

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Obesity has become a worldwide pandemic health problem, and morbid obesity leads to a high rate of complications associated with metabolic syndrome, including type 2 diabetes mellitus (DM). There is strong evidence that bariatric surgery can successfully treat most patients with morbid obesity, and it is the only recommended effective treatment for morbid obesity (1, 2, 3). Furthermore, bariatric surgery, most typically gastric bypass, reduces DM-related deaths (4), which is why gastric bypass surgery has been proposed as a new treatment modality for type 2 DM (5, 6, 7).
Laparoscopic Roux-en-Y gastric bypass (LRYGB) is a safe and effective standard bariatric surgical procedure and has been performed recently to control DM (5, 8). Laparoscopic mini-gastric bypass is a safe alternative to LRYGB because of its simple surgical technique, comparable or lower complication rate, and similar efficacy, including weight reduction and control of DM (9, 10, 11, 12). However, mini-gastric surgery imaging findings have seldom been reported.
In this study, we explain and illustrate laparoscopic mini-gastric bypass surgery to control DM and the postoperative imaging features and associated complications as seen on fluoroscopy and computed tomography (CT) to familiarize radiologists.
Surgical Technique
Five or six trocars (four 12-mm and two 5-mm) are usually placed under general anesthesia. An endo-stapler (Echelon Flex Endoscopic Articulating Linear Cutter, Ethicon Endosurgery, Cincinnati, OH, USA) is used to divide the stomach from the angle of His to 2 cm proximal to the pylorus along the lesser curvature to form a long and narrow mini-gastric tube. Although the volume of the mini-gastric tube is usually 150-180 cc, it can be changed according to the patient's body mass index (BMI). Then, additional surgical clips are applied in a staple line to prevent post-procedural bleeding and as reinforcement.
The jejunum is mounted antecolically with the mini-gastric tube 200 cm distal to the Treitz ligament via a side-to-side anastomosis using an endo-stapler (Endo GIA Universal Stapler, Covidien Autosuture, Mansfield, MA, USA). The gastric antrum, duodenum, and proximal jejunum are consequently bypassed. An acute angle is made with an anchoring suture adjacent to the gastro-jejunostomy to prevent bile reflux and food in the bypassed segment (Fig. 1). A nasogastric tube is passed into the efferent loop after intraoperative leak testing and gastroscopy to detect intraluminal bleeding and to determine the size of the anastomotic site.
Postoperative Anatomy
Our institution performs an upper gastrointestinal series (UGI) for all patients on postoperative day (POD) 1 with a water-soluble iodinated contrast agent to exclude obstructions, strictures, and staple line leaks before patients start a liquid diet. Diluted water-soluble contrast (up to 250 mL) is given via a straw. Fast-sequence images of the gastro-jejunostomy are obtained in anteroposterior, oblique, and lateral projections when the patient swallows. The shape and volume of the stomach can vary according to the patient's BMI when the water-soluble contrast passes into the remnant stomach. The desired pattern for the remnant stomach is a tubular shape due to the bariatric procedure, and an afferent loop is usually unidentified throughout its course (Fig. 2). Although an anchoring suture is made adjacent to the gastro-jejunostomy for angulation to prevent bile reflux and exclude food from the bypassed segment, the afferent loop can be infrequently opacified. Contrast should not pass the gastro-jejunostomy.
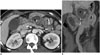
A contrast-enhanced CT scan is performed if postoperative complications are detected on the UGI or are clinically suspected. A CT scan shows the remnant stomach, the efferent loop, the bypassed segments, and their relationship with adjacent structures (Fig. 3). The anastomosis site is typically recognized as a highly attenuated staple line and can be used to find the surgical field.
Complications
Hematoma and Hemorrhage
Hemorrhage and hematoma (Fig. 4) usually occur in the surgical field, including the staple line of the stomach and adjacent to the gastro-jejunostomy site. Hemorrhage and hematoma can also occur at a trocar site or from internal solid organs located in the surgical field, such as the liver or spleen, in up to 3.4% of patients undergoing mini-gastric bypass (11). The origins of hemorrhage include insufficient vascular ligation or hemostasis or injury to solid organs (13). When blood through the surgical drainage or incision site is identified and accompanied by clinical hypotension, intra-abdominal hemorrhage clinically manifests. Hematoma and hemorrhage are typically shown as high density fluid or hemoperitoneum (60-80 Hounsfield units) in the acute stage on a CT scan. Because a hematoma is a low density fluid in the chronic stage, it is not easy to distinguish from ascites or an abscess (14).
Anastomotic Narrowing and Stenosis
Stricture or stenosis (Figs. 5, 6) at the gastro-jejunostomy site is a relatively common complication that can result in postprandial vomiting and pain (15). Causes for a passage disturbance can be anastomotic edema secondary to surgery or over-sewing (16). A transient standing column of contrast agent in the esophagus lasts < 1 minute in a typical case of postoperative edema, and recovery is expected within 2 weeks. Early stricture or severe edema should be considered when contrast remains static in the esophagus for > 1 minute. Persistent distension and air-fluid in the remnant stomach and esophagus on follow-up studies suggests a stricture, and balloon dilation using endoscopy is likely necessary (17).
Abscess
An abscess (Fig. 7) is usually associated with an intestinal leak or perforation (18, 19). CT is the primary means for diagnosing intestinal leaks and abscesses. CT reveals an intra-abdominal abscess as a collection of fluid with rim enhancement, internal gas formation, and adjacent inflammatory changes.
Leak
Anastomotic leaks (Fig. 8) are an uncommon but ominous complication and occur in 0.5-1.9% of patients undergoing the surgery (10, 12, 20, 21). A leak is common at the gastro-jejunostomy site. A postoperative UGI is necessary to identify a leak before patients start a liquid diet. Water-soluble contrast agent directly spills into the extra-luminal space and perigastric soft tissue during a UGI study. Pneumoperitoneum, localized fluid collection in an unexpected site, or an abscess are highly suspicious of leakage on a CT scan, and the presence of oral contrast in the extra-luminal space is obvious evidence of leakage. Although the majority of leaks are detected during the first 7 PODs, some leaks can occur later (22). Immediate surgical exploration should be advocated if a leak is strongly suspected, even with a negative postoperative UGI result.
Wound Complications
Wound complications (Fig. 9) are easily detected at the incision site. Subcutaneous fat stranding, mottled air bubbles, or a small volume of fluid in an adjoining trocar site are expected as postoperative findings. A wound infection may result from inflammation or necrosis of wound closure material and form an abscess. A larger volume of fluid and severe fat stranding should be considered an abscess. Wound dehiscence as a consequence of loosening of closure material or an incision hernia at the trocar site can be detected on a CT scan (14).
Marginal Ulcers
Marginal ulcers (ulcer at the gastrojejunal anastomosis) are one of the most problematic postoperative complications following gastric bypass surgery. The main factors leading to a marginal ulcer are a large gastric tube and exposure to acid, typically on the jejunal side (23, 24). Marginal ulcers occur in 0.6-8.0% of patients undergoing the surgery (9, 10, 12, 25).
Detecting a marginal ulcer (Fig. 10) on a UGI study or a CT scan is less reliable than endoscopy; therefore, these radiological examinations may produce negative results despite a positive endoscopic result. Although an ulcer is typically treated medically, surgery is required in cases of perforation, hemorrhage, ulcer intractability, or obstruction (24). Edematous wall thickening at the involved site, including perilesional fat stranding, perforation, or abscess may be seen on CT, and a stenosis or deformity can be identified as a result of scarring or fibrosis.
Acute Cholecystitis after Bariatric Surgery
The incidence of cholelithiasis increases by approximately 10-40% in patients with morbid obesity, compared with those of normal weight. The risks for gallbladder (GB) stones and cholecystitis (Fig. 11) increase following the rapid weight loss after bariatric surgery, ultimately leading to cholecystectomy in 20-30% of patients. Thus, many surgeons perform a pre-emptive cholecystectomy concomitantly with bariatric surgery (26). Typical CT findings of acute cholecystitis include GB wall thickening, distension, subserosal edema of the GB, high-attenuation bile, and fluid stranding and collection in an adjacent area (27).
Spontaneous Perforation in the Bypassed Segment
The bypassed segment of a mini-gastric bypass includes the stomach, duodenum, and proximal jejunum. A spontaneous perforation in the bypassed segment (Fig. 12) in a patient who has undergone mini-gastric surgery has not been reported. Macgregor et al. (28) reported a perforation in the bypassed segment after Roux-en-Y gastric bypass in < 0.24% of patients, including the duodenum and stomach. The mechanism of perforation is a complication of peptic ulcer disease or an obstruction of the biliopancreatic limb due to internal herniation (28). Because an endoscopic or fluoroscopic approach is not available for the bypassed segment, a CT scan is necessary to confirm the diagnosis.











 XML Download
XML Download