

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
As a noninvasive imaging tool, magnetic resonance imaging (MRI) has the capabilites of multiplanar imaging and superior soft tissue contrast, which are very important in delineating the pathologies of the abdomen's solid and hollow organs. Duodenal lesions are generally detected incidentally, although various appearances are encountered radiologically. In accordance with the recent increased and widespread use of MRI in abdominal imaging, these often asymptomatic lesions are encountered more frequently today in patterns that some radiologists may not be familiar with.
In this pictorial review, patients who had undergone abdominal MRI for various indications were evaluated retrospectively, and those with duodenal lesions were selected. The MRI patterns of the duodenal lesions were assessed and analyzed.
Normal Variations
Sphincter Contraction
Although it is normal that the most distal part of the common bile duct (CBD) and pancreatic duct cannot be visualized in magnetic resonance cholangiopancreatography (MRCP), sometimes it may be confused with real pathologies. These segments of the choledochus and the pancreatic duct are covered with muscle and belong to the Vaterian sphincter complex (1). A small intrasphincteric segment in these ducts or the existence of sphincter contractility may cause the Vaterian sphincter complex to not be visualized (12), which in turn causes false negative results in the diagnosis of small impacted calculus and papillary tumors. Moreover, severe contraction of the sphincter may cause what is called the "pseudo-calculus effect", which has a convex, semilunar shape in the distal CBD (Fig. 1) (1). There are phasic contractions approximately 4 times per minute that last 4.3 ± 0.5 seconds and that are revealed with manometric studies in the Vaterian sphincter complex, which normally has a basal pressure (12).
Major Papilla Variation
The major duodenal papilla is the slight mucosal bulging where the ampulla of Vater, created by the junction of the choledochus and the pancreatic duct, opens to the duodenum. The location, size and shape of the major papilla vary (3). The major papilla is in the 1/3 middle section of the descending segment of the duodenum at a rate of 75% and is located more distally in the horizontal segment at a rate of 25% (Fig. 2) (34).
Prominent Papilla
The major duodenal papilla is the oval protrusion in the medial part of the descending segment of the duodenum. Although the papilla has a variable diameter, it is generally approximately 5-10 mm. The normal bulging of the papilla into the duodenum lumen is smaller than 1 cm (3). Normally, the papilla is scarcely differentiated from the duodenal mucosal folds around it (45). Although hypertrophic papilla can rarely occur as a normal variant, it may also develop in connection with inflammatory (acute cholangitis, acute pancreatitis, biliary calculus, periampullary diverticulum, infection-infestation, etc.) or neoplastic processes (intraductal papillary mucinous tumor, ampullary adenoma and tumor, periampullary cancer, etc.) (Fig. 3) (45).
Congenital Anomalies
Diverticula
A duodenal diverticulum is the herniation of the mucosa and the muscular layer from the intestine wall. A real duodenal diverticulum is congenital and arises from luminal recanalization anomalies during embryologic development (678910), and it includes all of the layers in the intestine wall. A pseudo-diverticulum, which is more frequently encountered, includes only the mucosa and submucosa layers and is most frequently found on the medial wall of the 2nd and 3rd segments of the duodenum (67810). Diverticula are most frequently seen in the duodenum, after the colon in the gastrointestinal (GI) tract (11). They are seen relatively more frequently in women, and the prevalence increases with age (9). Most cases are asymptomatic and are detected incidentally at a rate of approximately 11% during GI barium studies or during endoscopy that is performed for other reasons (911). Diverticulitis may be complicated with perforation in the retroperitoneal space (7). The area in which diverticula are most frequently seen is in the 2 to 3 cm periphery of the ampulla of Vater and are called juxtapapillary or periampullary diverticula. Diverticula in this location may rarely cause functional disorders in the ampulla and compression of the CBD, depending on their size and configuration, and in this way, may lead to biliopancreatic symptoms such as jaundice, cholangitis, or biliary calculus (911). If the diverticulum lumen is full of air or a mixture of air-liquid, it may be easily identified with computerized tomography (CT) or MRI. However, in the event that the lumen is completely filled with liquid, the diverticulum may be confused with cystic tumors of the pancreas or with choledochus cysts on CT or MRI (69). It is important to show the continuity in the duodenum lumen of a diverticulum with multiplanar imaging on MRI to avoid misinterpretation. Moreover, the air-liquid level is beneficial for identifying diverticula in axial sections and enabling their differentiation from the cystic lesions that may be seen in this location (Figs. 4, 5, 6) (69).
Intraluminal Duodenal Diverticulum
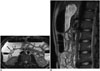
Intraluminal duodenal diverticulum (IDD) is one of the most rarely seen congenital anomalies of the duodenum, and it is thought to arise from defects in the recanalization process of the primitive foregut in the early gestational period (12131415). Typically, it is seen at the 2nd section of duodenum, near the papilla Vateri (1213). IDD is gender-free and is most frequently seen in the 3rd-5th decades (12). Although it is mostly asymptomatic, sometimes it may cause early satiety, bloating, nausea, and/or vomiting based on partial or total duodenal obstruction (16). Forty percent of cases may be accompanied with GI and extraintestinal malformations, such as annular pancreas, midgut malrotation, imperforate anus, choledochocele, or superior mesenteric artery (SMA) syndrome as well as extraintestinal anomalies such as congenital heart disease, bladder extrophy, or hypoplastic kidney (121314). In barium studies, IDD is seen as a pedunculated polypoid lesion that is projected into the real lumen and that is filled with barium, creating the appearance of what is called a pathognomonic "airport windsock" (Fig. 7) (101213). Lesions change place with peristaltism. On T2-weighted images, a hypointense rim that covers the diverticulum lumen inside the duodenum lumen (Fig. 7) is also a very important sign in diagnosis. This liquid collection, which is hypointense in its surrounding and which changes shape and place with intestinal peristaltism, is nearly pathognomonic for the IDD diagnosis on MRI and MRCP (12).
Annular Pancreas
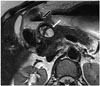
Annular pancreas is a rare congenital anomaly in which the pancreatic tissue band completely or partially surrounds the 2nd segment of the duodenum (17181920). The pancreas beings to develop from the 1 dorsal and 2 ventral buds as the outgrowth of the primitive foregut in the 4th-5th week of gestation. As the left ventral bud regresses, the right ventral bud rotates towards the dorsal as the duodenum expands, and it combines with the dorsal bud in the 7th week. As the ventral bud creates the head of the pancreas together with the uncinate process, the pancreatic body and tail are created from the dorsal bud (1819). Two theories are discussed in the development of annular pancreas. According to Lecco's theory, the left ventral bud regresses while the right ventral bud adheres on the duodenum wall and consequently becomes stretched and elongated together with a rotation towards the dorsal. According to Baldwin's theory, in contrast, the left ventral bud does not regress but rather moves in a contrary direction to that of the right ventral bud around the duodenum and they combine with the dorsal bud; in this way, the duodenum is covered with the pancreatic tissue (71819). Presentation of annular pancreas in children and in adults varies. Although vomiting caused by severe duodenal obstruction is the major symptom in the first year of life, 50% of adults are asymptomatic, and the condition is detected incidentally. The remaining 50%, however, show symptoms such as abdominal pain, vomiting, peptic ulcer, duodenal obstruction and pancreatitis in the 3rd-6th decades; however, the main presentation is pancreatitis (7181920). On MRI, the pancreatic tissue is recorded as completely or partially encircling the descending segment of the duodenum at the ampulla Vateri level or caudally (18). MRCP reveals an aberrant pancreatic duct encircling the duodenum (1819). This aberrant duct may be drained into the intrapancreatic part of the CBD or the Wirsung or Santorini ducts (Fig. 8) (20).
Duplication Cysts
Duplication cysts arise from the recanalization defect in the duodenum lumen in the embryogenic period (7). They are very rare in the GI tractus, and approximately 12% occur in the stomach and duodenum (7). Duodenal duplications are well-circumscribed cystic masses that are seen more frequently in the 2nd and 3rd segments of the duodenum (Fig. 9) (721). These cysts are not typically communicated with the duodenum lumen (717). They are mostly incidental; however, sometimes they may also cause biliary obstruction and pancreatitis because of their location (717). Carcinoma may occur inside duplication cysts, although very rarely. For this reason, intracystic mural nodules and vegetation should be taken into consideration (722).
Choledochocele
Choledochocele, which is the cystic dilatation of the intraduodenal segment of the choledochus, is concordant with type-III choledochal cysts according to Todani classification. It constitutes 4% of all choledochal cysts (Fig. 10) (23). Choledochocele is often encountered in elderly males. It generally presents with acute pancreatitis. Moreover, gallstones, cholangitis, cholecystitis are also seen. As choledochoceles protrude into the duodenum lumen, they may cause duodenal obstruction symptoms, hemorrhage and perforation. There exists a risk of pancreatic divisum and malignity, although the risk is low (232425).
Non-Neoplastic Acquired Diseases
Dilated Duodenum Secondary to Superior Mesenteric Artery Syndrome
Also known as Wilkie's syndrome, SMA syndrome is a rare pathology that arises from the compression of the 3rd segment of the duodenum intermittently between the aorta and the SMA, causing obstruction in the duodenum and proximal gastroduodenal dilatation (2627282930). It is more frequent in young adults and in women (28). Typical symptoms are epigastric pain, postprandial dyspepsia, nausea, vomiting of bile-stained material, early satiety and weight loss (262829). The most frequently encountered factor in etiopathogenesis is the decrease of superior mesenteric fatty tissue between the aorta and the SMA caused by extreme loss of weight. More rare reasons include short or abnormally inserted ligament of Treitz and hyperlordosis (282930). Normally, the fat pad between the aorta and the SMA increases the distance and angle between these two vascular structures and prevents the development of obstruction in the duodenum (30). It is stated in previous studies that the angle between the aorta and the SMA is 6-22° in those who have SMA syndrome and 25-60° in those who do not. Moreover, it is also found that the distance between the aorta and the SMA is shorter than normal in the duodenal crossing point in SMA syndrome (2-8 mm in SMA syndrome but 10-28 mm in normal cases) (Fig. 11) (2627).
Duodenal Wall Thickening Secondary to Acute Pancreatitis
Because the duodenum shows anatomic continuity with the pancreas, it is affected by the pathologies of the pancreas. Pancreatitis is the most frequently seen inflammatory process that affects the duodenum (710). Acute inflammation of the pancreas and excretion of exocrine enzymes may cause mild-severe duodenal edema, duodenal wall thickening and gastric outlet obstruction (Fig. 12) (710).
Postbulbar Stenosis
Peptic ulcer disease is the most common cause of benign duodenal stenosis. Duodenal ulcer may cause ectopic drainage of the CBD producing a hook-shaped configuration at its distal end (3132). In addition, benign conditions such as duodenal Crohn's disease and chronic pancreatitis, non-steroidal anti-inflammatory drugs, trauma, hyperplasia of Brunner's gland, corrosive agents, and malignant pathologies (duodenum, pancreas, gallbladder, ampulla) or metastases can cause duodenal stenosis or obstruction (Fig. 13) (31).
Duodenal Involvement of Celiac Disease
Indistinct fold (decrease in mucosal folds) is one of the imaging findings of duodenal involvement of celiac disease (6). Moreover, focal mucosal erosions, mural asymmetry, diffuse or nodular thickening in mucosal folds, mild luminal dilatation, stricture, and intramural fat storage are also reported (Fig. 14) (6).
Biliary Tract Fistulas
Biliary tract fistulas are rare and may occur spontaneously or postoperatively. A long-term history of biliary stones, recurrent biliary tract infections, CBD stones, malignancy and previous biliary surgery are the most common causes of a choledochoduodenal fistula. In this situation, the biliary system is exposed to intestinal flora and fluid (33). It is reported that gallbladder cancer may develop secondary to the chemical irritation of this back flow via choledochoduodenal fistula (34). On plain films, air can be seen in the biliary tree (Fig. 15).
Choledochoduodenostomy
Choledochoduodenostomy is one of the biliary bypass procedures for treating benign biliary strictures or malignant obstruction of the biliary system. This operation is also indicated in patients with biliary fistulas, recurrent bile duct stones, stenosis of the sphincter of Oddi, and choledochal cysts (Fig. 16) (35).
External Compression
The duodenum wall is a rare place of settlement for pancreatic pseudocysts. However, the inflammation and secretion that spread from the pancreas may cause the creation of pseudocysts on the posterior surface of the duodenum that are not covered by the peritoneum and that directly touch the head of pancreas. Because of this anatomic relationship, pseudocysts are most frequently seen in the 2nd segment (Fig. 17) (3637). A similar compression can be caused by rare diseases such as hydatid cysts (Fig. 18).
Neoplasms
Peutz-Jeghers Syndrome
Peutz-Jeghers syndrome (PJS) is an autosomal dominant syndrome that is characterized by mucocutaneous pigmentation and hamartomatous GI polyps (38). Patients present with intestinal obstruction, abdominal pain, rectal hemorrhage, and/or intussusception. Full GI system involvement may occur except for the esophagus; however, PJS primarily affects the small intestines (738). Although the polyps may be very small, they may also reach a diameter of 3-4 cm, and they may be sessile or pedunculated. Polyps are histopathologically hamartoma (Fig. 19) (738).
Ampullary Carcinoma
Ampullary carcinomas originate from the glandular epithelium of the ampulla of Vater (5). Symptoms such as jaundice, abdominal pain, nausea, and vomiting occur relatively early, and for this reason, at the time of the diagnosis, ampullary carcinomas often manifest as small tumors (5). They are usually in polypoid or papillary form, and an infiltrative form can occur but is infrequent. On MRI, iso- or hypointense mass lesions that protrude into the duodenal lumen can be seen in T1- and T2-weighted images (Fig. 20) (5).
Duodenal Adenocarcinoma
Adenocarciomas typically occur in the 5th and 6th decades, and they are the most common malignant tumors of the small intestine (6). More than 60% of small bowel malignant tumors arise in the duodenum (678). GI obstruction, bleeding and jaundice are the most common symptoms. Focal mural thickening, infiltrative annular strictures, and polypoid intramural or intraluminal masses are the imaging features on MRI (Fig. 21) (678).



















 XML Download
XML Download