

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Most pectoralis minor tendons insert into the superomedial aspect of the coracoid process (1, 2). However, in a cadaveric study, Le Double (1) described three types of attachment variations of the pectoralis minor tendon, and about 15% of the cadavers showed ectopic insertion of the pectoralis minor tendon (EIPMT) passing over the coracoid process. Since that report, several studies have found EIPMT incidence rates of 9.6-16% (1, 2, 3). However, this anatomical variation has attracted little attention from radiologists regardless of the high incidence.
The clinical significance of EIPMT remains obscure, but several studies have shown its association with subacromial or subcoracoid impingement (4, 5, 6, 7) and shoulder stiffness as in adhesive capsulitis (8). In addition, Yoo et al. (9) emphasized the importance of preoperative detection of EIPMT in patients with a rotator cuff tendon tear because it can be a possible obstacle to retract the supraspinatus tendon upon immobilization, leading to tension on the repaired tendon. Therefore, a preoperative evaluation for EIPMT could be important for patients undergoing rotator cuff tendon repair. In vivo imaging studies about this anatomical variation have been conducted in a larger population using ultrasound (US) by Homsi et al. (3) and MR arthrography by Lee et al. (10). US allows for a dynamic study to evaluate EIPMT but has disadvantages of being poorly objective and operator dependent. In turn, MR arthroscopy has an advantage to demonstrate EIPMT easily but may fail to detect partial EIPMT (a portion of the tendon has a normal insertion into the coracoid process and another portion has an anomalous insertion, Le Double type II). In addition, the extra-articular portion such as the subcoracoid area cannot be evaluated because of fat suppression. Magnetic resonance imaging (MRI) is the first-choice examination for many shoulder lesions as a noninvasive objective modality with excellent soft tissue contrast. However, MRI studies of EIPMT have only been retrospective for a few sporadic surgical and arthroscopic cases (8, 9, 11, 12).
The purpose of this study was to evaluate reproducibility of MRI to detect EIPMT. In addition, we evaluated the changes in subcoracoid soft tissue and the rotator interval in cases of EIPMT using MRI, based on the observation that most reported symptomatic EIPMT cases have been associated with impingement or shoulder stiffness (7, 8, 11).
MATERIALS AND METHODS
Subjects
Our Institutional Review Board approved this retrospective study, and informed patient consent was waived. A total of 516 consecutive MRI examinations in 508 patients were performed at our institution from April 2010 to January 2012. Eight patients underwent MRI on both shoulders. Nine of 516 shoulder MRI examinations were excluded because of severe anatomical distortion due to trauma (n = 2), tumor (n = 1), septic shoulder (n = 2), and an inappropriate scan axis for evaluating the pectoralis minor tendon because of scanning the acromioclavicular joint (n = 4). A total of 507 shoulder MRI examinations in 499 patients (male:female = 259:248, age range, 12-90 years; mean age, 55.4 years) were included in this study.
MRI was performed using a 3-T whole-body MR scanner (Achieva, Philips Healthcare, Best, The Netherlands) with a dedicated receive-only shoulder coil. Patients were positioned for imaging with the humerus in a neutral position and the thumb pointing upward. MRI was performed using the following imaging sequences. T2-weighted turbo spin echo sequences (repetition time [TR]/echo time [TE], 4325-4974/80 msec; section thickness, 2.5 mm; gap, 0.2 mm; field-of-view, 10 × 10 cm; matrix size, 512 × 512; echo-train length). Sixteen were performed in the axial plane, oblique coronal plane (parallel to the long axis of the supraspinatus tendon), and oblique sagittal plane (perpendicular to the long axis of the supraspinatus tendon). A T1-weighted turbo spin-echo sequence was performed in the oblique coronal plane (TR/TE, 500/20 msec; section thickness, 2.5 mm; gap, 0.2 mm; field-of-view, 10 × 10 cm; matrix size, 512 × 512). The spectral adiabatic inversion recovery (SPAIR) sequence was performed in the oblique coronal and oblique sagittal planes (TR/TE, 4346/65 msec; section thickness, 2.5 mm; field-of-view, 10 × 10 cm; matrix size, 512 × 512).
MRI Analysis of EIPMT
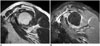
One fellow-trained musculoskeletal radiologist with 14 years experience in musculoskeletal MRI and one general radiologist with 3 years experience in musculoskeletal MRI independently examined the 507 shoulder MRIs, which they classified into 1) normal type insertion of the pectoralis minor tendon, 2) complete type, and 3) partial type EIPMT (Fig. 1). Normal type insertion of the pectoralis minor tendon was defined as insertion of the pectoralis minor tendon into the superomedial aspect of the coracoid process and lack of a connection between the coracohumoral ligament and the pectoralis minor tendon. EIPMT was defined as crossing and insertion of the tendinous structure of the pectoralis minor over the coracoid process into another site such as the anterior portion of the supraspinatus tendon, the coracohumeral ligament, or the rotator interval capsule. Complete type EIPMT was defined as crossing of the entire pectoralis minor tendon over the coracoid process without inserting into the coracoid process (Le Double type I). Partial type EIPMT was defined as normal insertion of a portion of the tendon into the coracoid process and anomalous insertion of another portion, which ran over the coracoid process (Le Double type II). T2-weighted and SPAIR oblique sagittal images were reviewed to evaluate the pectoralis minor tendon. SPAIR oblique coronal images were also reviewed if a dot-like tendon structure of the pectoralis minor continuously ran over the coracoid process. The images were reviewed independently by two blinded radiologists.
Cases in which the two radiologists did not reach the same conclusion were re-analyzed by consensus of the two reviewers. The incidence of EIPMT was calculated, and sex and arm predominance were evaluated and compared with those of previous studies.
Image Analysis of the Rotator Interval
The EIPMT cases were matched with normal control subjects to compare the MRI changes in the rotator interval and subcoracoid area between EIPMT and normal type insertion. Matching criteria were age and sex. Age- and sex-matched control subjects were chosen randomly using a random number table among the normal type insertion group.
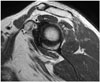
Thickness of fibrotic scar tissue was measured in the subcoracoid triangle, at the adjacent coracoid process, for the quantitative analysis (Fig. 2) and compared between the EIPMT and control subjects. Thickness was measured at the plane in which visualization of the overlying pectoralis minor tendon or coracohumeral ligament was best on the T2-weighted oblique sagittal plane. Thicknesses of the humeral capsule and synovium of the axillary recess were also measured and compared between the two groups to evaluate the association with adhesive capsulitis. Thickness of the humeral axillary recess was measured at the mid-axillary level on the T2-weighted coronal plane. The widest portion of the capsule and synovium of the axillary recess perpendicular to the adjacent cortical bone of the humeral neck was measured (Fig. 2). All measurements were performed by one blinded radiologist resident trainee with a random order of the MRIs including the EIPMT and control subjects.
The degree of fibrotic scar tissue proliferation in the subcoracoid area including the rotator interval was evaluated on the MRIs by consensus of the same radiologists, and compared between the EIPMT group and control subjects in a qualitative analysis. The degree of fibrotic scar tissue proliferation was graded according to the area occupied by fibrotic scar tissue in the rotator interval and subcoracoid area (Fig. 2A, B) on the T2-weighted oblique sagittal plane as none, mild (< 1/3), moderate (1/3-2/3), and severe (> 2/3).
Statistical Analysis
Inter-observer agreement was calculated using the kappa coefficient. Kappa coefficients were interpreted according to the guidelines of Landis and Koch (strength of agreement for the kappa coefficient: < 0 = poor; 0.01-0.2 = slight; 0.21-0.4 = fair; 0.41-0.6 = moderate; 0.61-0.8 = substantial; and 0.81-0.99 = almost perfect) (13). Significant differences in sex and arm predominance between the EIPMT and normal type insertion groups were evaluated by the χ2 test.
Student's t test (quantitative analysis) was used to compare EIPMT and control subjects, and the Mann-Whitney U-test was used between the complete and partial EIPMT groups for thicknesses of the fibrotic scar tissue in the subcoracoid fat triangle and humeral axillary recess (quantitative analysis). The degree of fibrotic scar tissue proliferation in the rotator interval (qualitative analysis) was analyzed with the χ2 test to compare the EIPMT and control subjects, and Fisher's exact test was used to compare complete and partial EIPMT. A p < 0.05 was considered significant. All statistical analyses were performed with SPSS version 18.0 for Microsoft Windows software (SPSS Inc., Chicago, IL, USA).
RESULTS
MRI Analysis of EIPMT
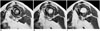
Ectopic insertion of the pectoralis minor tendon was found in 14.6% (complete type, 6.9%; partial type, 7.7%) (reviewer #1) and in 17.2% (complete type, 9.3%; partial type, 7.9%) (reviewer #2) on 507 shoulder MRIs. The inter-observer agreement for MRI detection of EIPMT was substantial (kappa value = 0.775). The incidence of EIPMT after re-analysis of discordant cases by consensus was 13.4% (n = 68) of the 507 shoulder MRIs; the incidence of normal type EIPMT was 86.6% (n = 439) (Fig. 3), that of complete type EIPMT was 7.7% (n = 39) (Fig. 4), and that of partial type EIPMT was 5.7% (n = 29) (Fig. 5). EIPMT was found in 25 of 259 (9.7%) male shoulders and 43 of 248 (17.3%) female shoulders. Female predominance was not significant (p > 0.05). EIPMT was found in 39 of 210 left shoulders (18.6%) and 29 of 297 right shoulders (9.8%). Left side predominance was significantly different (p = 0.04) (Table 1).
Image Analysis of the Rotator Interval
Thickness of the fibrotic scar tissue in the subcoracoid triangle was significantly thicker in the EIPMT group (8.6 ± 4.8 mm) than that in control subjects (4.4 ± 4.6 mm, p < 0.001) (Table 2). No significant difference in thickness of the humeral axillary recess was observed between the EIPMT (3.5 ± 1.2 cm) and control subjects (3.5 ± 1.1 cm, p > 0.05). The grade of fibrotic scar tissue proliferation in the rotator interval was also significantly higher in the EIPMT than that in control subjects (p < 0.001) (Table 3, Figs. 3, 4, 5). No significant differences were observed in the thicknesses of scar tissue in the subcoracoid fat or humeral axillary recess or the grade of fibrotic scar tissue proliferation in the rotator interval between the complete and partial type EIPMT groups (p > 0.05).
DISCUSSION
The incidence of EIPMT as assessed by MRI was 13.4% of 507 shoulders. Weinstabl et al. (2) found pectoralis minor fibers passing over the coracoid process in 16% of 126 shoulders. Our result was similar to the results in the literature (1, 2). Although our study was limited because the results were not surgically proven, we show definite imaging evidence of the pectoralis minor tendon passing over the coracoid process on 3.0-T MR. Moreover, inter-observer agreement was substantial (kappa value = 0.775). EIPMT was well demonstrated on SPAIR oblique sagittal images, as the small vessels around the coracoid process had high signal intensity. Therefore, the thin tendinous structure of the pectoralis minor tendon in the partial type EIPMT cases was differentiated with vessels passing over the coracoid process. Oblique sagittal T2-weighted and SPAIR oblique coronal images were also helpful.
According to a US study by Homsi et al. (3), the incidence of EIPMT was 9.6% in 606 shoulder joints, with left arm (12.2%) and female predominance and a female to male ratio of 2.6. Similarly, our study showed significant left arm predominance (18.6% vs. 9.8%, p = 0.004) but not significant female predominance (17.3% vs. 9.7%, p > 0.05). In a study of 505 MR arthrographic examinations by Lee et al. (10), the incidence of EIPMT was only 1.5% (five cases). In 1897, Le Double classified the variation of the superior attachment of the pectoralis minor muscle into three types. A type 1 variation occurs when the entire pectoralis minor tendon passes over the superior margin of the coracoid process to insert distally on multiple sites such as the supraspinatus tendon, the coracoacromial ligament, one of the tubercles of the humeral head, or the labrum. This type corresponded to the complete type in our study. A type 2 variation is seen when some portion of the tendon has normal insertion into the coracoid process and another portion has anomalous insertion. This type corresponded to the partial type in our study. Type 3 occurs when the muscle itself (as opposed to the tendon) inserts anomalously without attaching to the coracoid process. The reason for the low prevalence of EIPMT on MR arthrography in the study by Lee et al. (10) is unclear, but they only included cases in which MR arthrography showed contrast extension across the coracoid process along the pectoralis minor. Therefore, the partial type (Le Double type 2) may have been misdiagnosed. Among the 68 shoulders with EIPMT in our study, 39 were of the complete type and 29 were of the partial type. According to the cadaveric study of Le Double (1), the most common type is type 1, followed by types 2 and 3. Similarly, we found that the complete type was more common than the partial type, and the type 3 variation was not detected.
We started this study after gaining experience with EIPMT cases that had significant fibrotic scar tissue proliferation in the subcoracoid area and rotator interval. In our study, the patients with EIPMT had significantly thicker fibrotic scar tissue in the rotator interval adjacent to the coracoid process and a significantly higher grade of fibrotic scar tissue proliferation in the rotator interval, compared with those in sex- and age-matched control subjects. Although the correlation between clinical symptoms and this variation was not evaluated in this study, this pathological change may cause shoulder pain or tightness as observed in cases of adhesive capsulitis. However, no significant difference was observed in the thickness of the humeral axillary recess between patients with EIPMT and the control group. According to MRI studies on adhesive capsulitis, thickening of the capsule and synovium in the humeral axillary recess and fibrotic scar tissue proliferation in the rotator interval are characteristic findings of adhesive capsulitis (14, 15). In our study, EIPMT resulted in significant fibrotic scar changes in the rotator interval compared with that in control subjects, but the thicknesses of the synovium and the humeral axillary recess capsule were not different. This result indicates that EIPMT may cause scar changes around the coracoid process including the rotator interval and may have a different pathological or physiological mechanism than cases of adhesive capsulitis. The assumption about fibrotic scar tissue proliferation in the rotator interval of EIPMT cases is that the overlying tendon running on top of the coracoid process could cause friction against the coracoid process or structures in the rotator interval during motion. This variation might not be detected in an arthroscopic examination or surgery, as the ectopic tendon itself could be mixed up with the fibrotic scar tissue in the rotator interval.
This study had several limitations. First, our study group consisted of patients who underwent shoulder MRI examinations at our institution only. This may have created selection bias to represent the general population, because most of the patients referred for MRI have shoulder pain or discomfort and may have had other pathological findings. Second, our MRI findings were not confirmed surgically. Therefore, fibrovascular changes in the rotator interval and subcoracoid fat could not be correlated with surgical findings. Third, the relationships between other pathological findings such as a labral tear or rotator cuff tendinopathy and this variation were not evaluated. The clinical symptoms of the patients were not evaluated either. Therefore, further studies are required to establish the relationship between EIPMT and clinical symptoms.
In conclusion, EIPMT is a common variation, with a MRI incidence of 13.4%. MRI allows for reproducible detection of this anatomical variation. Although the clinical significance of this variation has not been clearly established, our results show a high tendency for fibrotic scar tissue proliferation in the rotator interval in patients with EIPMT. Radiologists should be aware of this variation and changes in the rotator interval for a diagnosis of adhesive capsulitis and during preoperative evaluation of rotator cuff tendon tears. Further studies are required to evaluate the relationships between this anomaly and clinical manifestations.





 XML Download
XML Download