

 PDF
PDF ePub
ePub Citation
Citation Print
Print


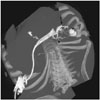
A 25-year-old man presented to the emergency department with a history of corrosive (turpentine) ingestion. Clinically, the patient had metabolic acidosis and his total white cell count was 28600/mm3. Computed tomography (CT) scan of the thorax and abdomen revealed diffuse thickening of the esophagus, stomach and duodenum. Minimal free fluid was present in the abdomen. The patient was first stabilised and step wise reconstruction of the gastro-intestinal tract was performed after esophagectomy, gastrectomy, pancreaticoduodenectomy, cholecystectomy, choledocho-jejenostomy and creation of a feeding jejenostomy. During the post-op period (around two months after the initial presentation), the patient had leakage of pancreatic secretions through the drain. CT of the abdomen was performed and dilute non-ionic iodinated contrast was injected through the surgical drain tube, which revealed opacification of the pancreatic duct and a tract with opacification of the splenic flexure in the colon (Figs. 1,2,3), compatible with a pancreatico-colonic fistula (PCF). The patient later underwent laparotomy again, and distal pancreatectomy and hemicolectomy were performed.
Pancreatico-colonic fistula is an uncommon complication of acute severe pancreatitis. It can occur either during pancreatitis or after pancreatic debridement (1). The diagnosis of fistula should be considered when there is recurrent sepsis, diarrhea or hemorrhage during follow-up of acute pancreatitis (2). Various imaging modalities such as endoscopic retrograde cholangio-pancreaticography (ERCP), barium enema and CT with rectal contrast can be used to demonstrate the fistula (2, 3). ERCP is the modality of choice for demonstrating PCF and it can also aid in management, especially for the placement of stents, which can be performed in the same sitting (1). Barium enema is a less sensitive modality. Shim et al. (3) reported a case of pancreatico-peritoneal fistula demonstrated by ERCP which was subsequently followed by a CT scan to provide a 3-dimensional display. CT with rectal contrast is a reliable modality for the demonstration and follow-up of PCF (1). PCF may be demonstrated by injecting contrast through the drainage tube when there is communication between the collection, pancreatic duct and colon, as in our case. PCF is usually managed by surgery or endoscopy-guided interventions and the reported mortality in cases of pancreatitis with fistula or colonic necrosis is 17-67% (4, 5). However, there are a few reports of pseudocysto-colonic fistulae that were managed conservatively (5). In our case, the necrosis of the tissues and development of fistulae were due to the delayed effect of corrosive injury and surgery. This case highlights the utility of CT in the demonstration of PCF in patients with recent surgery.


 XML Download
XML Download