonly hypointense on T1-weighted images. In a previous report, T1 signal intensity of HCCs was hypointense in 65% of cases, isointense in 23%, and hyperintense in 12% (64). Unenhanced T1-weighted imaging plays a minor role in the diagnosis of HCC because HCCs and non-malignant hepatic lesions have various and overlapping T1 signal intensity (65, 66). However, the signal intensity on T1-weighted images may be associated with histologic grade and clinical outcome (59, 61). It has been previously reported that 64-66% of HCCs of Edmondson-Steiner grade I or with well-differentiated histology show hyperintensity on T1-weighted imaging (Fig. 3) (59, 61). However, the proportion of HCC nodules with hyperintensity on T1-weighted imaging gradually decreases as the histological differentiation grade progresses (61). Therefore, HCCs with T1 hyperintensity tend to have better tumor histologic grade, while HCCs with T1 hypointensity tend to be more poorly differentiated (59, 61). Besides, T1 hyperintense HCCs without T2 hyperintensity or arterial hypervascularity usually follow a benign clinical course (67).
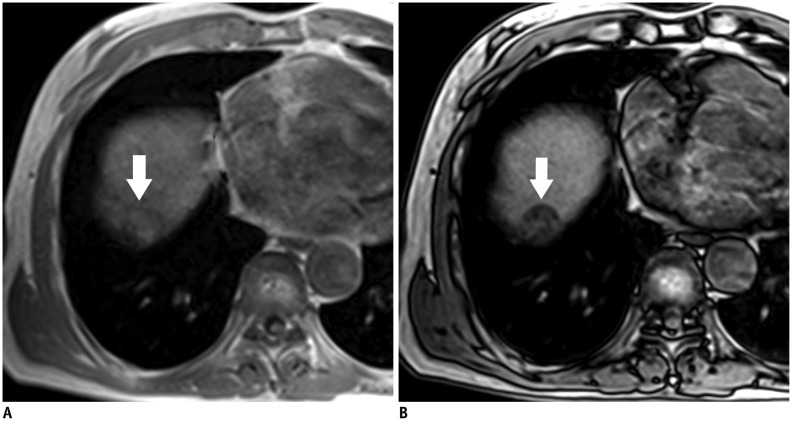
 | Fig. 371-year-old man with HCC showing T1 hyperintensity.
A. Unenhanced fat-saturated T1-weighted three-dimensional gradient echo image with fat suppression (TR/TE/FA = 2.5 ms/0.9 ms/11°) shows hyperintense mass (arrow) in segment 4. B. Mass is barely visible on fat-suppressed fast spin echo T2-weighted imaging due to isointense signal (arrow). FA = flip angle, HCC = hepatocellular carcinoma, TE = echo time, TR = repetition time
|
Go to :
Nodule-in-Nodule Appearance
Nodule-in-nodule appearance represents the presence of a small nodule within a larger nodule (43). This imaging appearance corresponds to the nodule-in-nodule growth pattern on histology (68) and suggests a focus of progressed HCC within a well-differentiated HCC or DN (19). Histologically, the inner nodule is composed of less differentiated cancer tissue, containing less fat and/or iron, while the parent nodule is a well-differentiated HCC or DN rich in fat and/or iron (69, 70). When less-differentiated cancerous tissues within the well-differentiated nodules proliferate in an expansive fashion, a 'nodule-in-nodule' appearance is frequently seen. Thus, a nodule-in-nodule appearance could be interpreted as a morphologic marker of the progression of dedifferentiation of the tumor (19, 68).
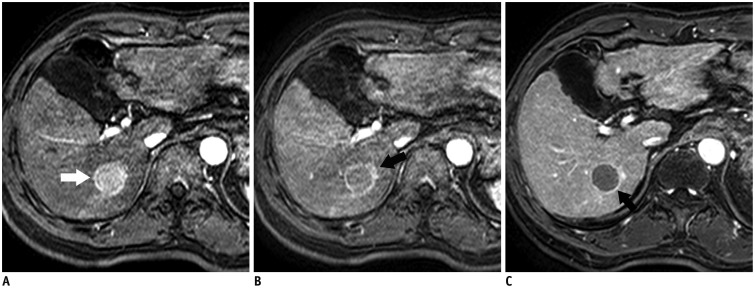
The inner nodule, corresponding to a developing and distinctly nodular-type HCC, shows T2 hyperintensity, T1 hypointensity, and arterial enhancement on dynamic imaging (Fig. 4) (28, 71). On the other hand, the preexisting parent nodule, corresponding to either a DN or early HCC tissue, demonstrates T2 hypointensity, T1 hyperintensity, and hypovascularity on dynamic imaging (11, 72, 73). The inner HCC nodule has radiological and pathologic features typical of progressed HCC with the potential for rapid growth and doubling time (74). However, consideration of the nodule-in-nodule appearance of HCC as a prognostic factor is not established (29).
 | Fig. 456-year-old man with HCC showing nodule-in-nodule appearance.
A. Pre-contrast T1-weighted three-dimensional GRE image shows hypointense inner nodules within hyperintense outer nodule, consistent with nodule-in-nodule architecture. B. Subtracted arterial phase image shows hyper-enhancement of inner nodules (arrows). C. Inner nodules (arrows) exhibit hyperintensity relative to outer nodule and surrounding liver on fat-suppressed fast spin echo T2-weighted image. Outer nodule is hypointense. GRE = gradient echo, HCC = hepatocellular carcinoma
|
Go to :
Corona Enhancement
Corona enhancement, one of the characteristics of hypervascular HCC, is described as a transient zone or rim of enhancement around a hypervascular HCC in the late arterial phase seen in either CT hepatic arteriography (75) or multiarterial phase dynamic MRI (Fig. 5) (63, 76). Since corona enhancement is a very unusual finding other than HCC, it is one of the most reliable features for distinguishing HCC from other hypervascular tumors or pseudolesions such as arterioportal shunts (77). Because corona enhancement is transient, it is hard to recognize on routine CT or MRI. Corona enhancement is seen only in the perfusion phase of dynamic study, such as the arterial or early portal venous phases and not the equilibrium phase (76). This is different from capsular enhancement, which is mainly seen as an enhancing rim in the delayed phase images (76).
 | Fig. 566-year-old man with HCC showing corona enhancement.
A, B. T1-weighted three-dimensional GRE image with fat suppression (TR/TE/FA = 4.5 ms/2.1 ms/15°) in (A) early and (B) late hepatic arterial phase after administration of gadolinium-based contrast agent shows hyper-enhancing mass (arrow) in segment 6. Notice irregular circumferential enhancement (arrow) in liver parenchyma around mass in late hepatic arterial phase. C. Enhancement of perilesional parenchyma fades in portal venous phase. Transient enhancement of perilesional parenchyma is known as corona enhancement. Note capsular appearance of mass (arrow). FA = flip angle, GRE = gradient echo, HCC = hepatocellular carcinoma, TE = echo time, TR = repetition time
|
In addition to the ancillary imaging features, the importance of corona enhancement is related to blood drainage in HCC. The drainage vessels of HCC change during multistep carcinogenesis (78). As the tumor cells proliferate more rapidly, they first invade the intranodular hepatic veins; however, tumor blood drainage via intranodular and perinodular hepatic veins disappears early, as perinodular hepatic veins are collapsed by tumor compression. Then, venous blood from tumors begins to drain into surrounding hepatic sinusoids and portal veins (75, 78). In HCCs with a fibrous capsule, perinodular hepatic sinusoids collapse, and the fibrous capsule interrupts the connection between intranodular and extranodular sinusoids. Consequently, tumor venous blood drains into the surrounding liver parenchyma via portal venules within the capsule, which can be seen as thick corona enhancement on imaging (40, 75, 78). Thus, corona enhancement may provide prognostic information. Local recurrence is frequently observed at the area of corona enhancement, as this corresponds to the initial drainage pathway of the tumor (40). The area of corona enhancement is the first site of intrahepatic metastasis of HCC, and daughter nodules are commonly found in this area. Therefore, resection or ablation of tumors should include the regions of corona enhancement to avoid tumor recurrence (40).
Go to :
Vascular Invasion by HCC
Vascular invasion is more common in HCCs that are larger or of higher histologic grade (38, 79, 80, 81, 82, 83). Tumor cells more frequently involve the portal venous system than hepatic veins (64, 82, 84). Vascular invasion is divided into macro- and microvascular invasion, depending on the level of involved vascular structures (14). Both types of vascular invasion are related to poor prognosis because they provide the route for tumor cells to access the portal or systemic circulation, which can result in intrahepatic or systemic metastases. Thus, HCCs with vascular invasion have frequent multifocality and a higher recurrence rate after hepatic resection, ablation therapy, or liver transplantation (85, 86). Therefore, surgical resection or liver transplantation is usually contraindicated in HCCs with macrovascular invasion (87).
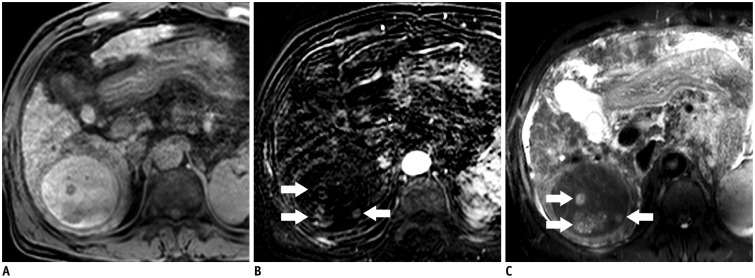
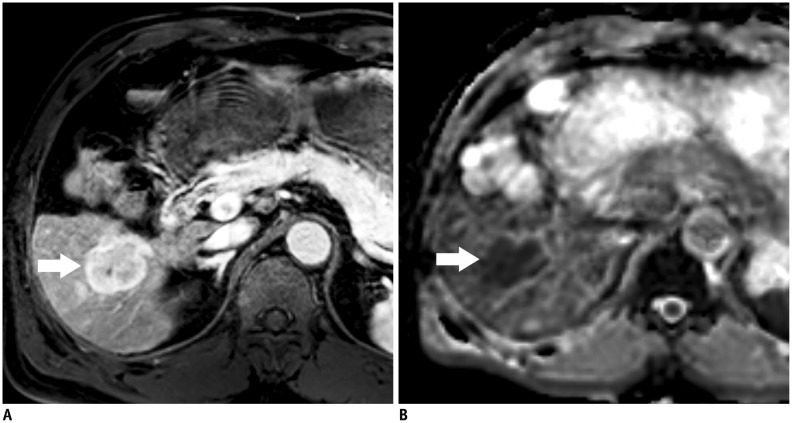
It is difficult to preoperatively predict microvascular invasion with imaging studies as it occurs at a microscopic level (88). Microvascular invasion of HCC is reportedly not predictable using morphologic and enhancement features of MRI, such as T1 and T2 signal intensity, margins, presence of capsule or pseudocapsule, wedge-shaped peritumoral enhancement, or quantitative tumor enhancement (18, 76). However, several tumor characteristics on MRI have been suggested as markers for risk of microvascular invasion. Morphologically, tumors with more than 3 foci and a tumor size > 3 cm exhibiting gross patterns of "nodular with extranodular growth", "confluent multinodular type", or "infiltrative type" are reported to be closely related to microvascular invasion (16, 17, 18). Therefore, multiple tumors or tumors > 3 cm with non-smooth margins on MRI are likely to have microvascular invasion. Additionally, HCCs of < 2 cm, especially those of distinct nodular type, may exhibit microvascular invasion (32). These tumors usually show a typical dynamic enhancement pattern and hyperintensity on T2-weighted and diffusion-weighted images (32). Some studies have suggested that large or irregular and distorted corona enhancement in HCC may predict microvascular invasion (76, 89, 90, 91). However, this finding is not been validated by other studies. Peritumoral hypointensity and non-smooth tumor margins on the hepatobiliary phase of gadoxetic acid-enhanced MRI may also be indicative factors of microvascular invasion (Fig. 6) (17, 91). In areas of peritumoral hypointensity of the liver parenchyma, expression of OATPs and canalicular transporter multidrug resistance-associated protein 2 receptors decrease, probably because of hemodynamic alteration related to tumor obstruction of minute portal veins (17). The tumor margin may be non-smooth if the tumor is infiltrative or with a minute budding portion at its periphery (91).
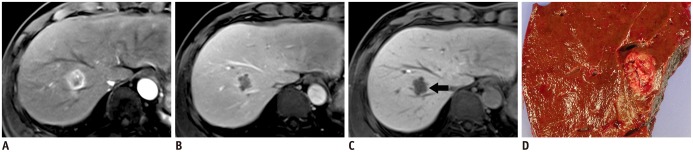 | Fig. 651-year-old man with HCC and microvascular invasion.
A. Gadoxetic acid-enhanced T1-weighted three-dimensional GRE sequence (TR/TE/FA = 3.4 ms/1.7 ms/15°) acquired in late hepatic arterial phase shows heterogeneous mass at segment 8 of liver. B. Transitional phase image at three minutes depicts hypointense mass. C. Margin of mass is non-smooth or lobulated on hepatobiliary phase imaging acquired 20 minutes after injection (arrow). D. Gross pathology photograph of resected specimen reveals confluent, multinodular type HCC. Histopathologic examination proves frequent microvascular invasion. FA = flip angle, GRE = gradient echo, HCC = hepatocellular carcinoma, TE = echo time, TR = repetition time
|
Go to :
Organic Anion Transporter Polypeptide Expression and Signal Intensity on Hepatobiliary Phase Imaging
Gadoxetic acid and gadobenate dimeglumine are 2 hepatobiliary contrast agents, currently available in clinical practice (12). They behave like extracellular agents after injection, are taken up by functioning hepatocytes and excreted into the biliary system. OATP 8 (also known as OATP1B1/3) is thought to be responsible for uptake of hepatobiliary contrast agents by hepatocytes (92, 93). Thus, nodules with low or no OATP expression do not take up hepatobiliary agents and appear hypointense in the hepatobiliary phase, while nodules with preserved or elevated OATP 8 expression take up the agents and tend to be isointense or hyperintense.
The expression of these transporters decreases during hepatocarcinogenesis. Expression levels are high in regenerating nodules and low-grade DNs and are lower in many high-grade DNs, early HCCs, and progressed HCCs (92, 94). On the hepatobiliary phase of gadoxetic acid-enhanced MRI, HCCs are usually hypointense from the lack of gadoxetic acid uptake due to down regulation of OATP 8 expression (95, 96). Studies have shown that the degree of tumor enhancement in the hepatobiliary phase after injection of gadoxetic acid inversely correlates with histologic grades (92, 97). Poorly-differentiated tumors tend to show lower signal intensity, as compared to well-differentiated or moderately-differentiated ones. Inverse correlation has been associated to the gradual decline in OATP expression seen during hepatocarcinogenesis (92, 94). This suggests that quantitative analysis of tumor enhancement in the hepatobiliary phase may predict histologic and prognostic features (92). However, other researchers show that the degree of tumor enhancement does not correspond with tumor grades (95, 98) or only correlates in a subset of patients with preserved liver function (99).
Some HCCs show hyperintensity on hepatobiliary phase due to increased uptake of hepatobiliary contrast media (Fig. 7) (100, 101, 102, 103). The overexpression of OATP 8 in some HCCs may be due to genomic alteration during hepatocarcinogenesis (92). The prevalence of these hyperintense HCCs on hepatobiliary phase varies from 5 to 12% (100, 101, 102). Most patients have well- or moderately-differentiated tumors, but poor differentiation is observed rarely (92, 95, 97, 100, 102, 103). Thus, the hyperintensity of HCCs on hepatobiliary phase may not be dependent on histologic differentiation of the tumor, but rather on the degree of OATP 8 expression or other potential genomic alterations (94, 97, 104).
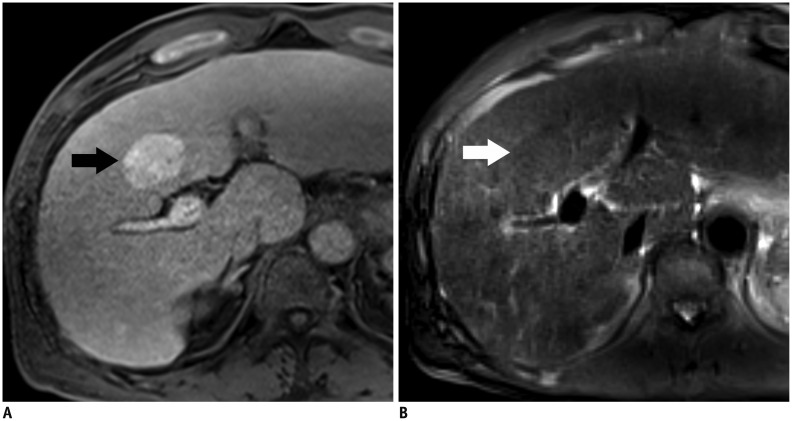
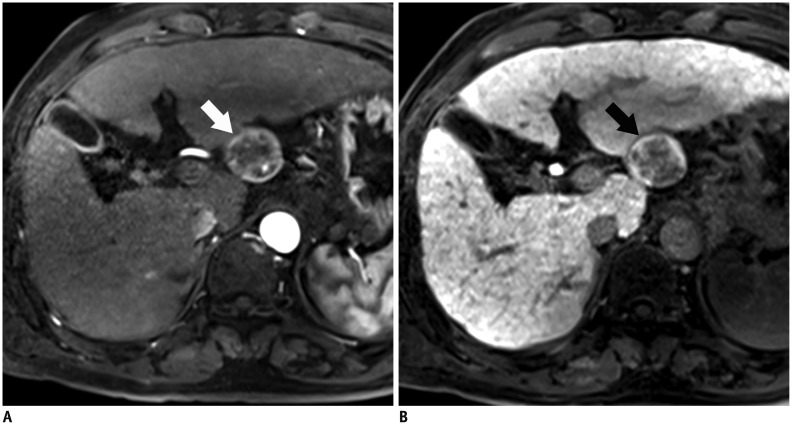 | Fig. 764-year-old man with HCC showing hyperintensity in hepatobiliary phase.
A. Gadoxetic acid-enhanced T1-weighted three-dimensional GRE image (TR/TE/FA = 3.4 ms/1.7 ms/15°) in late arterial phase shows exophytic, hyperenhancing mass (arrow) in left posterior liver. B. In hepatobiliary phase, mass is hyperintense with central hypointense areas (arrow). FA = flip angle, GRE = gradient echo, HCC = hepatocellular carcinoma, TE = echo time, TR = repetition time
|
Hyperintense HCCs on hepatobiliary phase may indicate a favorable clinical outcome in patients (95) since these tumors have infrequent microvascular invasion and have a longer interval of recurrence, as compared with hypointense HCCs (95, 102, 104, 105). Moreover, hyperintense HCCs most commonly appear as expanding gross-type, not infiltrative or diffuse-type, which are prone to poor prognosis (95). Patients with iso- to hyperintense HCCs on hepatobiliary phase tend to have lower levels of prognostic serum tumor markers (a-fetoprotein, protein induced by vitamin K absence or antagonist-II [PIVKA-II]) (104, 106, 107). Hyperintense HCCs on hepatobiliary phase are more common in older patients, suggesting that they grow more slowly (95, 98, 100, 103).
Go to :
Correlation of MR Imaging and Immunohistochemical Markers
Prognosis is not easy to determine in patients with HCC due to the heterogeneous nature of the tumors and the lack of appropriate biomarkers. Despite the advancement of molecular medicine, there are no well-established biomarkers to predict prognosis of HCC. Currently used tumor markers in HCC, such as alpha-fetoprotein or PIVKA-II, have limited sensitivity and specificity; however, some immunohistochemical markers have the potential to be used for prognosis and treatment stratification.
Hepatocellular carcinomas with biliary phenotypic markers such keratin 7 and keratin 19 (K19) may be more aggressive and have a worse prognosis (108, 109). Some HCCs expressing progenitor cell markers, such as epithelial cell adhesion molecule (EpCAM) and K19 have aggressive clinical outcomes due to a higher recurrence rate after resection or liver transplantation, resistance to chemoradiation therapy, and a higher rate of metastases (24, 108, 109, 110, 111, 112, 113, 114, 115, 116, 117). It is reported that HCCs expressing EpCAM or K19 show different radiologic features on MRI, as compared with HCCs lacking these markers (Fig. 8) (110). Gross multinodular confluent- or infiltrative-type tumors that are associated with an unfavorable prognosis are more common (110). A progressive or persistent enhancement pattern on dynamic study, similar to the enhancement pattern of cholangiocarcinoma, is more frequently seen in HCCs expressing progenitor cell markers (110). On gadoxetic acid-enhanced MRI, K19 expression is inversely correlated with tumor enhancement of HCC on hepatobiliary phase. Therefore, tumor enhancement on hepatobiliary phase is lower in K19-positive HCCs than in K19-negative HCCs (110, 118).
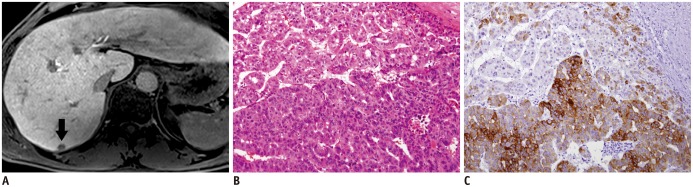 | Fig. 851-year-old man with HCC.
A. Hepatobiliary phase image acquired 20 minutes after injection shows hypointense nodule in segment 7 of liver (arrow). B. Nuclear grade III trabecular and pseudoglandular HCC with hepatic cells was confirmed (hematoxylin and eosin staining, × 100). C. Immunoreactivity of keratin 19 was strongly positive (× 100). Cell density ratio was 2.1. HCC = hepatocellular carcinoma
|
Go to :
Diffusion-Weighted Imaging
One of the characteristic radiologic features of many malignant tumors is elevated signal intensity on diffusion-weighted imaging, caused by a reduced apparent diffusion coefficient (ADC) of water in the tumor microenvironment (Fig. 9) (119). The mechanism of reduced ADC is not completely understood, but may reflect greater diffusion hindrance and reduced mobility of water molecules due to decreased extracellular space and increased tortuosity of the extracellular space matrix (120, 121, 122, 123). Most but not all (124) studies show that the addition of diffusion-weighted imaging to MRI improves the detection of HCC (125, 126, 127) and intrahepatic HCC metastases (128). The ADC value may provide information on tumor behavior. Since cellularity and the nuclear-to-cytoplasmic (N/C) ratio are major features used to determine histologic grading, high-grade tumors have densely-packed cells and a high N/C ratio in general. Densely-packed tumor cells can inhibit effective motion of water molecules and can restrict diffusion. Thus, the ADC value and the appearance on diffusion-weighted imaging likely reflect tumor cellularity and microenvironment.
 | Fig. 963-year-old man with HCC showing restricted diffusion.
A. Gadoxetic acid-enhanced T1-weighted three-dimensional GRE sequence (TR/TE/FA = 3.4 ms/1.7 ms/15°) in late arterial phase shows hyperenhancing mass (arrow) in right lobe of liver. B. Apparent diffusion coefficient map shows hypointensity (arrow) suggesting restricted diffusion. Restricted diffusion is highly suggestive of malignancy, but is not specific for HCC. FA = flip angle, GRE = gradient echo, HCC = hepatocellular carcinoma, TE = echo time, TR = repetition time
|
Some studies suggest that measuring the ADC value can predict tumor histopathologic grade (129, 130, 131, 132, 133), microvascular invasion (88), the presence of progenitor cell markers (110), and early recurrence after resection (132). However, these correlations are not always consistent, and some studies show no significant correlation between ADC and histopathologic grade of HCCs due to the large overlap of ADC among different histopathologic grades (134). Because the ADC value and diffusion-weighted signal intensity ratios particularly depend on techniques, magnetic field strength, and MRI scanners, diffusion-weight-based prediction thresholds may not yet be generalized.
Diffusion-weighted imaging is used to monitor efficacy of treatment using TACE and target therapy (135, 136, 137, 138, 139, 140). Some studies report that the ADC value of HCCs increase after TACE (136, 137, 138), and a high baseline ADC value could predict poor response to TACE (135, 140). In HCCs treated with an antiangiogenic agent (sorafenib), the ADC value may temporarily decrease in the early phase of treatment and increase again in long-term follow-up (> 3 months) (139). However, ADC values vary widely and may not contribute to the accurate diagnosis of tumor necrosis by any cut-off levels. Increased ADC may be caused not only by tumor necrosis, but also by perilesional inflammation and arterial reperfusion after TACE (141).
Go to :
CONCLUSION
MRI can not only be used for non-invasive diagnosis and staging, but also for predicting tumor biology as an imaging biomarker in patients with HCC. Favorable findings of HCCs on MRI include small size, presence of fibrous capsule/pseudocapsule, intralesional fat, high ADC value, and smooth margins or hyperintensity on hepatobiliary phase images, while unfavorable findings of HCCs include large size, multifocality, low ADC value, non-smooth margins or hypointensity on hepatobiliary phase images.
Go to :
 XML Download
XML Download