

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
MRI is the most important noninvasive imaging modality for the diagnosis of hydrocephalus. However, hydrocephalus is an ambiguous diagnosis that may actually result from many different causes. In evaluation of the patients with hydrocephalus, the visualization of the cerebrospinal fluid (CSF) pathways is essential. In assessment of the CSF pathways, besides anatomical information with high spatial and contrast resolution multiplanar imaging, functional information including CSF flow dynamics is also very important (1, 2). For MRI, the functional analyses of CSF flow dynamics and aqueductal patency primarily rely on the demonstration of flow void signal (3). The phase-contrast MRI (PC-MRI) is extremely sensitive to CSF flow and provides the potential for noninvasive flow quantification (2, 4, 5). Since cine PC-MRI is incapable of demonstrating CSF pathways anatomically, it should be used in conjunction with high-resolution two-dimensional (2D) T2-weighted (T2W) turbo spin echo (TSE) and three-dimensional (3D) heavily-T2W sequences (such as 3D-constructive interference steady state [CISS]) (6, 7, 8). However, the demonstration of both anatomical detail and functional analyses of CSF flow with these sequences has a number of drawbacks and limitations in its applications.
With the introduction of 3-T MRI system, high resolution images and shortened imaging times have been achieved. However, the most important concern about the 3-T MRI unit is its high specific absorption rate (SAR). On 3-T MR units, a new 3D T2W TSE technique named "sampling perfection with application optimized contrast using different flip angle evolutions" (SPACE, Siemens Healthcare, Erlangen, Germany) has recently been introduced and uses variable flip angle distribution and non-volume selective refocusing pulses with short echo spacing.
Besides providing excellent spatial resolution images that could be reconstructed in any desired plane, the use of variable flip angle further decreases the acquisition time and reduces SAR. The advantages of this technique in evaluation of the spine, pelvis, and abdomen have been reported previously (9, 10, 11, 12). T2W 3D-SPACE with high spatial resolution and multiplanar reconstruction capacity would also be advantageous for imaging the CSF pathways. Algin and Turkbey (13) recently reported that T2W 3D-SPACE with variable flip angle mode provides noninvasive evaluation of CSF similar to that in cine PC-MRI sequence. In their study, they also proposed that T2W 3D-SPACE could be used as a single technique to obtain both morphological and physiological information. In another study by Dinçer et al. (14), it was reported that T2W 2D-TSE sequence with 2-mm slice thickness demonstrates flow void nearly equal to cine PC-MRI. However, to the best of our knowledge, the comparison of T2W 3D-SPACE and T2W 2D-TSE sequences in the evaluation CSF flow was not previously described. The purpose of our study was to compare the accuracy of diagnosing aqueductal patency and image quality between T2W 3D-SPACE with variable flip angle mode sequence and T2W 2D-TSE (2 mm section thickness without flow compensation) sequences on a 3-T unit in patients with hydrocephalus.
MATERIALS AND METHODS
Patients
Ninety-nine patients (43 men and 56 women; mean age, 37.1 years; age range, 6-71 years) with clinical and radiological diagnosis of hydrocephalus who were examined in our MRI unit between June 2012 and July 2013 were included. The retrospective study was approved by our Institutional Review Board. All patients were informed about the study and gave consent for participation.
According to the etiology of hydrocephalus, the patients were divided into subgroups. These were as follows: 30 primary (idiopathic) aqueductal stenosis; 17 secondary aqueductal stenosis (caused by tectal tumors in 9, 4th ventricular masses in 5, and arachnoid or colloid cysts in 3 patients); 33 Arnold Chiari malformations; and 19 communicating hydrocephalus. Of the 17 patients with secondary aqueductal stenosis, 5 patients with 4th ventricular masses were diagnosed histopathologically (2 with pilocytic astrocytoma, 2 with hemangioblastoma, and 1 with medulloblastoma). The diagnosis of the remaining 12 patients of the secondary aqueductal stenosis and other 82 patients with primary aqueductal stenosis, Arnold Chiari malformations, and communicating hydrocephalus was based on typical conventional and CSF flow MRI findings and clinical and radiological follow-up. The diagnosis of primary aqueductal stenosis was based on the demonstration of the obstructive character of the pathologic condition and fine membrane on the MR cisternography technique such as 3D-CISS and conventional MRI techniques.
MRI Technique
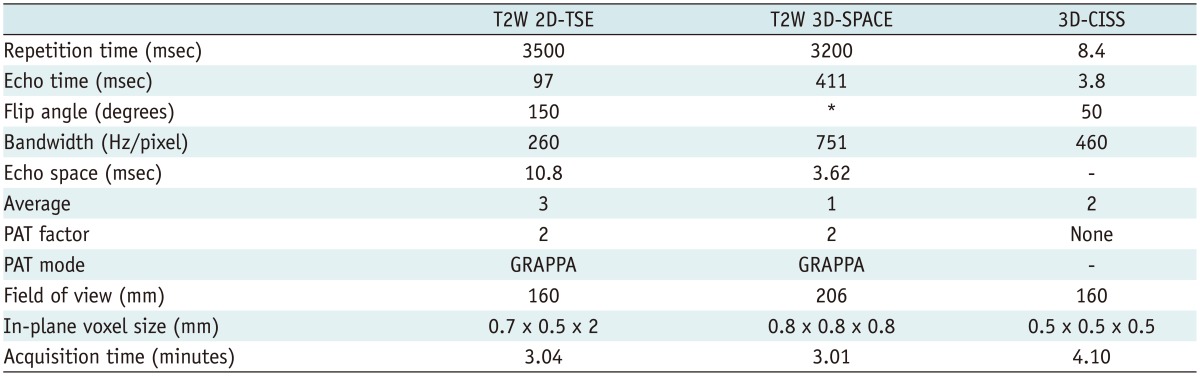
All patients were examined with a 3-T MRI scanner (Verio; Siemens, Erlangen, Germany) with an 8-channel head coil. After acquisition of the T2W TSE in axial plane, 3D-CISS, T2W 2D-TSE (2 mm section thickness without flow compensation), and T2W 3D-SPACE were obtained in sagittal plane. The sequence parameters are summarized in Table 1. These sequences were followed by midline sagittal and axial-oblique cine PC-MRI in which the axial-oblique images were taken in a plane perpendicular to aqueduct. In the cine PC-MRI, the in-plane and through-plane velocity encoding was in the craniocaudal direction. The sequence parameters were as follows: repetition time/echo time, 36/5.6 msec; number of excitation, 2; field of view, 240 × 240 mm; section thickness, 4 mm; flip angle, 20°; and velocity encoding, 20-22 cm/sec for axial-oblique plane and 6-8 cm/sec for sagittal plane. Retrospective cardiac gating was used in this sequence. Depending on the patient's heart rate, the acquisition time was approximately 4-6 minutes for PC-MRI.
MR Evaluation
MR images were evaluated retrospectively by two radiologists with 10 and 4 years of experience in neuroimaging. The evaluation steps were as follows: first step was the evaluation of sagittal T2W 2D-TSE images by two radiologists independently. Three weeks later, in the second step, the readers independently evaluated the T2W 3D-SPACE images. In both steps, according to visibility of flow void in aqueduct, the aqueductal patency was scored on a relative 4-point scale: grade 0, no flow void in the aqueduct through the third ventricle to the apex of the fourth ventricle; grade 1, flow void in only one of these compartments; grade 2, flow void in two of them; and grade 3, flow void in all of them. For each of these sequences, grade 0 was diagnosed as occluded aqueduct, and grade 1 to 3 was considered as patent aqueduct. In the case of disagreement about aqueductal patency, a final diagnosis was based on consensus by the two readers for statistical analysis.
In the third and fourth steps, each of the T2W 2D-TSE and T2W 3D-SPACE were separately compared with 3D-CISS for image quality. The evaluations were made in consensus of two radiologists. In the evaluation, the image quality in terms of wall conspicuity, contrast (between CSF and brain parenchyma), continuity, sharpness, and background homogeneity of the third ventricle, aqueduct, and fourth ventricle were assigned on a 5-point relative scale. Relative scores of each of these sequences (T2W 2D-TSE and T2W 3D-SPACE) were as follows: 1, superior to 3D-CISS; 2, slightly superior to 3D-CISS; 3, equal to 3D-CISS; 4, slightly inferior to 3D-CISS; 5, clearly inferior to 3D-CISS.
For the final step, the aqueductal patency was evaluated on midline sagittal and axial-oblique plane cine PC-MRI by consensus of the same two readers and scored as: grade 0, no aqueductal flow on any of the PC sequences (aqueduct occlusion); grade 1, patent aqueduct. In statistical analyses, the cine PC-MRI was accepted as the reference standard in the evaluation of the aqueductal patency.
Statistical Analysis
The statistical analyses were performed using PASW Statistics software (version 18; SPSS Inc., Chicago, IL, USA). After grading of each sequence, sensitivity, specificity, positive predictive value, negative predictive value, and accuracy of the T2W 2D-TSE and T2W 3D-SPACE images for the patency of the aqueduct were calculated. The McNemar test was used for comparison of the sensitivity and specificity of the T2W 2D-TSE and T2W 3D-SPACE. A p value of less than 0.05 was considered to indicate a statistically significant difference. The Wilcoxon signed rank test was used to analyze the ordinal scale aqueductal patency and overall image quality. A two-tailed p < 0.05 was considered to indicate a significant difference.
Inter-observer agreement for grading of the aqueductal patency was calculated by using the κ statistic.
RESULTS
Aqueductal Patency
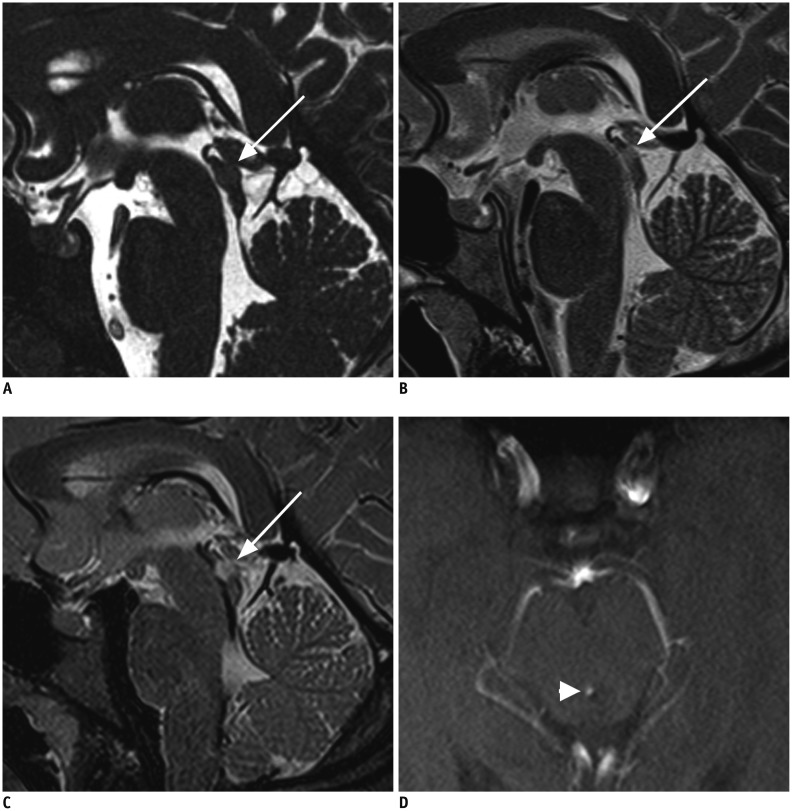
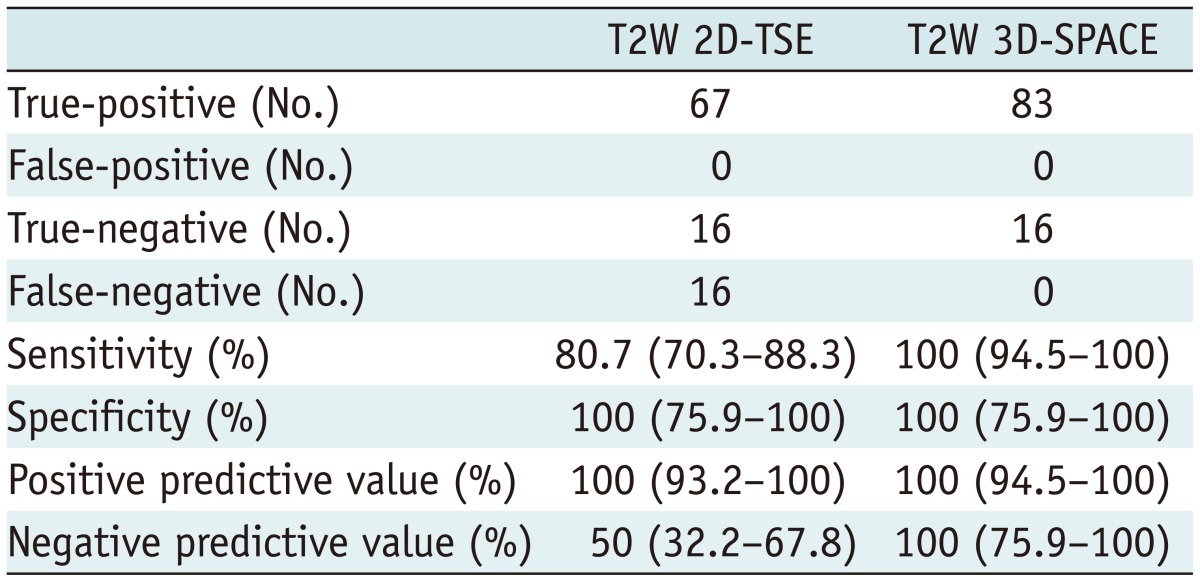
According to cine PC-MRI, 83 patients (83.8%) had patent aqueduct and 16 had (16.2%) aqueduct occlusion. In the evaluation of aqueductal patency, the T2W 2D-TSE and T2W 3D-SPACE were in agreement with the cine PC-MRI findings in 83 of 99 (83.8%) and 99 of 99 (100%) patients, respectively. Table 2 shows the sensitivities and specificities with corresponding 95% confidence intervals (CIs) of the T2W 2D-TSE and T2W 3D-SPACE for the diagnosis of the aqueductal patency. Therefore, the T2W 3D-SPACE was found to be equal to the cine PC-MRI in the evaluation of the aqueductal patency. Significant differences between the T2W 3D-SPACE findings and results of the T2W 2D-TSE (p < 0.001) occurred. While the T2W 2D-TSE demonstrated an aqueduct occlusion in 16 patients (false negative), the cine PC-MRI and T2W 3D-SPACE revealed patent aqueduct in those patients, and diagnostic sensitivity of T2W 2D-TSE was 80.7%. Accordingly, in comparison with the cine PC-MRI, all aqueduct occlusions were also detected using both T2W 3D-SPACE and T2W 2D-TSE, and the diagnostic specificity of both sequences were 100%. While the T2W 2D-TSE demonstrated an aqueduct occlusion in 16 patients (16.2%, false negative), cine PC-MRI and T2W 3D-SPACE revealed patent aqueduct in those patients (Figs. 1, 2). In evaluation of the grading of aqueductal patency, the T2W 3D-SPACE was significantly superior to T2W 2D-TSE (Table 3).
The kappa values for inter-observer agreement in grading of the aqueductal patency was 0.714 (p < 0.001; 95% CI, 0.608-0.820) for T2W 2D-TSE and 0.899 (p < 0.001; 95% CI, 0.817-0.981) for T2W 3D-SPACE.
Image Quality Evaluation
In side-by-side comparisons of the T2W 2D-TSE and T2W 3D-SPACE with 3D-CISS, the image quality was found to be inferior to the 3D-CISS. In comparison with the 3D-CISS, the mean scores of the T2W 2D-TSE and T2W 3D-SPACE in image quality were 4.01 ± 0.6 and 4.31 ± 0.5, respectively. The readers tended to prefer the 3D-CISS in both comparisons because the means were greater than 3 (p < 0.001). In the T2W 2D-TSE, the scores of image quality were equal in 18 of 99 patients (18.2%), slightly inferior in 62 (62.6%), and clearly inferior in 19 patients (19.2%) compared to the 3D-CISS. The scores of image quality in the T2W 3D-SPACE were equal in 3 of 99 patients (3%), slightly inferior in 62 patients (62.6%), and clearly inferior in 34 patients (34.3%) compared to the 3D-CISS.
DISCUSSION
In our study, the most important advantage of the T2W 3D-SPACE over T2W 2D-TSE sequence was sensitivity of the aqueductal patency evaluation when compared to the T2W 2D-TSE sequence which led to false negative results in 16.2% of patients. T2W 3D-SPACE yielded the same sensitivity as the PC-MRI, which is known to have very high sensitivity for aqueductal patency. However, the T2W 3D-SPACE did not show the same benefit in the morphological evaluation of the CSF pathways, and the 3D-CISS was found to be superior to both the T2W 2D-TSE and T2W 3D-SPACE sequences in assessment of the aqueduct morphology.
In recent years, to be able to choose the best treatment modality including shunt insertion and endoscopic surgery and to guide these surgical procedures, evaluation of the CSF dynamics in addition to complex anatomy of the ventricular system from the ventricles to the subarachnoid space have gained importance in determining the appropriate treatment modality. Evaluation of the aqueductal patency, diagnosis of the underlying pathology in aqueductal stenosis, and postsurgical assessment of the patients with hydrocephalus are very difficult tasks for radiologists with routine cranial MRI (1). As hydrocephalus results in alterations in the CSF flow signal on conventional MRI, the differential diagnosis between obstruction of flow and excessive turbulent flow by using motion-sensitive MRI techniques is sometimes difficult. The evaluation of flow through the CSF pathways has a major importance in demonstrating the CSF dynamics and plays an important role in the decision-making process. The CSF flow void is recognized as signal loss within the ventricular system. Consequently, a combination of cine PC-MRI and 3D-CISS have gained wide acceptance in demonstration of flow void and anatomical details, respectively (14).
As stated in the literature, with cine PC-MRI, reliable qualitative and quantitative information for CSF flow through aqueduct could be obtained and used as a criterion standard (1). Cine PC-MRI is the only noninvasive imaging method presently available to quantify the CSF flow. However, several drawbacks have limited the use of cine PC-MRI for evaluation of CSF flow imaging. First, PC-MRI can be incorrect in the presence of turbulent-complex flow or if the velocity encoding value is not correctly chosen. Second, this sequence is two-dimensional and demonstrates only selected plane in a slice, and the multiple slices require long acquisition times. Sometimes inadequate or false results may be seen due to partial volume effect. Although cine PC-MRI is very sensitive to demonstrate flow, it cannot provide adequate anatomical information. Furthermore, the 3D-CISS can give high spatial resolution for anatomical information. However, it cannot provide physiological information about the aqueductal flow because it has lower sensitivity for flow void (7). For this reason, other alternative MRI techniques have been studied in patients with hydrocephalus. The T2W 2D-TSE, which is the main sequence of CSF flow imaging, is frequently obtained to provide more anatomical detail than physiological information (15). However, in this sequence, the flow void signal is affected by the acquisition parameters such as time of echo, slice thickness, spatial resolution, receiver bandwidth, the number of averaging, and echo train length as well as by the technical characteristics of the MR imaging system (14, 15). Dinçer et al. (14) evaluated various TSE sequences for assessment of flow void through endoscopic third ventriculostomy fenestration. They reported that the sagittal T2W 2D-TSE sequence with 2-mm slice thickness revealed nearly equal information compared to cine PC-MRI. In their study, for the evaluation of the CSF flow void, this sequence had 98% accuracy, 100% sensitivity, 95% specificity, and 100% negative predictive value. In our study, the lower sensitivity and specificity of the T2W 2D-TSE sequence could be attributed to a different patient population compared to their study. In their study (14), the efficacy of the T2W 2D-TSE was evaluated in terms of patency of ventriculostomy fenestration.
SPACE is a recently introduced 3D T2W TSE sequence with variable flip-angle refocusing pulses that has been developed by Mugler et al. (16). Several potential fields of application were also reported in the medical literature including hepatobiliary system, spine, and pelvic organs (10, 11, 12, 17, 18). Also, some potential advantages of this sequence for CSF flow over other techniques include the use of thinner slice thickness without interslice gaps, high sensitivity of flow, and high signal-to-noise ratio.
On the T2W 3D-SPACE with variant flip-angle mode images, which is a TSE variant, the CSF proximal to the obstruction demonstrates a high signal (restricted CSF) whereas the free-floating CSF is seen as a low signal, which is called "flow void" sign. These features offer a non-invasive evaluation of the CSF hydrodynamics, aqueductal patency, and third ventricular integrity (19). The flow-void sign simply represents moving protons. It has been demonstrated that the flow-void sign is dependent on some sequence parameters. It has been proven that the time of echo, slice thickness, receiver bandwidth, and average number are well known sequence parameters and affect flow-void sign (14, 20). Our finding that the T2W 3D-SPACE is more flow-sensitive than the T2W 2D-TSE may be explained by a superiority of all sequence parameters of the T2W 3D-SPACE when compared to the T2W 2D-TSE (Table 1).
The efficacy of the T2W 3D-SPACE in CSF flow was previously reported by Algin and Turkbey (13). They recommended in their study that it would be an efficient single technique for evaluation of aqueductal patency to provide both morphological and physiological information. Although including a relatively low patient population, this study (13) revealed an excellent correlation of the T2W 3D-SPACE in consensus-based scores (21/21). While the data concerning anatomical details are limited in their study, our results also support the findings of this study in term of aqueductal patency. Our results also indicated that 3D-CISS is more effective than both T2W 3D-SPACE and T2W 2D-TSE in the assessment of anatomical details. In both side-by-side comparisons of the T2W 2D-TSE with 3D-CISS and T2W 3D-SPACE with 3D-CISS, the readers tended to prefer the 3D-CISS images over other sequences. Accordingly, the 3D-CISS should remain the MRI sequence of choice in morphological evaluation of the CSF pathways.
Some limitations in our study occurred. First, we did not use more accurate invasive tests such as intrathecal gadolinium-enhanced MR cisternography or laparoscopic surgery as a reference standard. However, the principal purpose of this study was to compare the different sequences and the observers' subjective perception of image quality. Second, although the readers were blinded to the type of reviewed MRI sequence, the particular differences in appearances of these sequences made it impossible for the readers to be completely blinded. Third, we did not optimize the sequence parameters. The 3D-CISS was obtained with 0.5-mm isotropic voxels whereas the T2W 3D-SPACE sequence was obtained with 0.8-mm isotropic voxels and slice thickness, which might explain slightly higher resolution and finer anatomical details of the 3D-CISS over T2W 3D-SPACE. We agree that in any future studies comparing the T2W 3D-SPACE to the 3D-CISS, similar voxel sizes should be used.
In conclusion, the T2W 3D-SPACE is superior to T2W 2D-TSE for the evaluation of aqueductal patency in patients with hydrocephalus. The T2W 3D-SPACE may hold promise as a highly accurate alternative to PC-MRI for physiological and morphological evaluation of aqueductal patency. For complicated cases, incorporating this sequence in an MRI protocol while evaluating patients with hydrocephalus is a valuable adjunct to the 3D-CISS and could be an ideal CSF imaging protocol for both physiological and morphological evaluation of CSF flow-saving acquisition time.


 XML Download
XML Download