

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Immunoglobulin G4 (IgG4)-related kidney disease (IgG4-KD) is a comprehensive term indicating the renal involvement of IgG4-related sclerosing disease (IgG4-SD), which is an immune-mediated systemic disease that can affect almost every organ system (1). The most common feature of IgG4-KD is tubulointerstitial nephritis with increased IgG4-positive plasma cells, along with fibrosis (123456). IgG4-KD usually responds well to steroid therapy; however, if not properly treated, it may cause acute or chronic renal dysfunction and can progress to irreversible renal failure (6). Therefore, a timely and accurate diagnosis that ensures early steroid treatment is crucial for improving the patient outcome. In addition, as IgG4-KD is usually associated with IgG4-SD involving other organs, including autoimmune pancreatitis (AIP) or IgG4-related sclerosing cholangitis, identifying the renal lesions can provide clues for diagnosing IgG4-SD (56789). Therefore, radiologists must be aware of the imaging features of IgG4-KD, as well as also be familiar with this disease entity. The purpose of this article is to provide a comprehensive pictorial review of the imaging spectrum of IgG4-KD, and to discuss differential diagnosis from its mimickers. We will also briefly review the clinicopathologic characteristics of IgG4-KD.
Clinicopathologic Characteristics of IgG4-KD
Immunoglobulin G4-related kidney disease usually affects middle-aged or elderly patients and shows a definite male predominance (73-90%), which is similar in patients with IgG4-SD involving other organs (57910). IgG4-KD is usually accompanied by other organ involvement in IgG4-SD, typically AIP, and approximately 1/4 or 1/3 of AIP patients have IgG4-KD (111213). Isolated cases of IgG4-KD without other organ involvement, is very rare. In our series, only 3 (6%) of 48 IgG4-KD patients had renal lesions alone.
The clinical manifestations are usually mild or even asymptomatic. As the disease progresses, renal dysfunction or abnormalities are seen in imaging studies; only then it becomes clinically evident. Renal function at the time of the initial diagnosis varies from normal function to renal failure. Mild proteinuria occurs in approximately half the patients (710). Hypergammaglobulinemia, either IgG4 or total IgG, is the serologic hallmark of IgG4-KD as well as IgG4-SD. Although up to 30% of patients with IgG4-SD have a normal range of serum IgG4 level, almost all IgG4-KD patients have an elevated serum IgG4 level (710). Other serologic findings include an elevated serum immunoglobulin E level, eosinophilia, and hypocomplementemia (15).
Immunoglobulin G4-related kidney disease manifests most commonly as tubulointerstitial nephritis, followed by glomerular disease such as membranous glomerulonephritis (1). Other less frequent conditions, including IgG4-related chronic sclerosing pyelitis, IgG4-related plasma-cell arteritis, and IgG4-related inflammatory pseudotumors of the ureter, have also been reported (1141516). The key histologic findings of IgG4-KD are dense lymphoplasmacytic infiltration with increased IgG4-positive plasma cells, and storiform fibrosis, both of which are identical to the findings of IgG4-SD involving other organs (Fig. 1) (310). In addition, the characteristic microscopic features of IgG4-related tubulointerstitial nephritis are nests of inflammatory cells with irregular fibers surrounding them, and immune complex deposition in the tubular basement membrane (51718).
Imaging Spectrum of IgG4-KD
The diagnosis of IgG4-KD is based on a combination of imaging, serologic and histologic findings, as well as other organ involvement (57). Among these findings, the imaging findings may be the most important component as they are usually the first recognized abnormal findings of IgG4-KD, which enables clinicians or radiologists to consider the occurrence of this disease. Therefore, it is crucial to be aware of the imaging spectrum of IgG4-KD in order to obtain a timely and accurate diagnosis.
Distribution of IgG4-KD
Immunoglobulin G4-related kidney disease can be divided into three types, based on their location: renal parenchymal, renal pelvic, and a perinephric lesion. A renal parenchymal lesion is the most common type, followed by a renal pelvic and a perinephric lesion (91219). Two types can sometimes appear together. Among the 48 IgG4-KD patients seen at our institution, 36 (75%) had only renal parenchymal lesions, 5 (10%) had only renal pelvic lesions, and 1 (2%) had only perinephric lesions. Two types of IgG4-KD co-existed in 6 (13%) patients: 5 with renal parenchymal and renal pelvic lesions, and 1 with renal parenchymal and perinephric lesions. Because of the systemic nature of the disease, IgG4-KD typically shows multiplicity and bilaterality (91920). In our series, 45 (94%) and 37 (77%) patients had multiple and bilateral lesions, respectively.
Renal Parenchymal Lesions
A renal parenchymal lesion in IgG4-KD can show three patterns: a single nodule, multiple nodules (Fig. 2), and diffuse patchy infiltrative lesions (Fig. 3). Among these, multiple nodules are the most common pattern (121920). Renal parenchymal nodules are located predominantly in the renal cortex. They are usually small and round, or wedge-shaped. It rarely appears as a single, large, mass-like lesion mimicking a solid renal neoplasm (91219).
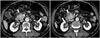
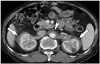
On contrast-enhanced CT, renal parenchymal lesions are mostly hypodense to the normal renal cortex in the early phase, i.e., the arterial or corticomedullary phase, and progressively get enhanced in the portal or delayed phase (Fig. 2) (192021). These lesions are usually not visible on precontrast CT scans (1219). It can often be challenging to perceive early, subtle renal lesions depending solely on CT scans. MR imaging can improve detection of the lesions in such cases. On T2-weighted MR images, renal lesions typically appear hypointense relative to the normal renal parenchyma, and are easily detectable due to the obvious contrast between the dark lesions and the bright, normal parenchyma (Figs. 3, 4) (91222). On the other hand, renal lesions usually appear isointense on T1-weighted images, and they are barely visible or are invisible (Fig. 4). On dynamic contrast-enhanced MR images, most renal lesions are hypointense to the normal renal cortex in the arterial phase, and progressively enhance in the portal and delayed phases, thus becoming indistinct as the phase passes; this is similar to the dynamic enhancement pattern seen on CT (Fig. 5) (91222). Diffusion-weighted MR imaging (DWI) has recently been reported to be particularly useful for detecting IgG4-KD (9). Kim et al. (9) reported that the sensitivity of DWI (b value, 1000 s/mm2) for detecting IgG4-KD was significantly higher than that of T2-weighted images (100% vs. 77%). The renal lesions have marked hyperintensity on DWI at a high b value and, conversely, have marked hypointensity on the apparent diffusion coefficient map (Figs. 4, 5). These DWI findings can be explained by the histopathologic background of IgG4-KD, i.e., dense lymphoplasmacytic infiltration with fibrosis. This may be supported by the hypointensity seen on T2-weighted images and the progressive enhancement pattern seen on dynamic contrast-enhanced images, which may also represent fibrosis (912). DWI may also have the potential to detect IgG4-KD at an early or subclinical stage (923).
Ultrasonographic (US) findings of IgG4-KD are not specific and are less sensitive for lesion detection than CT or MR imaging (24). The most common US findings are ill-defined, non-mass-like areas of decreased echogenicity (24). Other US findings include irregular lobular thickening of the renal parenchyma with a bulging contour and multiple, hypoechoic masses with decreased vascularity, as compared to the normal renal cortex (24).
Renal Pelvic and Perinephric Lesions
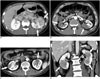
Renal pelvic or perinephric lesions are much rarer than renal parenchymal lesions. Renal pelvic lesions manifest as diffused wall thickening of the renal pelvis, or as a mildly enhanced, soft-tissue mass encasing the renal pelvis (1219). These lesions can be unilateral (Fig. 6) or bilateral (Fig. 7). Hydronephrosis seldom occurs, unless the ureter is entrapped by accompanying periaortic retroperitoneal fibrosis. In our series, only 1 of 10 patients with renal pelvic lesions had a mild, unilateral hydronephrosis without retroperitoneal fibrosis. Perinephric lesions typically appear as a diffuse, rim-like, soft-tissue mass surrounding the kidneys (Fig. 8) (12). These masses usually exhibit homogeneous and mild enhancement. They can be also unilateral or bilateral.
Response of IgG4-KD to Steroid Therapy
Immunoglobulin G4-related kidney disease usually shows a rapid and favorable response to steroid therapy, which similar to IgG4-SD with other organ involvement, regardless of the lesion location (i.e., renal parenchymal, renal pelvic or perinephric). According to the pathologic subtype, tubulointerstitial nephritis generally responds better than membranous glomerulonephritis (1). Approximately 90% of IgG4-KD patients show improvement of decreased renal function and abnormal imaging findings with steroid treatment (110121719). During the steroid treatment, the lesion size and number dramatically decreases, as seen on imaging studies (Fig. 9). After completion of the steroid therapy, varying degrees of renal atrophy can develop, especially in patients with renal parenchymal lesions, and which may be proportionate to the extent of the renal involvement before treatment (61012). In our series, the majority of patients having renal parenchymal lesions of a diffuse patchy infiltrative pattern, or with large, multiple nodules, experienced mild cortical scars after steroid therapy (Fig. 9). IgG4-KD as well as other organ involvement of IgG4-SD can relapse in up to 20% of patients, mainly during maintenance therapy or after cessation of the steroid therapy (Fig. 9) (612). Without steroid treatment, the renal lesions can increase in size and number, or progress to diffuse cortical involvement (12).
Mimickers of IgG4-KD and the Differential Diagnosis
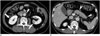
As stated above, IgG4-KD has a broad spectrum of imaging features. Therefore, various neoplastic or non-neoplastic conditions of the kidneys can mimic IgG4-KD. With regard to IgG4-KD manifesting as multiple, renal parenchymal lesions, the differential diagnosis includes acute pyelonephritis, infarction, metastasis, and lymphoma (Fig. 10) (91220). Acute pyelonephritis typically appear as unilateral or bilateral, multiple, ill-defined, and round or wedge-shaped lesions of decreased enhancement (Fig. 10A) (2526). Clinical findings, which include fever, pyuria or knocking tenderness in the flank area, may undoubtedly be important clues suggesting acute pyelonephritis. In addition to the aforementioned clinical findings, perilesional infiltration or fluid collection, and renal or perirenal abscesses seen on imaging examinations, may also help to differentiate acute pyelonephritis from IgG4-KD. Well-demarcated, large, wedge-shaped areas showing poor contrast enhancement are typical of renal infarction, although they may mimic the patchy infiltrative pattern of IgG4-KD (Fig. 10B) (2527). A hyperenhanced cortical rim at the lesion periphery, the so-called cortical rim sign, can be seen in approximately half of the patients with renal infarction, whereas in IgG4-KD this sign has never been reported in the published medical literature, including our study (2728). Metastases usually appear as bilateral, multiple, and less exophytic nodules, and they are therefore capable of closely mimicking IgG4-KD (Fig. 10C) (29). The presence of primary malignancy is the most important clue to metastasis. The common sites of primary malignancy are the lung, breast, contralateral kidney, and colon (30). Renal lymphomas commonly manifest as multiple, parenchymal nodules/masses (Fig. 10D), or as a renal pelvic or perinephric mass with mild homogeneous enhancement, which can be quite similar to the IgG4-KD features (313233). Moreover, lymphomas often appear hypointense on T2-weighted MR images and have diffusion restriction (3334). However, renal lymphomas seem more bulky than IgG4-KD and frequently accompany multiple, retroperitoneal lymphadenopathies, compared to IgG4-KD (932).
In rare cases, when IgG4-KD manifests as a single parenchymal nodule/mass, it can be challenging to distinguish it from renal cell carcinoma, especially when non-clear cell types, such as the papillary or chromophobe type, appear as a non-hypervascular mass (Fig. 11) (35). Diffuse wall thickening of the renal pelvis or a parapelvic mass in IgG4-KD should be differentiated from urothelial carcinoma (Fig. 12). The relatively common bilaterality and uncommon hydronephrosis in IgG4-KD may be helpful in differentiating the two diseases, and may warrant further comparative studies.
In addition to the above-mentioned analyses regarding the imaging features, detection of other organ involvement of IgG4-SD, i.e., AIP (Fig. 13), sclerosing cholangitis, retroperitoneal fibrosis (Fig. 13) or sialadenitis, may be essential for differentiating IgG4-KD from the other diseases, as isolated IgG4-KD without other organ involvement is very rare, as demonstrated in our study (6%). According to recently established diagnostic criteria of IgG4-KD, the presence of other organ involvement is an important diagnostic component (57). Alternatively, identification of renal lesions can be of crucial importance for the diagnosis of IgG4-SD involving other organs, especially when imaging features of other organs are not characteristic of IgG4-SD. A typical example would be the differential diagnosis of focal-type AIP and pancreatic cancer; in this situation, the presence of renal lesions may substantially favor the former diagnosis (Fig. 14) (8).
On the other hand, despite the detailed analysis using various imaging modalities, it can still be difficult to differentiate IgG4-KD from other diseases, in particular neoplasms. In such cases, CT- or US-guided biopsy of the renal lesions should be considered, in order to avoid unnecessary surgery caused by the misdiagnosis as neoplasm, in patients having IgG4-KD.
CONCLUSION
Immunoglobulin G4-related kidney disease has a broad spectrum of imaging features and a variety of mimickers to be differentiated from it. Awareness of the broad imaging spectrum of IgG4-KD, differential diagnosis from its mimickers, and important clinicopathologic characteristics, will facilitate its accurate and prompt diagnosis as well as optimally timed treatment.










 XML Download
XML Download