

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Magnetic resonance (MR) arthrography is a diagnostic modality used widely in the diagnosis of glenoid, labrum, and rotator cuff lesions (1, 2, 3, 4, 5). In particular, using intravenous paramagnetic contrast medium to enhance the joint cavity, indirect shoulder MR arthrography can provide arthrogram-like images without radiation exposure, invasive procedures, or coordination of additional scheduling (6, 7, 8, 9, 10). In a recent study, based on a relatively small number of patients, indirect shoulder MR arthrography showed similar diagnostic accuracy to direct MR arthrography (11).
Recently, three-dimensional (3D) techniques with isotropic resolution have facilitated shorter imaging times and multiplanar reformation in musculoskeletal imaging (12, 13, 14, 15). Additionally, the advent of high-performance gradients also has enabled 3D fast spin-echo (FSE) imaging in reasonable scan times, which now show comparable diagnostic accuracy and reliability compared with conventional two-dimensional (2D) imaging in multiple performance studies (16, 17, 18). However, to our knowledge, the number of studies regarding diagnostic performance of 3D isotropic FSE techniques for rotator cuff tears is limited (19, 20). Thus, the purpose of this study was to compare the diagnostic accuracy of 3D indirect isotropic T1-weighted FSE MR arthrography with that of conventional 2D indirect MR arthrography for the diagnosis of rotator cuff tears in a large number patient population.
MATERIALS AND METHODS
Patients
Our retrospective study was approved by the Institutional Review Board. The requirement for informed consent was waived.
From March 2011 to July 2012, 207 patients who had undergone indirect shoulder MR arthrography followed by arthroscopic surgery were initially included. At our institution, patients who are suspected of having rotator cuff lesions, based on clinical history or physical examination, undergo indirect MR arthrography. However, most of patients visiting the orthopedic outpatient clinic for shoulder pain already have MR images obtained at outside hospitals. In this instance, the treatment plan is made based on these images. Then, we performed indirect MR arthrography 1 day prior to the surgery if the outside MR images were of poor quality or if they were from more than 6 months ago according to our orthopedic surgeon's policy. Inclusion criteria were: 1) patients with shoulder discomfort who had undergone indirect shoulder MR arthrography followed by arthroscopic surgery, and 2) indirect MR arthrography performed with both conventional 2D FSE and 3D isotropic T1-weighted FSE sequences. Among them, two patients who had undergone previous surgeries on the symptomatic shoulder were excluded. As a result, in total, 206 shoulders in 205 patients with indirect MR arthrography were finally included for image analysis in this study. The study population consisted of 98 men (age range, 17-77 years; mean age, 51.0 years; 96 Koreans, 2 Caucasians) and 107 women (age range, 35-78 years; mean age 61.6 years; all Koreans). The patients complained of shoulder pain with or without limitation of movement, shoulder dislocation, or weakness. The time interval between indirect MR arthrography and arthroscopic surgery was less than 1 day for 153 patients, 1 day for 51 patients, and 5 days for one patient.
MR Imaging Protocol
Based on the clinical standard protocol for indirect MR arthrography, 0.1 mmol/kg of gadobutrol (Gadovist, Bayer Healthcare, Berlin, Germany) was injected into an antecubital vein. Immediately after the injection of contrast media, patients were instructed to exercise their shoulders for 15 minutes. After exercise, MR imaging was performed with a 3.0-T imager (Gyroscan Intera Achieva; Philips Medical Systems, Best, the Netherlands) with a dedicated receive-only shoulder coil. Patients were imaged supine with the humerus in a neutral position and the thumb pointing upward.
Conventional 2D MR images were performed first, followed by a 3D isotropic T1-weighted FSE sequence. Conventional 2D MR images were obtained with fat-suppressed T1-weighted FSE sequences in axial and oblique coronal planes (repetition time [TR]/echo time [TE], 610/10; field-of-view [FOV], 16 cm; acquisition matrix number, 320 × 256; acquisition matrix size, 0.5 × 0.6 mm; receiver bandwidth, 64 kHz; section thickness, 3 mm; intersection gap, 0 mm; echo train length, 5; number of averages, 2; acquisition time, 4 minutes 16 seconds) parallel to the long axis of the supraspinatus (SSP) tendon, and oblique sagittal plane (TR/TE, 610/10; FOV, 16 cm; acquisition matrix number, 320 x 256; acquisition matrix size, 0.5 × 0.6 mm; receiver bandwidth, 74 kHz; section thickness, 3 mm; intersection gap, 0 mm; echo train length, 5; number of averages, 2; acquisition time, 4 minutes 31 seconds) perpendicular to the long axis of the SSP tendon. We then performed the 3D isotropic fat-suppressed T1-weighted FSE sequence (volumetric isotropic turbo spin-echo acquisition, VISTA; Philips Medical Systems, Best, the Netherlands) in the oblique coronal plane (TR/TE, 350/19 ms; FOV, 15 cm; acquisition matrix number, 300 × 300; acquisition matrix size, 0.5 × 0.5 mm; receiver bandwidth, 109 kHz; section thickness, 0.5 mm; intersection gap, 0 mm; echo train length, 25; number of averages, 2; parallel reduction factor, 2; acquisition time, 6 minutes 10 seconds).
Image Analysis
All images from the 2D and 3D acquisitions were separated. One musculoskeletal radiologist with 8 years of experience in the evaluation of shoulder MRI (reader I) and a senior resident from the department of radiology (reader II) were blinded to the arthroscopic results and reviewed the MR images independently in two separate sessions retrospectively. The two sessions were separated by at least 1 month to minimize recall bias.
There has been controversy regarding the true anatomical relationship and footprint areas of SSP and infraspinatus (ISP) tendons (21, 22). Because these two tendons overlap and fuse together on the footprint, it is difficult to separate these tendons and delineate them (21, 23). Thus, we regarded SSP and ISP tendon tears as one entity to improve the accuracy of correlation between MR and arthroscopic findings in the same way as other previous reports on rotator cuff tears (11, 19, 24), rather than seeking to differentiate them.
Using a five-point scale as a confidence level, the SSP-ISP tendons and subscapularis (SSC) tendons were scored on a scale of 0-4 (0, absolutely not a tear; 1, probably not a tear; 2, equivocal; 3, probably a tear; 4, absolutely a tear). The confidence level scores were dichotomized with a cutoff for the presence of tear between confidence level scores 3 and 4 (positive) and 0-2 (negative). Then, the radiologists scored each SSP-ISP tendon lesion from the 2D T1-weighted sequences and 3D isotropic T1-weighted sequences as full-thickness tear, partial-thickness tear, or no tear. Partial-thickness SSP-ISP tendon tears were classified as articular- or bursal-sided tears. Intrasubstance tears were not evaluated because they are often occult on tendon visualization during arthroscopic surgery and thus cannot be accurately correlated with arthroscopic findings.
Images were presented in random order at each reading session and evaluated using a picture archiving and communication system (PACS; Centricity Radiology RA 1000; General Electric Healthcare, Chicago, IL, USA). A full-thickness tear of the SSP-ISP tendon was diagnosed if a signal abnormality as intense as the fluid involving the entire thickness was noticed that extended from the articular surface of the rotator cuff to the subacromial/subdeltoid bursa and tendinous discontinuity with or without retraction of the musculotendinous junction (25). A partial-thickness tear of SSP-ISP tendon was diagnosed if a focal region of fiber discontinuity filled with fluid signal extending across a portion of the tendon at either the bursal or the articular surface with surface abnormalities was observed without involving the entire thickness (25). When an intra-tendinous high signal was noticed without definite extension to the articular or bursal surface, it was scored as no tear. The criteria for a SSC tendon tear were a tendon discontinuity, contrast media extending across the articular or bursal surface of the tendon with or without entering into the tendon substance, and caliber changes. Subluxation or dislocation of the long biceps tendon was considered as a secondary sign of a SSC tendon tear too (26). The same diagnostic criteria were applied on both 2D and 3D images. For 2D sequences, only T1-weighted images were used for the analysis because 3D images were not obtained with T2-weighted sequence. The reformation of the 3D images was performed simultaneously during the image analysis using Aquarius iNtuition (ver. 4.4.6; TeraRecon, Inc., San Mateo, CA, USA). Reformatted images with a slice thickness of 0.5 mm in the axial and oblique sagittal planes were semi-automatically generated in a standard fashion after Digital Imaging and Communications in Medicine files of 150 oblique coronal images with 3D isotropic FSE T1-weighted MR images were imported to the program network from PACS. When injury was suspected, arbitrary planes according to the axis of the involved structures were also used.
Arthroscopic Shoulder Surgery
Arthroscopic surgeries were performed by an orthopedic surgeon with 8 years of experience in shoulder surgery who was not blinded to the MR imaging findings. The interval between MR imaging and arthroscopic surgery was 1 day or less, except for one patient who underwent arthroscopic surgery 5 days after the MR imaging. The surgeon described the presence of SSP-ISP and/or SSC tendon tears. The grades of SSP-ISP tendon tears were categorized as full-thickness or partial-thickness tears. Partial-thickness SSP-ISP tendon tears were classified as articular- or bursal-sided tears. When a SSC tendon tear was noticed on arthroscopy, the involved width of the SSC tendon tear at the first facet of the lesser tuberosity was recorded.
Statistical Analysis
The arthroscopic findings were used as a standard of reference in all statistical analyses. The sensitivities, specificities, and accuracies in both readers were calculated for the diagnosis of overall SSP-ISP tendon tears (full- and partial-thickness tears together, without considering the grades of the tears) for both 2D and 3D sequences. We then used the receiver operating characteristic (ROC) method based on the five-point scale confidence scores. The diagnostic performances of both readers were evaluated using the area under the ROC curve (AUC), followed by assessment of the differences in the AUC values between the 2D and 3D sequences of both readers according to the method of DeLong et al. (27).
The sensitivities, specificities, and accuracies for the diagnosis of full- and partial-thickness tears were calculated separately. The sensitivities, specificities, and accuracies were also evaluated in the detection of SSC tendon tears for both 2D and 3D sequences. To determine the difference in sensitivity and specificity for the diagnosis of rotator cuff tears between 2D and 3D sequences in each reader, we performed McNemar's test for matched samples (28).
We used κ statistics to calculate the interobserver agreement between the readers regarding the detection of SSP-ISP and SSC tendon tears without considering the grade of tears for 2D and 3D sequences. Then, weighted κ coefficients were also used to assess the interobserver agreement between two readers in discriminating between full-, partial-thickness tears, or no tears of SSP-ISP tendon in evaluating both 2D and 3D sequences using three ordinal values as follows: 2, full-thickness tear; 1, partial-thickness tear; and 0, no tear. The degree of agreement was interpreted as 'poor' for a κ value of less than 0, 'slight' for a κ value of 0-0.20, 'fair' for a κ value of 0.21-0.40, 'moderate' for a κ value of 0.41-0.60, 'substantial' for a κ value of 0.61-0.80, and 'excellent' for a κ value of 0.81-1.0. All statistical analyses were performed using statistical software (SPSS Statistics Standard, ver. 18.0.0, IBM, Chicago, IL, USA; MedCalc for Windows, ver. 12.5.0.0, MedCalc Software, Mariakerke, Belgium). A p value of < 0.05 was considered to indicate statistical significance.
RESULTS
Diagnostic Performance
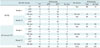
Interpretations on 2D and 3D sequences by both readers were compared with arthroscopic findings (Table 1). 56/103 (54%) SSC tendon tears involved less than 50% of the first facet. The number of SSC tendon tears involving more than 50% and less than 100% of the first facet was 28 of 103 (27%). In 19 of 103 (18%) cases, SSC tendon tears involved the entire first facet or more. There were 33 of 206 (16%) shoulders without rotator cuff tears, including 16 shoulder dislocations with or without labral tears, eight adhesive capsulitis, five paralabral cysts, three calcific tendinitis, and one biceps pulley lesion. Table 2 and Figure 1 show the AUC values reflecting overall accuracy for the detection of SSP-ISP and SSC tendon tears using each reader's confidence scores, based on the five-point scale of two sequences and corresponding ROC curves, respectively, while sensitivities, specificities, and accuracies are summarized in Table 3. There was no significant difference between 2D and 3D sequences in either reader regarding the diagnosis of SSP-ISP and SSC tendon tears.
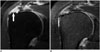
No full-thickness SSP-ISP tendon tear was missed by both readers using both sequences. A full-thickness tear of the SSP-ISP tendon, which was correctly diagnosed using the 3D isotropic sequence, was misinterpreted as a bursal-sided partial-thickness tear using 2D sequences by both readers (Fig. 2). There were three cases of bursal-sided partial-thickness tears of the SSP-ISP tendon showing disagreement between 2D and 3D isotropic sequences. The first was correctly diagnosed by both readers using the 2D sequence only, but the 3D isotropic sequence failed to demonstrate the tear (Fig. 3). On the other hand, the other two cases were correctly detected only by using 3D isotropic sequence by both readers. There were two false-negative and one false-positive cases in the diagnosis of articular-sided partial-thickness tear of the SSP-ISP tendon using both sequences by both readers. An articular-sided SSP-ISP tendon partial-thickness tear was detected only by reader I using 3D isotropic sequence. Among 103 arthroscopically proven SSC tendon tears, 56 cases were correctly detected in both readers using both sequences (Fig. 4). There was a false-positive case of SSC tendon tear that was scored as a tear by both readers using both sequences. In this patient, focal contrast media accumulation at the articular side of the SSC tendon was suspected by both readers.
Interobserver Agreement
Interobserver agreement was substantial in the diagnosis of SSP-ISP tendon tears for both non-weighted and weighted κ statistics. Interobserver agreement for diagnosing SSC tendon tear was moderate for both 2D and 3D sequences using non-weighted κ statistics (Table 4).
DISCUSSION
Conventional MR imaging with 2D sequences provides excellent tissue contrast and high spatial resolution. However, thick slices and small gaps between slices create a partial volume averaging effect, which may obscure rotator cuff pathologies (29). On the other hand, 3D isotropic sequences allow for image reformation in any arbitrary imaging plane with a single acquisition, resulting in decreased MR examination times and reduced partial volume averaging effects (14, 29). Due to these advantages, 3D sequences have been used for years for the evaluation of the musculoskeletal system, including of the knee, ankle, shoulder, elbow, and wrist joints and the cervical spine (12, 13, 14, 15, 30). Although several studies have reported a comparable diagnostic performance of 3D isotropic sequences to 2D sequences, most of these used the gradient-echo technique (24, 31, 32) or FSE images with intermediate-weighted sequences (16, 17, 33, 34, 35, 36). Regarding the diagnosis of shoulder pathologies, several previous studies compared the accuracy of 3D isotropic sequences and conventional 2D sequences and reported there was no significant difference (24, 31).
Recently, development of more efficient imaging techniques with high-performance MR imaging workstations has enabled 3D FSE sequence to be feasible. Especially compared with 3D gradient-echo sequences, it also has advantages in terms of reduced magnetic susceptibility and field inhomogeneity artifacts with tissue contrast similar to that of 2D FSE sequences. Since a preliminary study by Rybak et al. (37), 3D FSE imaging has been used for several studies of shoulder imaging and revealed similar diagnostic performances to conventional 2D sequences (19, 20, 38).
Compared with previous reports, the present study was based on a large patient population and was performed with 2D and 3D FSE T1-weighted sequences using indirect MR arthrography for all patients for the diagnosis of SSP-ISP and SSC tendon tears. Also, we minimized the time interval between MR examination and arthroscopic surgery to strengthen the correlation between the findings. In our study, AUC analysis revealed no significant difference between the diagnostic performance of 2D and 3D sequences in detecting SSP-ISP and SSC tendon tears despite several advantages of 3D isotropic techniques versus 2D sequences, as described above. One suggested cause is that 3D imaging requires more acquisition time than 2D imaging in each orthogonal planes, suffering from more motion artifacts (19). Additionally, a long echo train length may result in a blurring effect, which can lead to false interpretations. Increasing receiver bandwidth or parallel reduction factor can reduce these drawbacks, but it inevitably has costs in signal-to-noise ratio as a trade-off. Also, the voxel profile generated by phase encoding is inferior to that generated with selective excitation (39). These shortcomings of 3D sequence may have offset the advantages.
Regarding indirect MR arthrography, previous studies reported the sensitivity and specificity for the detection of SSP-ISP tendon tears to be 67-100% and 75-89%, respectively (10, 11, 24, 40, 41). More specifically, the sensitivity and specificity of the full-thickness SSP tendon tears were reported as 80-95% and 96-100%, respectively, and those for partial-thickness SSP tendon tears were reported as 38-71% and 86-88%, respectively (40, 41). Although the diagnostic accuracies using indirect MR arthrography were high for full-thickness tears, those for partial-thickness tears vary widely. The sensitivities and specificities in the diagnosis of SSC tendon tears using indirect MR arthrography were reported to be 64-67% and 75-88% (11, 24). In our study, the diagnostic performance of indirect MR arthrography in both 2D and 3D techniques for overall SSP-ISP tendon tears (sensitivity, 92-95%; specificity, 88-95%) was comparable to published data with slightly higher specificity. Regarding full-thickness tears, our sensitivity (91-95%) was similar to previous reports, whereas our results showed relatively lower specificity (87-94%). The sensitivity (64-78%) and specificity (91-94%) for the diagnosis of partial-thickness tears was also higher than those of previous reports. Considering that the previous studies were conducted using 1.5-T MR scanners (40, 41), our use of a 3.0-T scanner may explain our superior results, although magic angle artifacts often made discrimination between small-sized tears and degenerative change difficult. The sensitivities (75-86%) and specificities (82-89%) in the diagnosis of SSC tendon tears in our study were higher than those of previous reports using indirect MR arthrography (11, 24).
The present study has several limitations. First, the MR images were analyzed retrospectively, and the two radiologists who evaluated the images were aware that the patients had undergone arthroscopic shoulder surgery, which may have introduced a reader bias resulting in the overestimation of rotator cuff tear diagnoses. Additionally, there may have been a patient selection bias because only patients who had undergone arthroscopic surgery were included in this study. Second, arthroscopy is operator-dependent, although it was used as the reference standard. Thus, precise evaluation of SSC tendons could be difficult and lesions of SSC tendons might be missed on imaging and arthroscopy (26, 42). Third, we cannot exclude the possibility of recall bias. Although the readers reviewed the 2D images first and the 3D images 1 month later, the detection rate with the 3D sequences might have been affected. Finally, we used only T1-weighted sequence in both techniques, which may result in confusion between tendon pathology and magic angle artifact, thus lowering the diagnostic performance. Further studies are needed for the diagnosis of rotator cuff tears with both 3D isotropic T1- and T2-weighted FSE sequences.
In conclusion, 3D isotropic T1-weighted FSE indirect MR arthrography and conventional 2D indirect MR arthrography were not significantly different in accuracy for diagnosing rotator cuff tears. Accordingly, 3D isotropic FSE imaging may have the potential to substitute for conventional 2D sequences for diagnosing rotator cuff tears if several technical improvements are achieved.






 XML Download
XML Download