

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Imaging plays an important role in the evaluation of thyroid diseases in pediatric patients. Scintigraphy and ultrasonography (US) are the primary modalities used for thyroid screening and evaluating congenital hypothyroidism (CH) (1, 2, 3, 4). US and scintigraphy are complementary, as US provides anatomical information and scintigraphy provides functional information. In pediatric patients, US is a first-line diagnostic test for detecting thyroid abnormalities and lymphadenopathy. In addition, US can be used to guide aspiration of detected nodules.
Normal Thyroid Gland Development
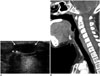
The thyroid gland develops from the median and paired lateral anlages. Thyroid follicular cells originate as the median thyroid anlage, an endodermal thickening between the first and second pharyngeal arches during the fourth to fifth gestational week. A thickening rapidly forms a small out-pouch referred to as thyroid primordium (5, 6). This structure elongates into a bilobate diverticulum and descends caudally while maintaining contact with the aortic primordium. A small channel; i.e., the thyroglossal duct, temporarily manifests as a connection between the tongue and the caudal migration of the thyroid primordium, which then involutes. The thyroid primordium first courses anteriorly to the primordial hyoid bone and laryngeal cartilage, and then loops inferiorly and posteriorly to the hyoid bone before continuing its descent into the infrahyoid portion of the neck (5, 6). By the seventh week, the gland attains its normal final position anterior to the second and third tracheal rings (Fig. 1). Arrest of descent can occur anywhere from the tongue down to the lower neck. The thyroglossal duct has usually degenerated and disappeared at the time of descent by week 7. The proximal opening of the thyroglossal duct persists as a small pit in the tongue (i.e., the foramen cecum). Parafollicular cells originate as lateral thyroid anlages, also known as ultimobranchial bodies, which arise laterally at the fourth and fifth pharyngeal pouches around the gestational week 5. The lateral anlages merge with products of the median anlage after descent into the infrahyoid portion of the neck, resulting in parafollicular cells interspersed throughout the thyroid gland (5, 6).
Congenital Hypothyroidism
Prevalence and Causes
Congenital hypothyroidism is a relatively common endocrine disorder that occurs in about 1 in 3981 live births in Korea (7). Neonatal screening started in 1985 in Korea. Most CH cases (75-80%) are caused by developmental defects known as thyroid dysgenesis. Dyshormonogenesis, which results from defective thyroxine (T4) synthesis, is caused by various autosomal recessive mutations (15-20%) (1, 2, 7). Thyroid dysgenesis is typically sporadic with a female predominance (1, 2) and there appears to be a wide range of molecular heterogeneity (1, 2, 3, 4). Among them, the thyroid-stimulating hormone receptor (TSHR) and thyroid peroxidase (TPO) genes account for the majority of mutation-positive cases of dysgenesis and dyshormonogenesis, respectively (8, 9). Scintigraphy reveals TSHR mutations in patients with decreased 99mTC-pertechnetate uptake and TPO mutations in those with increased uptake. TPO mutations are observed exclusively in patients with normal to enlarged thyroid glands. These organizational defects cause goitrous CH. Hypothyroidism resulting from dyshormonogenesis may cause neoplastic transformation if TSH levels are high for a prolonged period as a result of inappropriate levothyroxine treatment (4).
Diagnostic Imaging
Ultrasonography and scintigraphy can differentiate various types of CH. Aplasia is defined as the failure to detect thyroid tissue on US and scintigraphy (Fig. 2). If the thyroid gland is not visible in the normal position, an attempt is made to find the ectopic thyroid by examining the thyroid migration pathway along the course of the thyroglossal duct (1, 2). Ectopic thyroid tissue can be found anywhere along the migration course of the thyroid primordium (Fig. 3); however, in most (90%) cases, it is located at the base of the tongue (6). The lingual thyroid is the only functioning thyroid tissue in approximately 75% of these patients. Appearance varies on US, but the tissue is generally located close to the hyoid bone. An ectopic gland appears as a round or oval area of uptake in the midline of the upper neck on scintigraphy (Fig. 3B). Scintigraphy is more sensitive than US for detecting an ectopic thyroid. The thyroid gland appears normal on US in patients with hypoplasia; however, scintigraphy reveals decreased isotope uptake. Transient CH is diagnosed by normal thyroid function, thyrotropin-releasing hormone studies, and scintigraphy performed during trial-off therapy. Trial-off therapy is conducted at 1-3 years for all children with suspected CH, except those with aplasia, to determine whether treatment remains necessary (Fig. 4). The percentage of transient CH cases is estimated to be 13-38% in the US (10, 11, 12). Thyroid hemiaplasia is generally discovered incidentally (Fig. 5), and thyroid function in children with thyroid hemiaplasia may decrease during puberty when the need for thyroid hormones is higher. Dyshormonogenesis involves an inborn error in thyroxine synthesis (1, 2). The most common defect is TPO deficiency, which results in the failure to oxidize iodide to iodine. Iodide becomes trapped in the thyroid gland and cannot be organified. US reveals an enlarged, orthotropic thyroid as a result of increased TSH level, and the lobes develop a convex appearance laterally (1, 2, 3, 4). The isthmus is readily visualized in contrast to a normal gland. Scintigraphy reveals an enlarged gland in the normal location with increased isotope uptake (Fig. 6). Thyroid gland size in a child varies with age and is correlated with height, weight, body surface area, and age (13, 14, 15, 16, 17). Enlargement of the thyroid gland can be visually assessed by anterior convexity instead of normal concavity, increased thickness of the isthmus, or tracheal narrowing.
The most common pitfall of isotope scanning is lack of uptake despite the presence of thyroid tissue, leading to the spurious diagnosis of aplasia. This phenomenon may occur for several reasons: when the scan is delayed beyond 4-5 days of T4 treatment; thus, TSH suppression has occurred by the time the scan is performed; from iodine exposure; from blocking TSHR antibodies causing transient hypothyroidism; and rarely, from defects affecting iodide uptake; e.g., sodium-iodide symporter gene mutations. The diagnosis of spurious thyroid absence will not be made if concurrent US is carried out (1, 2). Chang et al. (3) reported that 14% of pediatric patients with CH who had no uptake during scintigraphy had a thyroid gland in the appropriate location on US. Detecting the thyroid gland in the normal position provides greater diagnostic power to identify the etiology, decide when treatment should be discontinued, and determine the prognosis.
Thyroglossal Duct Cyst
If the thyroglossal duct does not involute completely, the remnant may manifest as a thyroglossal duct cyst (TGDC), which accounts for approximately 70% of congenital abnormalities in the neck (6, 18). Eighty-five percent of TGDCs are located below the level of the hyoid bone and typically present as midline cystic masses. Anechoic or hypoechoic masses appear as well-circumscribed cysts deep or embedded in the strap muscle on US scans (Fig. 7). Acute infection, chronic inflammation, or hemorrhage may also occur. A ruptured cyst may result in a thyroglossal duct sinus that opens through the overlying skin. A localized mass appearing in a portion of the cyst wall suggests the possibility of a malignancy, whereas invasion of the
adjacent soft tissue with no history of infection strongly suggests the presence of a neoplasm in the cyst (18).
Thyroid Nodules
Detecting thyroid nodules has become more frequent with the widespread use of US. US is the mainstay for detecting and making the differential diagnosis of thyroid nodules and for providing biopsy guidance.
The incidence of thyroid nodules in children and adolescents is estimated to be between 1% and 18% (19, 20). Avula et al. (20) reported that a 1-year increase in age in children increases the risk of incidental thyroid abnormalities by 9%. The risk of malignant thyroid nodules in children ranges from 14% to 40%, which is considerably higher than that of adults (9-15%) (20, 21).
Ultrasonography findings for thyroid nodules are classified into one of three categories: probably benign, indeterminate, or suspicious malignant. Solid thyroid nodules with one or more US malignancy features (i.e., spiculated or microlobulated margin, markedly hypoechogenic, taller-than-wide shape, or calcification) are considered malignant, and thyroid nodules with one or two benign US features (i.e., complete cyst, predominantly a cystic lesion, cystic lesion with a comet-tail artifact, or spongiform benign cystic lesion) are considered probably benign (Fig. 8), based on the "Guidelines for Thyroid US" provided by the Korean Society of Thyroid Radiology (22). A nodule that does not show benign or malignant features is considered to be an indeterminate nodule. US findings are summarized in Table 1.
Benign Thyroid Nodules
The majority (67.3%) of incidentally detected thyroid lesions in children are cysts (20). True epithelial-lined thyroid cysts are rare. Most cystic thyroid lesions are hyperplastic nodules that have undergone extensive degeneration. Colloid cysts may contain bright echogenic foci with comet-tail artifacts caused by the presence of microcrystals (Fig. 9) (23, 24).
An intrathyroid thymus has been reported in 17.3% of incidentally detected thyroid nodules (20). The thymus originates from the third pair of branchial pouches with a rudimentary portion arising from the fourth pair and descends to the superior mediastinum. Migration anomalies can produce an ectopic thymus that rests along the path of descent (18, 25). These lesions have US findings similar to a normal thymus and are more common in males than females, in contrast to the higher incidence of incidental thyroid lesions in adult females (Fig. 10).
Thyroid Malignancy
Malignancies include papillary, follicular, and medullary carcinomas, and a papillary carcinoma is the most common (80%). Of thyroid cancer cases, 5-10% are familial and autosomal dominant; 17% are follicular, and 2-3% are medullary and often diagnosed in patients with multiple endocrine neoplasia syndrome (23).
Thyroid cancer is the eleventh most frequently diagnosed cancer in Korean children < 14 years of age and the fifth most common cancer in girls (26). The prevalence of thyroid cancer in girls increased from the tenth to the fifth most common cancer between 2002 and 2011. Thyroid cancer in children tends to present at a more advanced stage than that in adults and with a higher frequency of lymph node and pulmonary metastases. Distant metastasis is less common than regional lymph node involvement, and the lung is the most common site of distant metastasis. Pediatric patients with papillary thyroid cancer (PTC) have a good prognosis, despite a high incidence of cervical lymph node metastasis (27, 28). Metastatic nodes are characterized by a round shape, asymmetrical cortical thickening, hyperechogenecity, multiple punctate calcifications, cystic changes, loss of fatty hilum, or increased vascularity on color Doppler imaging (29). The reasons for the variations between children and adults are unknown, but are generally thought to be due to differences in mutations and oncogene expression in the thyroid (30, 31).
In addition to suspicious malignant nodules, a diffusely enlarged thyroid with numerous microcalcifications on US is defined as a thyroid malignancy and should be evaluated using fine-needle aspiration (FNA) biopsy with a BRAF analysis (31).
Papillary thyroid cancer is frequently associated with genetic alterations. The BRAF mutation is intrinsically associated with increased progression and aggressiveness of PTC. Similarly, the BRAF mutation has a high predictive value for PTC recurrence (32). The frequency of the BRAF mutation increases with age. The prevalence of the BRAF mutation in Korean children (30-50%) is lower than that in adults (70-83%) (31, 33).
Follicular carcinoma accounts for approximately 17% of thyroid cancers and is more common in females than males (23, 26, 27, 28). The distinction between a benign (Fig. 11) and malignant follicular neoplasm can only be made by evaluating the presence of capsular or vascular invasion during a histological examination. The estimated rate of malignancy for follicular neoplasm is variable, ranging from 10-30% (34, 35). Follicular thyroid tumors present with several genetic alterations, such as aneuploidy, RAS mutations, and PAX8/PPARγ rearrangements. Activation of RAS gene mutations plays an important role initiating follicular thyroid tumors. RAS mutations are found in follicular adenomas but are more prevalent in follicular carcinomas (35, 36).
The US characteristics of autoimmune diseases include enlargement of the thyroid with reduced echogenicity, heterogeneity, and hypervascularity. Diffusely infiltrative papillary or follicular thyroid carcinomas may have all of these features and, thus, may be mistaken for autoimmune thyroid disease. Furthermore, patients may present with misleading thyrotoxicosis (Fig. 12).
Diffuse Thyroid Disease
Ultrasonography findings indicative of diffuse thyroid disease (DTD) are characterized by a diffusely enlarged thyroid gland, decreased or increased diffuse heterogeneous parenchymal echogenicity, a coarse echotexture, micronodulation, and scattered microcalcifications (37, 38).
Ultrasonography is not generally required to diagnose DTD; however, Hashimoto's thyroiditis is primarily a subclinical disease, and US can detect this subset of patients before they come to clinical attention when typical US findings are present (39). US plays a role excluding focal thyroid disease and in assessing the size of the thyroid gland. US is also used to distinguish, characterize, and detect diffuse infiltrating tumors (37, 39).
Graves' Disease
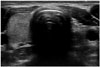
Hyperthyroidism is rare in childhood and is most commonly caused by Graves' disease. It affects 0.02% of children or 1 in 5000 (23). The peak incidence occurs from 11-15 years of age with a female predominance. A positive family history is common (37). Antibodies stimulate TSHR leading to lymphocyte infiltration of the thyroid gland. US reveals diffuse heterogeneous and hypoechoic enlargement of the thyroid (Fig. 13). Color Doppler imaging reveals a hypervascular pattern in the thyroid referred to as a "thyroid inferno".
Hashimoto's Thyroiditis
Hashimoto's thyroiditis is one of the most common organ-specific autoimmune diseases. Its annual incidence is estimated to be between 0.3 and 1.5 cases per 1000 persons, with no significant race-related predominance (37). Hashimoto's thyroiditis affects 1.3% of children and has a female predominance (23, 37, 38). This disease, which is the most common DTD, is characterized by diffuse lymphocytic infiltration. Diagnosis is made by detecting antithyroid antibodies, including antithyroid peroxidase and antithyroglobulin antibodies. US is useful for measuring thyroid size and assessing echotexture. US imaging shows an enlarged gland with a diffusely heterogeneous, coarse echotexture and multiple discrete hypoechoic micronodules ranging from 1-6 mm in diameter. There may be coarse septations from fibrous bands (37, 38).
Suppurative Thyroiditis
Acute suppurative thyroiditis is rare and is the result of microbial infection of the thyroid gland. Patients present with a tender mass or swelling over the thyroid gland and fever. When the left lobe of the thyroid is involved and a fistula is present between this lobe and the ipsilateral pyriform sinus, the possibility of a left third pharyngeal pouch remnant should be considered (Fig. 14). The infected portion of the gland appears enlarged and heterogeneous on US scans. A focal abscess may have developed, and prominent swelling in adjacent soft tissue resulting from associated myositis and cellulitis may be present (18, 23, 37).
CONCLUSION
Imaging, particularly US, plays an important role evaluating the various thyroid diseases affecting pediatric patients. Dual imaging with US and scintigraphy increases the diagnostic yield for CH. US is the most sensitive diagnostic modality for evaluating thyroid nodules and to diagnose of thyroid carcinoma because it facilitates aspiration biopsies and follow-up. Testing for cancer-specific mutations in thyroid FNA samples increases the diagnostic accuracy of FNA cytology. Additionally, US enables the diagnosis of lymph node metastasis.













 XML Download
XML Download